
"The Eustachian tube mucosa relies on autonomic regulation for normal function. Understanding the cervical autonomic anatomy clarifies why upper cervical structural problems may contribute to mucosal dysfunction and Eustachian tube dysfunction in appropriate patients — and where the evidence supports versus where it does not"
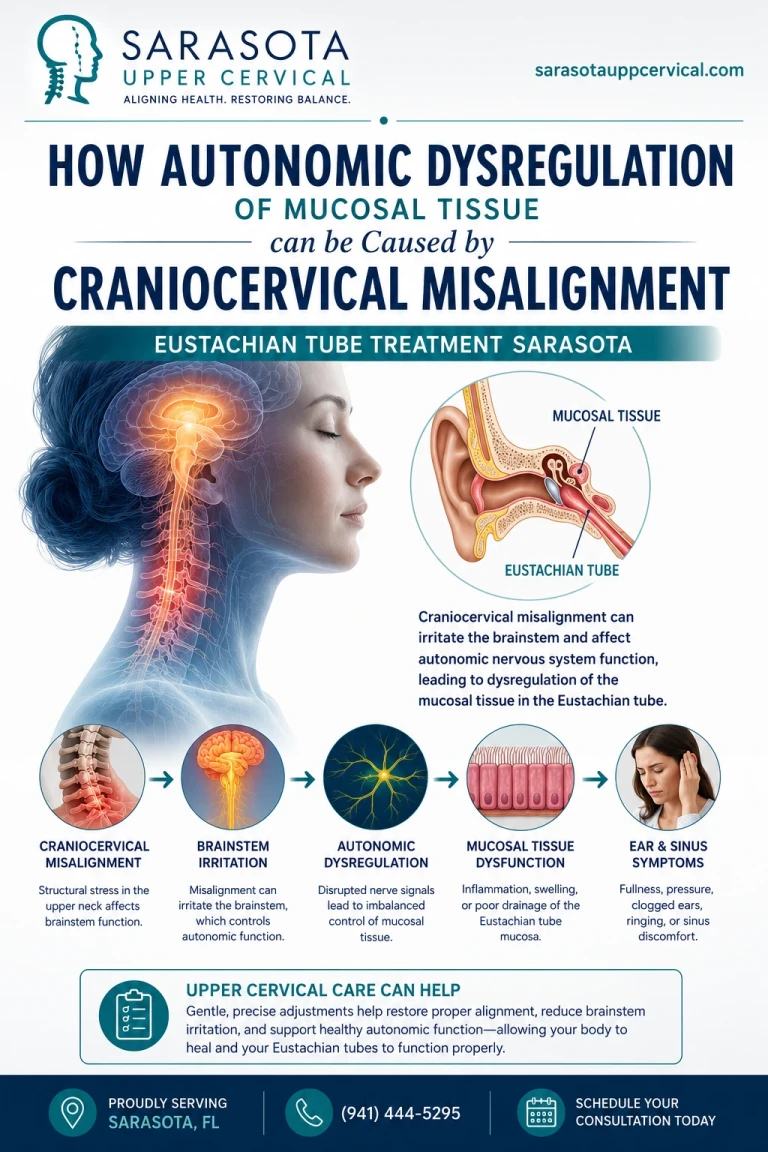
The Eustachian tube does not function in isolation. Its ability to open and close appropriately, to drain middle ear secretions, to equalize pressure changes, and to maintain normal middle ear physiology all depend on healthy mucosal tissue — the lining that covers the tube's interior and surrounds its opening. The mucosal tissue is not passive plumbing; it is actively regulated by the autonomic nervous system, with sympathetic and parasympathetic input controlling vascular tone, secretion patterns, swelling responses, and overall tissue characteristics. When this autonomic regulation is disrupted, mucosal dysfunction can follow, and the consequences for Eustachian tube function can be substantial.
Patients with persistent Eustachian tube dysfunction sometimes have underlying autonomic dysregulation contributing to their condition. Standard medical treatments — decongestants, antihistamines, nasal corticosteroids, allergy management — address the mucosal inflammation and congestion that often accompanies ETD, but for some patients these treatments produce only partial improvement. Understanding what controls mucosal function autonomically opens consideration of factors that may be contributing beyond what standard treatments directly address. The cervical autonomic anatomy — the cervical sympathetic chain and its relationship to upper cervical structures — provides one such consideration.
This article walks through the autonomic innervation of mucosal tissue including the Eustachian tube mucosa, the role of the cervical sympathetic chain in mucosal regulation, how structural problems in the upper cervical region can potentially affect autonomic function, what this means for patients with persistent Eustachian tube dysfunction, the honest framing of the evidence supporting this framework, and when upper cervical evaluation may be worth considering as part of comprehensive ETD care alongside continued standard medical management.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The Autonomic Regulation of Mucosal Tissue
Mucosal tissue throughout the body — including the lining of the respiratory tract, the gut, the urinary tract, and the Eustachian tube — receives extensive autonomic innervation that controls its moment-to-moment function. Understanding what the autonomic system does at the mucosal level clarifies why disruption can have substantial consequences.
Sympathetic innervation and mucosal function
Sympathetic innervation reaches mucosal tissue through postganglionic fibers originating in the sympathetic chain. For the upper respiratory tract including the Eustachian tube, this innervation comes primarily through the cervical sympathetic chain — specifically the superior cervical ganglion, which provides sympathetic fibers to the head and neck. The sympathetic effects on mucosa include vasoconstriction of mucosal blood vessels, reduced mucosal secretions, and reduced tissue swelling. When sympathetic input is appropriate, mucosal vasculature operates within a balanced range that supports normal tissue function.
Parasympathetic innervation and mucosal function
Parasympathetic innervation reaches the upper respiratory mucosa primarily through the glossopharyngeal nerve (CN IX) and other parasympathetic pathways. The parasympathetic effects generally oppose the sympathetic effects — vasodilation of mucosal vessels, increased mucosal secretions, and increased tissue activity. Normal mucosal function requires balanced parasympathetic and sympathetic input, with the balance shifting appropriately based on physiological demands.
The balance and its consequences
Normal mucosal function requires the autonomic system to maintain appropriate balance between sympathetic and parasympathetic input. When the balance shifts inappropriately in one direction, mucosal dysfunction can follow. Excessive sympathetic activity can produce dryness, reduced secretions, and inadequate mucosal protection. Excessive parasympathetic activity or inadequate sympathetic activity can produce mucosal congestion, increased secretions, and swelling. For tissues like the Eustachian tube mucosa where physical dimensions matter for function (the tube needs to open and close appropriately), even modest swelling can substantially impair function.
Why this matters for the Eustachian tube
The Eustachian tube depends on its mucosal lining functioning normally. Mucosal swelling reduces the lumen of the tube, impairing the ability to open during swallowing or yawning. Mucosal congestion can produce a sense of fullness or pressure. Altered secretions affect drainage from the middle ear. The mucosa around the tube opening at the back of the nose (the torus tubarius and surrounding tissue) also matters for tube function. Autonomic dysregulation affecting any of these regions can contribute to Eustachian tube dysfunction symptoms.
The Cervical Sympathetic Chain and Its Relationship to Upper Cervical Structures
The autonomic innervation of upper respiratory mucosa comes primarily from the cervical sympathetic chain, which has specific anatomical relationships to the upper cervical structures. Understanding this anatomy clarifies where cervical structural problems could potentially affect mucosal autonomic regulation.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Anatomy of the cervical sympathetic chain
The cervical sympathetic chain runs along the cervical spine, providing sympathetic innervation to the head, neck, and upper body. The chain contains three sympathetic ganglia — the superior cervical ganglion (the largest, located near the upper cervical structures at the level of C2-C3), the middle cervical ganglion (smaller, at C6-C7 level), and the cervicothoracic or stellate ganglion (at the C7-T1 level). The superior cervical ganglion is the source of sympathetic innervation to the head, including the upper respiratory mucosa and the Eustachian tube region.
Proximity to upper cervical structures
The superior cervical ganglion sits in close proximity to the upper cervical structures — the axis (C2) and surrounding tissues. The ganglion is positioned anterior to the cervical spine, between the carotid sheath and the longus capitis muscle. The anatomical relationship means that structural problems in the upper cervical region can potentially affect the ganglion's environment through several mechanisms — mechanical pressure changes from structural displacement, altered blood flow in the surrounding vasculature, altered cerebrospinal fluid dynamics that affect the tissue environment, and altered proprioceptive input that may influence central autonomic regulation.
Sympathetic pathways to the head
Postganglionic fibers from the superior cervical ganglion follow several pathways to reach their target tissues. The internal carotid plexus follows the internal carotid artery into the cranium, providing sympathetic innervation to intracranial structures. The external carotid plexus follows the external carotid artery and its branches, providing sympathetic innervation to facial structures, the upper respiratory mucosa, and the nasopharynx including the Eustachian tube opening area. These pathways carry the sympathetic signals that affect mucosal vasculature and function.
Vagal pathways through the cervical region
While the focus here is on sympathetic innervation, the vagus nerve (CN X) also passes through the cervical region carrying parasympathetic fibers to many regions. The vagus runs within the carotid sheath and traverses the cervical region as it travels from the brainstem to its peripheral targets. The vagus does not directly innervate the Eustachian tube mucosa in the same way as the cervical sympathetic chain does, but the cervical anatomical relationships are part of the broader autonomic framework operating through the cervical region.
Central autonomic influence
Beyond the direct peripheral autonomic pathways, the upper cervical region provides proprioceptive input to brainstem autonomic regulatory centers. The deep suboccipital muscles and joint capsules send dense proprioceptive signals to the brainstem, including connections to regions involved in autonomic regulation (Gdowski & McCrea, 2000; Kulkarni et al., 2001). Distorted proprioceptive input from upper cervical structural problems can potentially influence central autonomic processing, providing another pathway by which cervical issues may affect autonomic function broadly, including mucosal regulation.
How Craniocervical Misalignment May Affect Mucosal Autonomic Function
With the anatomy of the cervical sympathetic chain and its relationship to upper cervical structures established, the proposed mechanisms by which upper cervical structural problems could affect mucosal autonomic function become clearer. Understanding the proposed mechanisms — while maintaining honest framing about the evidence supporting them — helps clarify what upper cervical evaluation may or may not offer for patients with mucosal dysfunction.
Direct effects on the sympathetic chain
Structural misalignment of the upper cervical region — particularly involving the atlas (C1) and axis (C2) — may affect the immediate environment of the superior cervical ganglion. Mechanical effects from altered tissue tensions, vascular effects from altered blood flow patterns, and inflammatory effects from chronic tissue stress could potentially affect ganglion function. These effects, if present, would alter the sympathetic output to the head and neck including the mucosal innervation.
Effects through craniocervical hydrodynamics
Michael Flanagan's 2015 paper in Neurology Research International described the craniocervical junction as a potential choke point for craniospinal hydrodynamics (Flanagan, 2015). Venous drainage from the head, cerebrospinal fluid circulation, and the mechanical environment around brainstem structures can all be affected by misalignment at this level. For autonomic function, altered hydrodynamics could potentially affect the brainstem regions involved in autonomic regulation, providing an indirect pathway by which structural cervical problems might influence mucosal autonomic function.
Effects through proprioceptive input to central autonomic centers
Distorted proprioceptive input from upper cervical structural problems feeds into brainstem regions including those involved in autonomic regulation. The brainstem autonomic centers — including the nucleus tractus solitarius, rostral ventrolateral medulla, and other regions — integrate multiple inputs to produce autonomic responses. Distorted input from the upper cervical proprioceptors may influence this integration, potentially affecting the autonomic output that regulates mucosal function throughout the head and neck region.
Effects on local vascular function
Beyond the direct autonomic pathway effects, upper cervical structural problems may affect local vascular function in the region. Altered venous drainage, altered arterial flow patterns, and altered tissue perfusion can all potentially affect the local environment in which the autonomic structures and their target tissues operate. These local effects could compound any direct autonomic dysregulation, producing the broader pattern of mucosal dysfunction.
The combined effect on mucosal function
If these mechanisms operate in a given patient, the combined effect on mucosal function could be substantial. Reduced sympathetic input would tend to produce mucosal congestion (less vasoconstriction, more parasympathetic dominance). Altered proprioceptive feedback could disrupt the balanced autonomic regulation that maintains normal mucosal function. The combined effects would manifest as the kinds of mucosal dysfunction that contribute to Eustachian tube dysfunction — mucosal swelling, altered secretions, and impaired tube function.
Honest Framing of the Evidence
Patients considering upper cervical evaluation for Eustachian tube dysfunction or mucosal-related concerns should understand the evidence landscape clearly. The case for cervical involvement is based primarily on anatomical and physiological reasoning rather than on randomized controlled trial evidence.
What is established
The autonomic innervation of mucosal tissue is established anatomy and physiology. The cervical sympathetic chain's role in providing sympathetic innervation to the head and upper respiratory mucosa is established. The proximity of the superior cervical ganglion to upper cervical structures is established. The proprioceptive input from the upper cervical region to brainstem autonomic centers is established. These anatomical and physiological foundations are not in question.
What is not established at the trial level
What has not been established through randomized controlled trials is the clinical impact of upper cervical chiropractic care specifically on mucosal autonomic dysregulation or on Eustachian tube dysfunction. The proposed mechanisms by which cervical structural problems could affect mucosal autonomic function are reasoning-based — anatomically and physiologically plausible but not definitively demonstrated as significant clinical contributors. No RCTs specifically test upper cervical chiropractic as treatment for ETD or for mucosal autonomic dysregulation.
What this means for patient decisions
Patients considering upper cervical evaluation in the context of persistent Eustachian tube dysfunction should understand that the evaluation represents a hypothesis-driven consideration based on anatomical reasoning rather than an established treatment supported by formal clinical research. The evaluation may be reasonable for appropriate patients — those with persistent ETD not responding to standard treatments, those with concurrent cervical symptoms, those with trauma history affecting both regions — but should be pursued with realistic expectations and alongside continued standard medical management.
When Upper Cervical Evaluation May Be Appropriate
Upper cervical evaluation is not appropriate for every patient with Eustachian tube dysfunction. Identifying the specific subsets where the evaluation may be reasonable to consider helps patients make informed decisions about pursuing it.
Persistent ETD not responding to standard treatment
Patients whose Eustachian tube dysfunction has not responded adequately to standard medical management — addressing allergies and environmental triggers, optimizing nasal corticosteroids, treating any underlying sinusitis, considering pressure equalization devices when appropriate, and other evidence-based ETD treatments — may consider additional approaches alongside continued standard care. For these patients, upper cervical evaluation can be one component of comprehensive evaluation rather than a replacement for the standard treatments.
Concurrent cervical symptoms
Patients with persistent ETD who also have cervical symptoms (chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern) may have layered presentations where cervical structural problems contribute to the broader picture. The cervical evaluation in these cases addresses one specific potential contributor that the standard ETD treatments do not target.
Post-traumatic ETD
ETD that developed after head or neck trauma — concussion, whiplash, fall, sports injury — may involve cervical structural injury alongside the inner ear or Eustachian tube effects. A 2005 study by Kaale and colleagues in the Journal of Neurotrauma documented upper cervical ligamentous injuries from whiplash mechanisms (Kaale et al., 2005). When trauma was sufficient to affect ETD, the upper cervical structures have typically experienced forces well above the threshold for their own injury. For these patients, cervical evaluation addresses the structural component that often persists after the immediate trauma effects have stabilized.
Layered presentations with autonomic features
Patients with ETD alongside other autonomic-related symptoms — chronic congestion, altered temperature regulation, gastrointestinal symptoms, or other broader autonomic features — may have systemic autonomic dysregulation contributing to multiple symptoms including the ETD. Upper cervical evaluation in these cases addresses one potential contributor to the broader autonomic picture. The evaluation should be pursued alongside appropriate medical workup for the broader autonomic symptoms.
When upper cervical evaluation is not particularly indicated
For patients with acute Eustachian tube dysfunction responding to standard treatment, patients with ETD clearly explained by allergies or specific environmental factors, patients without concurrent cervical symptoms or trauma history, and patients in the acute phase of any ear or sinus pathology requiring medical evaluation, upper cervical evaluation is not particularly indicated. Standard medical management should remain the focus for these patients.
How an Upper Cervical Evaluation Works
For appropriate patients, upper cervical chiropractic focuses specifically on the precise structural relationship between the skull, atlas, and axis — the region most closely related to the cervical autonomic anatomy discussed throughout this article.
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree. The imaging identifies the specific structural problems that may be relevant. For patients with ETD and suspected autonomic involvement, the imaging provides objective measurement rather than subjective assessment of the cervical structural picture.
Objective testing before any intervention
Leg length analysis and paraspinal infrared thermography are performed before any adjustment, and corrections are only delivered when objective findings indicate a structural shift. The principle of restraint guided by data is appropriate for ETD patients — the cervical correction is only performed when objective findings support it, not based on symptoms alone.
Precision without manipulation
Corrections are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. For patients whose autonomic systems may already be in a dysregulated state, this precision matters — aggressive cervical manipulation could potentially aggravate autonomic dysregulation and is not appropriate for this presentation.
Integration With Standard ETD Care
When upper cervical evaluation is appropriate, it should be added to standard ETD care rather than substituted for it.
Standard ETD management continues
Otolaryngology follow-up should continue. Standard ETD management — allergy management when relevant, nasal corticosteroids when indicated, treatment of any underlying sinusitis, consideration of pressure equalization techniques, evaluation for any anatomical contributors — should be optimized. The standard care addresses the immediate ETD picture; upper cervical care addresses one potential contributing factor that the standard treatments do not specifically target.
Realistic expectations
Patients pursuing upper cervical evaluation for ETD should set realistic expectations. The evaluation may identify cervical structural problems that, when corrected, may support better autonomic function over time. The response, when it occurs, is typically gradual over weeks to months rather than immediate. Lack of improvement from cervical care does not indicate the ETD diagnosis was wrong; it indicates the cervical contribution may have been limited in that particular case.
Comprehensive evaluation when appropriate
For patients with broader autonomic features beyond ETD — chronic congestion, gastrointestinal symptoms, temperature regulation issues, blood pressure variability — appropriate medical workup of the broader autonomic picture is important. Upper cervical evaluation in this broader context is one component of comprehensive care, not a substitute for medical evaluation of the autonomic features.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation may be worth considering for ETD patients when any of the following are true:
Your Eustachian tube dysfunction has not responded adequately to standard medical management despite consistent treatment. You have concurrent cervical symptoms — chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern — alongside your ETD. Your ETD developed after head or neck trauma affecting both regions. You have broader autonomic features alongside the ETD that may reflect systemic autonomic dysregulation. You have prior concussions or significant neck trauma layered on top of the current presentation. Your symptoms vary significantly with head or neck position. You have features suggesting upper cervical involvement (cervicogenic headache, cervicogenic dizziness, post-traumatic features).
For patients with acute or straightforward ETD responding to standard treatment, without concurrent cervical symptoms or trauma history, the case for upper cervical evaluation is weak. Standard medical management should remain the focus, and otolaryngology follow-up should continue as primary care.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Where to Go From Here
The autonomic regulation of mucosal tissue including the Eustachian tube mucosa is real anatomy and physiology, and the cervical sympathetic chain plays an established role in providing this autonomic innervation to the head and upper respiratory regions. The cervical sympathetic chain's proximity to upper cervical structures, combined with the broader cervical influences on central autonomic regulation through proprioceptive pathways and craniocervical hydrodynamics, creates an anatomical framework by which upper cervical structural problems could potentially affect mucosal autonomic function.
For patients with persistent Eustachian tube dysfunction not responding adequately to standard medical management, with concurrent cervical symptoms, with trauma history, or with broader autonomic features, upper cervical evaluation may be worth considering as one component of comprehensive care alongside continued standard ETD treatment. The evaluation should be pursued with realistic expectations and with continued otolaryngology follow-up as primary medical care. The evidence supporting upper cervical care for ETD is reasoning-based rather than trial-based, and patient decisions should reflect this evidence landscape.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Schilder, A. G., Bhutta, M. F., Butler, C. C., et al. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Gdowski, G. T., & McCrea, R. A. (2000). Neck proprioceptive inputs to primate vestibular nucleus neurons. Experimental Brain Research, 135(4), 511–526.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
Poe, D. S., Hanna, B. M. (2007). Balloon dilation of the cartilaginous portion of the Eustachian tube: Initial safety and feasibility analysis in a cadaver model. American Journal of Otolaryngology, 28(5), 320–322.
Goldstein, D. S., Robertson, D., Esler, M., Straus, S. E., & Eisenhofer, G. (2002). Dysautonomias: Clinical disorders of the autonomic nervous system. Annals of Internal Medicine, 137(9), 753–763.
Ward, B. K., Ashry, Y., & Poe, D. S. (2017). Patulous Eustachian tube dysfunction: Patient demographics and comorbidities. Otology & Neurotology, 38(9), 1362–1369.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with Eustachian tube dysfunction should pursue appropriate medical evaluation including otolaryngology consultation and engage with evidence-based medical management as the primary approach. Standard ETD treatments should remain the foundation of care. Upper cervical evaluation should be considered only for specific patient subsets as a complementary approach rather than a primary treatment. No claim is made or implied that upper cervical chiropractic cures or treats Eustachian tube dysfunction or any other specific disease.



Leave a comment