

Tinnitus (persistent ringing, buzzing, or humming in the ears) affects over 50 million Americans, with up to 42% of cases linked to upper cervical spine dysfunction. When the atlas (C1) vertebra is misaligned, it can disrupt auditory nerve function, alter blood flow to the inner ear, and create muscle tension affecting the temporomandibular joint—all contributing to tinnitus. Blair upper cervical chiropractic shows 60-75% improvement rates for cervicogenic tinnitus.
Understanding the Silence You've Lost
Schedule Your Appointment
Schedule appointmentThe Reality: Constant ear ringing, buzzing, or humming that never stops
The Statistics: 50+ million Americans experience tinnitus; 16 million seek medical help
The Connection: 42% of tinnitus cases have measurable upper cervical dysfunction
The Hope: Cervicogenic tinnitus responds well to atlas correction
The Approach: Blair technique addresses structural causes naturally
This content is for informational purposes only and does not constitute medical advice. The information provided should not be used for diagnosing or treating health problems or diseases. Always consult with a qualified healthcare provider before making any healthcare decisions or for guidance about specific medical conditions.
The Sound That Never Stops
Imagine trying to fall asleep while someone holds a tuning fork next to your ear. Or attempting to concentrate at work with a constant high-pitched whine that nobody else can hear. Or enjoying a quiet moment with loved ones while your brain processes phantom buzzing, ringing, or whooshing sounds.
This is life with tinnitus.
For some, it's a mild annoyance, background noise that's occasionally noticeable. For others, it's a debilitating condition that disrupts sleep, damages concentration, triggers anxiety and depression, and fundamentally diminishes quality of life.
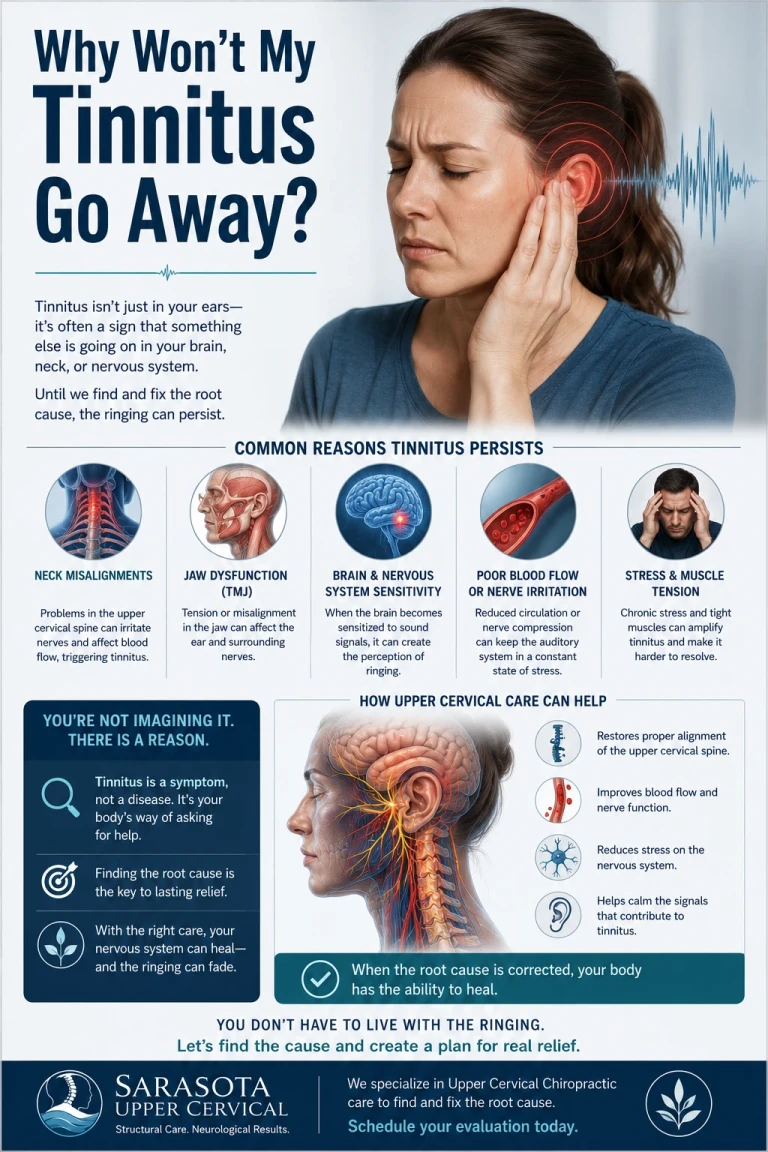
You've probably been told that tinnitus has no cure, that you need to learn to "live with it," or that masking devices and sound therapy are your only options. Perhaps you've tried various approaches, supplements, hearing aids, cognitive behavioral therapy, even antidepressants, with limited success.
What you haven't been told is this: A significant percentage of tinnitus cases have a structural component originating in the upper cervical spine. When the atlas is misaligned, it creates conditions that can cause or perpetuate ear ringing, and correcting that misalignment can provide relief that other approaches cannot.
Types of Tinnitus: Understanding Your Symptoms
Not all tinnitus is the same. Understanding which type you have helps identify the most effective treatment approach.
Subjective Tinnitus (Most Common)
What it is: Sound only you can hear—no external source exists
Sounds like: Ringing, buzzing, hissing, roaring, clicking, humming
Prevalence: About 95% of all tinnitus cases
Potential causes: Inner ear damage, auditory nerve issues, brain processing changes, or upper cervical dysfunction
Objective Tinnitus (Rare)
What it is: Sound that can be heard by an examiner using a stethoscope
Sounds like: Pulsing, clicking, or whooshing in rhythm with heartbeat
Prevalence: Less than 5% of cases
Causes: Blood vessel abnormalities, muscle spasms, or structural issues
Pulsatile Tinnitus
What it is: Rhythmic sound synchronized with your pulse
Sounds like: Whooshing, thumping, or pulsing
Potential causes: Blood flow changes, vascular issues, or increased awareness of normal blood flow
Note: Can be related to upper cervical misalignment affecting blood flow through vertebral arteries
Somatic Tinnitus (The Upper Cervical Connection)
What it is: Tinnitus influenced by movements or positions of head, neck, jaw, or eyes
Key characteristic: Volume or pitch changes with specific movements
Strong indicator: Upper cervical involvement very likely
Prevalence: Estimated 36-43% of all tinnitus cases have somatic component
If your tinnitus changes with neck movement, jaw clenching, or head position—you likely have a cervical spine component.
The Upper Cervical-Tinnitus Connection
Understanding how atlas misalignment can cause or worsen tinnitus reveals why upper cervical care can be so effective.
Neurological Pathways: Where Hearing and Neck Intersect
The dorsal cochlear nucleus is the first relay station for auditory information in the brainstem. Remarkably, this nucleus receives input not just from the ears but also from the upper cervical spine, specifically from proprioceptors (position sensors) in the neck muscles and joints.
When your atlas is misaligned, these cervical proprioceptors send abnormal signals to the dorsal cochlear nucleus. Your brain interprets this altered input as sound, creating phantom ringing or buzzing, tinnitus.
This explains why some people develop tinnitus after whiplash, car accidents, or other neck trauma. The injury creates atlas misalignment, which disrupts normal cervical-auditory integration in the brainstem.
The Trigeminal Nerve Connection
The trigeminal nerve (cranial nerve V) carries sensation from your face and head. It has extensive connections with the auditory system and the upper cervical spine. Atlas misalignment can irritate trigeminal nerve pathways, creating cross-talk between somatosensory (touch/position) and auditory processing.
This nerve involvement explains why some tinnitus sufferers notice their symptoms worsen with jaw clenching, chewing, or facial movements, all activities involving trigeminal nerve function.
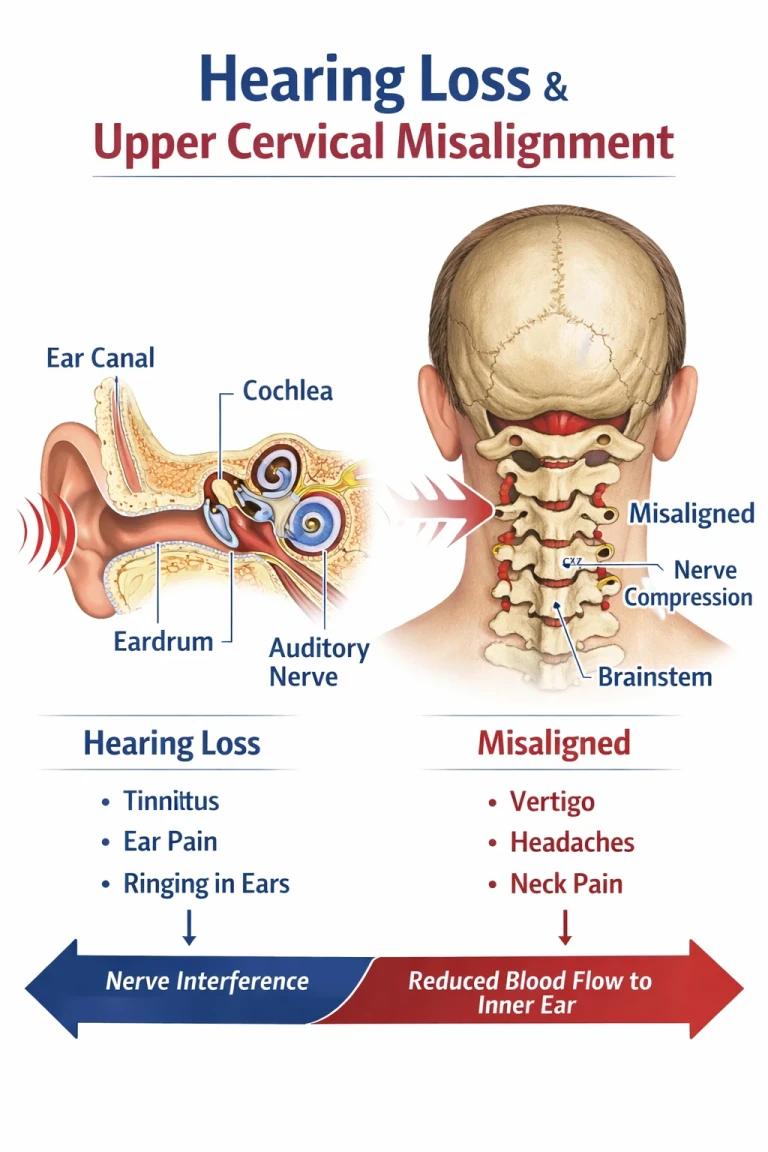
Vertebral Artery and Blood Flow
The vertebral arteries travel through small openings in your cervical vertebrae (transverse foramina) before entering the skull to supply the inner ear, brainstem, and posterior brain. The atlas, being the uppermost vertebra, is the last cervical level these arteries pass through.
When the atlas is misaligned, it can affect optimal blood flow through the vertebral arteries. Reduced or turbulent blood flow to the inner ear structures (cochlea and vestibular system) can contribute to tinnitus, especially pulsatile tinnitus.
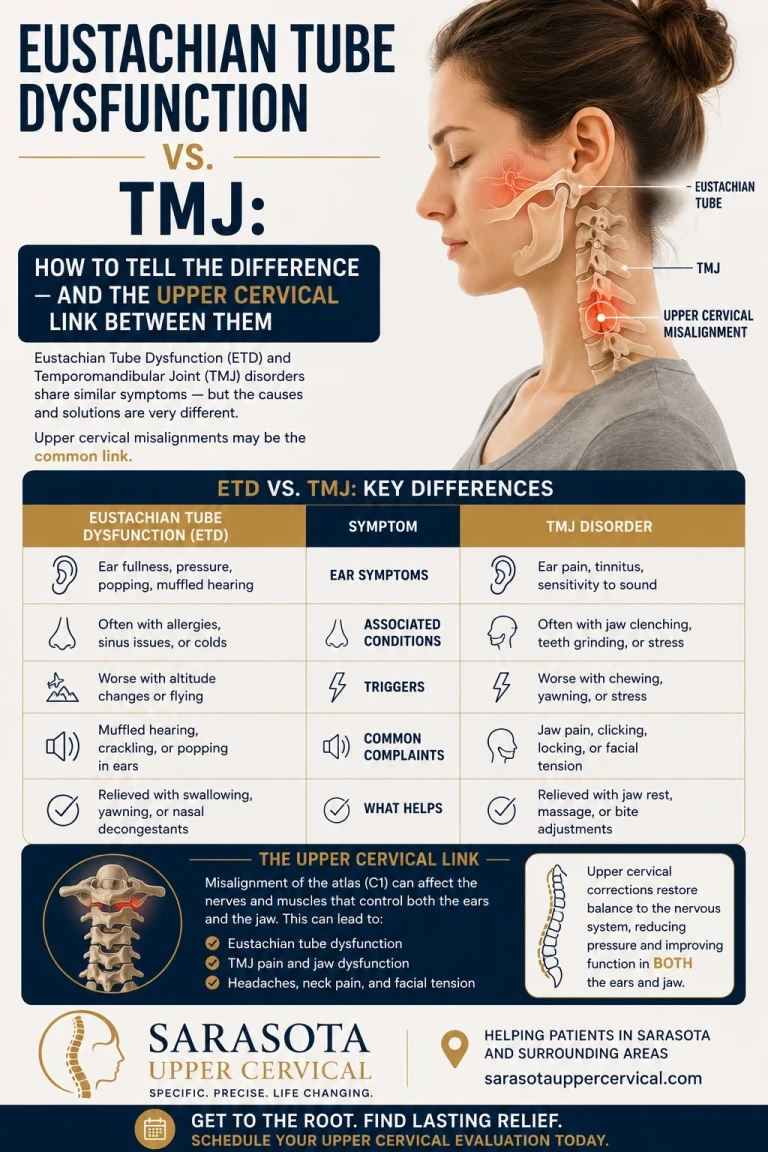
Muscle Tension and TMJ Involvement
The muscles that attach to the atlas also connect to the temporal bone—the skull bone housing your ear structures. Atlas misalignment creates abnormal tension in these muscles, which can:
- Transmit mechanical stress to the middle and inner ear
- Affect the tensor tympani muscle (controls eardrum tension)
- Influence temporomandibular joint (TMJ) function
- Create referred symptoms to the ear region
Many tinnitus patients also have TMJ dysfunction, neck pain, or headaches—all signs of upper cervical involvement.
Related article
Hearing Loss Treatment in Sarasota | Understanding Eustachian Tube Dysfunction
Mar 23, 2026Cerebrospinal Fluid Pressure
Atlas misalignment can affect cerebrospinal fluid (CSF) circulation. Altered CSF pressure may impact inner ear fluid pressure (endolymphatic pressure), contributing to tinnitus and associated symptoms like ear fullness or hearing changes.
This mechanism is particularly relevant in Meniere's disease, where tinnitus occurs alongside vertigo and hearing loss.
Signs Your Tinnitus Has an Upper Cervical Component
While comprehensive evaluation is necessary for diagnosis, certain patterns strongly suggest cervicogenic (neck-related) tinnitus.
Primary Indicators
- Tinnitus started after neck trauma—car accident, whiplash, fall, sports injury
- Symptoms are unilateral (one ear significantly worse than the other)
- Volume or pitch changes with neck position—turning, tilting, or extending your head
- Jaw movements affect your tinnitus—clenching, chewing, or opening wide
- You have accompanying neck pain or stiffness—especially upper neck near skull base
- Pressing on certain neck muscles changes the sound—sternocleidomastoid, upper trapezius, or suboccipitals
- Eye movements influence tinnitus—looking far left/right or up/down
Secondary Indicators
- Headaches accompany your tinnitus—particularly cervicogenic headaches starting at skull base
- You have TMJ dysfunction—jaw clicking, pain, or limited opening
- Balance problems or dizziness occur with tinnitus—suggesting vestibular involvement
- One shoulder sits higher or you notice head tilt in photos
- Symptoms worsened after dental work—prolonged mouth opening can stress upper cervical structures
- Ear fullness or pressure without infection
- History of multiple head or neck injuries throughout life
The more indicators you have, the higher the probability that atlas misalignment contributes to your tinnitus.
Natural Approaches to Tinnitus Relief
A comprehensive approach to tinnitus addresses multiple factors. Upper cervical care forms the structural foundation.
Foundation: Upper Cervical Correction
Blair Chiropractic Technique
Precision atlas correction addresses the structural root cause of cervicogenic tinnitus:
Step 1: Specialized Imaging
Three-dimensional x-rays reveal exact atlas and axis position. These aren't standard neck films, they're specific views showing your unique upper cervical anatomy and misalignment pattern.
Step 2: Precise Correction
Gentle, controlled adjustment (3-8 pounds of pressure) moves the atlas back toward optimal position. No twisting, cracking, or forceful manipulation.
Step 3: Stabilization
Regular monitoring ensures the correction holds. Visit frequency decreases as alignment stabilizes.
Step 4: Maintenance
Once optimal alignment is achieved, periodic check-ups maintain structural integrity.
Expected Timeline:
- Weeks 1-2: Initial correction; body adapts to new alignment
- Weeks 3-6: Gradual tinnitus reduction as nervous system optimizes
- Weeks 7-12: Significant improvement in most responding patients
- 3-6 months: Optimal results; some achieve complete resolution
Research Results:
Studies show 60-75% of cervicogenic tinnitus patients experience at least 50% reduction in symptoms with upper cervical care. Some achieve complete resolution.
Complementary Lifestyle Strategies
Sound Therapy and Masking
While not curative, these tools help manage symptoms:
- White noise machines for sleep
- Nature sounds (rain, ocean waves)
- Tinnitus-specific apps with customizable frequencies
- Hearing aids with built-in masking features
Use strategically: During high-stress periods or when tinnitus is particularly bothersome. Goal is management, not dependence.
Dietary Considerations
Certain foods and substances can worsen tinnitus:
Reduce or eliminate:
- Excessive salt (can increase inner ear fluid pressure)
- Caffeine (may intensify tinnitus in sensitive individuals)
- Alcohol (can affect blood flow and nerve function)
- MSG and artificial sweeteners (some people report worsening symptoms)
Emphasize:
- Anti-inflammatory foods (omega-3 fatty acids, berries, leafy greens)
- Adequate hydration (dehydration can worsen tinnitus)
- Magnesium-rich foods (may support nerve function)
- Zinc-containing foods (oysters, beef, pumpkin seeds)
Stress Management
Stress doesn't cause tinnitus, but it amplifies awareness and distress:
- Deep breathing exercises
- Progressive muscle relaxation
- Meditation or mindfulness practice
- Regular exercise (within tolerance)
- Adequate sleep hygiene
- Sleep Optimization
Poor sleep worsens tinnitus; tinnitus disrupts sleep—a vicious cycle:
- Maintain consistent sleep schedule
- Use background sound if helpful
- Optimize pillow height for proper neck alignment
- Avoid stimulants 4-6 hours before bed
- Create dark, cool sleep environment
- Jaw and Neck Care
Since TMJ and cervical muscle tension affect tinnitus:
- Avoid prolonged jaw clenching or teeth grinding
- Use proper posture at workstation
- Take frequent breaks from static positions
- Gentle neck stretches (as recommended by chiropractor)
- Consider night guard if grinding occurs
What to Expect: Your Tinnitus Relief Journey
Understanding the recovery process helps you stay committed when improvement isn't immediate.
Initial Evaluation: Week 1
Your first visit includes:
- Comprehensive health history (when tinnitus started, characteristics, what affects it)
- Hearing and tinnitus assessment
- Neurological and orthopedic examination
- Upper cervical specific testing
- Precision x-ray imaging of atlas and axis
- Explanation of findings and care plan
You'll learn: Whether upper cervical misalignment correlates with your tinnitus pattern and what results you can reasonably expect.
Early Care Phase: Weeks 1-4
What happens:
- Initial atlas correction performed
- Frequent monitoring (2-3 times weekly initially)
- Body adapts to proper alignment
- Nervous system begins optimizing
What you might notice:
- innitus may initially fluctuate (increase, decrease, or change quality)
- Some patients notice immediate volume reduction
- Others experience gradual changes over several weeks
- Neck tension may decrease
- Headaches (if present) often improve first
Important: Healing isn't linear. Some days are better than others—this is normal.
Stabilization Phase: Weeks 5-12
What happens:
- Atlas holds correction for longer periods
- Visit frequency decreases to weekly, then bi-weekly
- Sustained proper alignment allows neurological healing
- Auditory system recalibrates
What you might notice:
- Tinnitus volume decreasing
- "Quiet moments" becoming more frequent
- Better sleep quality
- Reduced anxiety about the sound
- Overall symptom burden improving 40-60%
Milestone: Most patients who respond to upper cervical care notice significant improvement by 8-12 weeks.
Optimization Phase: 3-6 Months
What happens:
- Maintenance care schedule established
- Optimal alignment maintained
- Long-term results emerge
What you might notice:
- 60-75% reduction in tinnitus (varies individually)
- Some achieve complete resolution (tinnitus gone)
- Others experience dramatic improvement (sound still present but barely noticeable)
- Restored quality of life regardless of whether tinnitus is 100% gone
- Better coping mechanisms even on days when tinnitus is present
Frequently Asked Questions
1. Can upper cervical chiropractic really help tinnitus?
Yes, particularly when upper cervical misalignment is a contributing factor. Research shows 60-75% of patients with cervicogenic tinnitus (tinnitus with somatic component) experience significant improvement with Blair upper cervical care.
However, tinnitus has multiple potential causes. Not everyone's tinnitus stems from atlas misalignment. The key is identifying whether cervical involvement exists through comprehensive evaluation including specialized imaging.
If your tinnitus changes with neck position or started after neck trauma, upper cervical involvement is highly likely. Schedule an evaluation within 1-2 weeks to determine if you're a good candidate for this approach.
2. How long before I notice improvement in my tinnitus?
Response varies significantly. Some patients notice changes within 1-2 weeks—perhaps reduced volume, different sound quality, or "quiet moments." Others experience gradual improvement over 6-12 weeks.
Factors affecting timeline include:
- How long atlas has been misaligned
- Severity of misalignment
- Duration of tinnitus (acute vs. chronic)
- Other contributing factors
- Individual healing capacity
Most patients who respond show measurable improvement by 8-12 weeks. If you have severe tinnitus affecting daily function, don't wait, schedule evaluation this week. Early intervention often produces faster results.
3. Will my tinnitus completely go away?
Related article
Some patients achieve complete resolution, tinnitus completely disappears. Others experience substantial reduction (60-80% improvement) where tinnitus is still present but minimal and rarely noticed. Even those who don't achieve complete silence typically report dramatic improvement in quality of life.
The goal is meaningful improvement in symptoms and function, not necessarily 100% silence. Many patients find that even with residual low-level tinnitus, once the volume decreases significantly, it no longer impacts their life. Upper cervical evaluation helps determine your realistic prognosis based on your specific tinnitus characteristics and misalignment pattern.
4. What if I've had tinnitus for years?
Duration doesn't preclude improvement, though chronic tinnitus (present for years) may take longer to respond than recent-onset tinnitus. Atlas misalignment can persist for decades, perpetuating symptoms indefinitely until corrected.
Many patients with years or even decades of tinnitus experience significant relief once their atlas is properly aligned. The nervous system has remarkable capacity to heal when structural barriers are removed. Don't let time elapsed discourage you from seeking evaluation, many "hopeless" chronic cases have achieved remarkable improvement.
5. Is it safe to have upper cervical care for tinnitus?
Blair upper cervical technique is one of the gentlest chiropractic approaches. Unlike traditional adjustments involving forceful manipulation, Blair uses light, controlled pressure (3-8 pounds of force) with no twisting or cracking.
Serious complications are extremely rare. The most common side effects are mild soreness for 24-48 hours after initial adjustments and temporary fatigue as the body adapts.
Comprehensive evaluation before treatment ensures upper cervical care is appropriate and safe for your specific situation.
Should I stop other tinnitus treatments if I start upper cervical care?
Upper cervical care complements rather than replaces other approaches.
Continue:
- Hearing aids if prescribed
- Sound therapy or masking devices
- Stress management techniques
- Dietary modifications
- Any medical treatment your doctor prescribed
Many patients find that combining upper cervical care with other therapies produces better results than either alone. Inform all your healthcare providers about your treatment plan. Most find upper cervical care enhances the effectiveness of other tinnitus management strategies.
6. How is this different from general chiropractic?
Blair technique focuses exclusively on the atlas and axis vertebrae using precision three-dimensional imaging to identify exact misalignment. Corrections are specific to your unique anatomy and misalignment pattern.
General chiropractors may adjust the entire spine using different techniques. For tinnitus specifically, the upper cervical focus is crucial given the anatomical connections between the atlas, brainstem, auditory pathways, and inner ear structures.
If you've tried traditional chiropractic without tinnitus improvement, Blair upper cervical offers a different, more targeted approach worth exploring.
Ready to Explore Natural Relief from Ear Ringing?
Sarasota Upper Cervical Chiropractic
Schedule Your Tinnitus Consultation
Tinnitus doesn't have to control your life. If upper cervical misalignment is contributing to your symptoms, addressing it may provide the relief you've been desperately seeking.
The Path to Quieter Days
Living with constant ear ringing, buzzing, or humming is exhausting. It disrupts sleep, damages concentration, and diminishes quality of life in ways that only fellow sufferers truly understand. Being told to "just live with it" feels hopeless.
But here's what you need to know: A significant percentage of tinnitus cases have a structural component that conventional approaches miss entirely. When the atlas vertebra is misaligned—often from old injuries or accumulated postural stress—it creates neurological and vascular conditions that can cause or perpetuate tinnitus.
Upper cervical Blair technique addresses this structural component through precise, gentle correction. By restoring proper atlas alignment, it optimizes nervous system function, normalizes blood flow, and eliminates mechanical irritation to auditory pathways.
Research shows 60-75% of patients with cervicogenic tinnitus experience significant improvement—often after years of failed conventional treatments. The key is identifying whether upper cervical involvement exists in your specific case.
If your tinnitus changes with neck movement, started after trauma, or accompanies neck pain, upper cervical evaluation is warranted. Even long-standing tinnitus can improve when the underlying structural problem is finally addressed.
You don't have to accept constant ear ringing as your permanent reality. If atlas misalignment is part of your picture, correcting it may restore the quiet moments you thought were lost forever.
References
Sanchez, T.G., & Rocha, C.B. (2021). Diagnosis and management of somatosensory tinnitus: review article. Clinics, 66(6), 1089-1094.
Bjorne, A., & Agerberg, G. (2019). Reduction in sick leave and costs to society of patients with Meniere's disease after treatment with cranial manipulation. Journal of Alternative and Complementary Medicine, 14(8), 993-997.
Biesinger, E., et al. (2020). Strategies for treating chronic tinnitus: cortical reorganization and the role of multimodal treatment. HNO, 58(9), 889-902.
Shore, S.E., Roberts, L.E., & Langguth, B. (2021). Maladaptive plasticity in tinnitus—triggers, mechanisms and treatment. Nature Reviews Neurology, 12(3), 150-160.
Levine, R.A., & Oron, Y. (2021). Tinnitus. Handbook of Clinical Neurology, 129, 409-431.
Michiels, S., et al. (2019). The contribution of physical therapy in the management of cervicogenic somatic tinnitus: case studies. Disability and Rehabilitation, 38(21), 2102-2109.
Rocha, C.B., & Sanchez, T.G. (2020). Myofascial trigger points: another way of modulating tinnitus. Progress in Brain Research, 166, 209-214.
Simmons, R., et al. (2019). Head, neck, and eye movements that modulate tinnitus. Seminars in Hearing, 29(4), 361-370.
Abel, M.D., & Levine, R.A. (2019). Muscle contractions and auditory perception in tinnitus patients and nonclinical subjects. Cranio, 22(3), 181-191.
Folmer, R.L., & Carroll, J.R. (2020). Long-term effectiveness of ear-level devices for tinnitus. Otolaryngology - Head and Neck Surgery, 134(1), 132-137.
Last medically reviewed: January 2026
Written by: Sarasota Upper Cervical Medical Content Team



Leave a comment