
"The opposite problem from blocked ears — and a structural angle worth considering when standard treatments have not provided relief"
Most people who think about Eustachian tube problems think about the familiar blocked-ear feeling — the pressure that builds during a flight, the muffled hearing that comes with a cold, the fullness that follows altitude changes. This is obstructive Eustachian tube dysfunction, where the tube fails to open properly to equalize pressure, and it is by far the more common form of the condition.
Schedule Your Appointment
Schedule appointmentPatulous Eustachian tube dysfunction is the opposite problem. The Eustachian tube fails to close properly. Instead of being closed at rest and opening briefly to equalize pressure, the tube remains abnormally open, allowing sound and air pressure to travel directly between the back of the throat and the middle ear. The symptoms this produces are distinctive, sometimes profoundly disabling, and often misdiagnosed because the picture does not match what most patients expect from an Eustachian tube problem.
This article walks through what patulous Eustachian tube dysfunction actually is, the symptoms that define it, the recognized causes, the diagnostic process, and the standard treatments — and addresses a less commonly discussed factor for the subset of patients in whom structural cervical problems may be contributing to the condition.
What Patulous Eustachian Tube Dysfunction Is
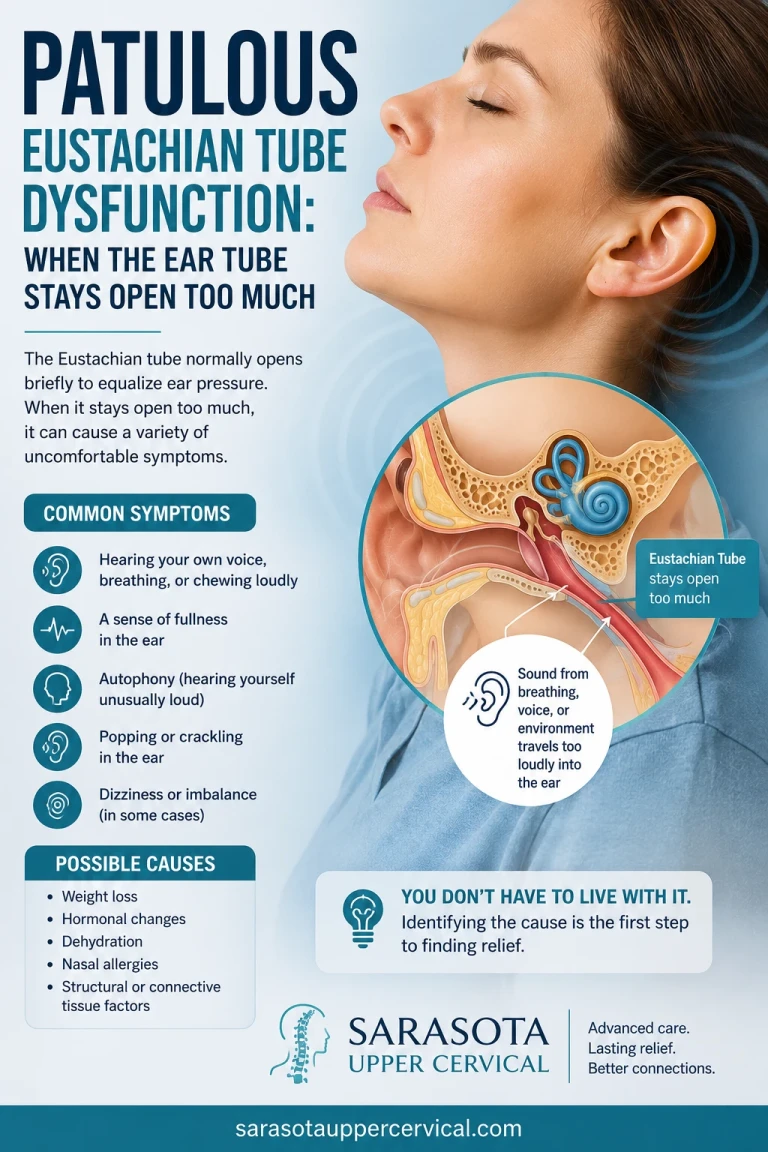
The Eustachian tube is a small canal connecting the middle ear to the back of the throat. Its primary job is to equalize air pressure between the middle ear and the outside environment, which it does by briefly opening — typically with swallowing, yawning, or jaw movement — and then closing again. The tube is closed at rest the great majority of the time, sealed by the natural elasticity of its walls and the surrounding tissues.
In patulous Eustachian tube dysfunction, the tube fails to maintain this normal closed state. It remains either chronically open or excessively easy to open with minimal stimulus. The result is that the middle ear becomes acoustically and mechanically connected to the back of the throat in a way that should not normally occur. Sounds, air pressure changes, and even the patient's own voice and breathing travel directly from the throat into the middle ear, producing the characteristic symptoms.
The condition is less common than obstructive Eustachian tube dysfunction by a substantial margin. It is also frequently under-recognized because the symptoms are unusual and patients may struggle to describe them clearly. Many patients receive multiple diagnoses or extended workups before patulous Eustachian tube dysfunction is identified.
The Symptoms That Define Patulous ETD
The symptom pattern of patulous Eustachian tube dysfunction is distinctive once recognized. The core symptoms reflect the abnormal acoustic and mechanical connection between the throat and the middle ear.
Autophony — hearing your own voice in the ear
The signature symptom. Patients hear their own voice resonating, echoing, or reverberating in the affected ear when they speak. The sensation is often described as similar to having a microphone inside the ear, or like talking inside a barrel. Autophony can be profoundly disturbing — patients sometimes find it difficult to converse, to speak on the phone, or to engage in any sustained vocal activity because of how their own voice sounds to them. Singers, teachers, and others who rely on voice professionally may find the condition career-limiting.
Hearing your own breathing
Patients hear their own breathing — the inhale, the exhale, sometimes the heartbeat — in the affected ear. The sounds are louder than would be expected and reflect the open airway between the throat and middle ear amplifying these normal internal sounds. Many patients describe this as one of the most distressing aspects of the condition because it is continuous and difficult to ignore.
Fluctuating fullness sensation
A sensation of fullness or pressure in the affected ear, often paradoxically similar to obstructive Eustachian tube dysfunction even though the underlying problem is opposite. The fullness may fluctuate, often improving when lying down (which engorges the surrounding tissues and partially closes the tube) and worsening when upright or after exercise.
Symptoms improving with head-down position
Related article
Seeing the Whole Picture: CBCT, the Blair Analysis, and Why Precision Changes Outcomes
Jun 20, 2026
A distinctive feature: many patients with patulous Eustachian tube dysfunction notice that their symptoms improve when they lie down, bend forward, or position the head below the level of the heart. This positional improvement reflects the increased blood flow and tissue engorgement around the tube in dependent positions, which helps close the abnormally open tube. Recognizing this pattern can help confirm the diagnosis.
Symptoms worsening with exercise, dehydration, or stress
Patulous Eustachian tube dysfunction often worsens during activities that reduce tissue fluid content — exercise, sustained physical activity, dehydration, dry environments. Stress may also worsen symptoms, possibly through autonomic effects on tissue tone and blood flow.
Tinnitus
Some patients experience tinnitus in the affected ear, though the patulous ETD itself is more associated with the autophony and breathing sounds than with classic tinnitus.
Hearing changes
Most patients with patulous Eustachian tube dysfunction have normal hearing thresholds on standard audiometry. The condition typically does not produce permanent hearing damage. However, the subjective experience of altered hearing — the sense that their own voice is too loud, that ambient sounds are distorted — is real and reflects the abnormal acoustic environment of the middle ear rather than structural hearing damage.
What Causes Patulous Eustachian Tube Dysfunction
The underlying causes of patulous Eustachian tube dysfunction vary, and most patients have one or more identifiable contributing factors.
Weight loss
The single most commonly identified cause. The Eustachian tube is supported by surrounding fat tissue, and rapid or substantial weight loss removes this support, allowing the tube to remain abnormally open. Patients who develop patulous Eustachian tube dysfunction after significant weight loss — through dieting, bariatric surgery, illness, or other causes — represent the largest single category of cases. The connection is so well established that weight loss is one of the first factors clinicians inquire about when evaluating possible patulous Eustachian tube dysfunction.
Pregnancy
Hormonal and fluid balance changes during pregnancy can produce patulous Eustachian tube dysfunction that resolves after delivery. Some women experience the condition only during specific pregnancies, and the postpartum resolution is usually complete.
Hormonal changes
Estrogen-related changes — including those associated with hormonal contraceptive use, menstrual cycles, and perimenopause — can affect tissue volume and tone around the Eustachian tube. The hormonal contribution is more variable than weight loss but is recognized in clinical practice.
Dehydration
Reduced tissue fluid content can contribute to or worsen patulous Eustachian tube dysfunction. Severe or chronic dehydration is associated with symptom development, and rehydration sometimes produces meaningful symptom improvement.
Stress
Chronic stress is associated with patulous Eustachian tube dysfunction, possibly through effects on autonomic regulation of tissue tone and vascular function. Many patients describe stress as a meaningful trigger or aggravator of their symptoms.
Neurological causes
Conditions affecting the tensor veli palatini and levator veli palatini muscles — the muscles that control Eustachian tube opening and closing — can produce patulous Eustachian tube dysfunction. These conditions include stroke affecting relevant brainstem regions, multiple sclerosis, and various other neurological disorders affecting cranial nerve V or the pharyngeal plexus.
Post-traumatic onset
Patulous Eustachian tube dysfunction can develop after head or neck trauma, including whiplash, concussion, and significant falls. For these patients, the trauma that triggered the Eustachian tube dysfunction may have also produced upper cervical structural injury, and the broader picture often includes more than the ear symptoms alone.
Idiopathic cases
A substantial percentage of patulous Eustachian tube dysfunction cases occur without any identifiable cause. These patients are diagnosed as idiopathic, and the underlying mechanism remains unclear.
How Patulous ETD Is Diagnosed
Patulous Eustachian tube dysfunction is a clinical diagnosis established by the symptom pattern, physical examination findings, and exclusion of other causes.
Symptom history
Recognition of the distinctive symptom pattern — autophony, hearing one's own breathing, fullness sensation that improves with head-down positioning, worsening with exercise and dehydration — is the foundation of diagnosis. Many patients are diagnosed primarily on history alone, with examination confirming what the symptoms suggest.
Otoscopic examination
Examination of the tympanic membrane sometimes reveals characteristic findings — the membrane may move in and out with the patient's breathing, which is highly suggestive of patulous Eustachian tube dysfunction. This finding is not present in all cases but is essentially diagnostic when seen.
Tympanometry
Tympanometry measures the movement of the tympanic membrane in response to pressure changes. In patulous Eustachian tube dysfunction, tympanometry may show characteristic respiratory variations reflecting the patient's breathing transmitted through the abnormally open tube. This finding helps distinguish patulous from obstructive Eustachian tube dysfunction.
Audiometry
Standard audiometry is typically normal in patulous Eustachian tube dysfunction but is performed to document hearing status and rule out other conditions affecting hearing.
Imaging
CT or MRI imaging is sometimes obtained to evaluate for structural abnormalities, particularly when the clinical picture is atypical or when other diagnoses need to be excluded. Specialized imaging of the Eustachian tube itself is occasionally used in academic centers.
Standard Treatment Approaches
Treatment of patulous Eustachian tube dysfunction follows a stepwise approach, with intensity matched to symptom severity and treatment response.
First-line: hydration and weight restoration
For patients whose patulous Eustachian tube dysfunction is associated with dehydration or recent weight loss, restoration of normal hydration and weight stabilization or gain (when appropriate) often produces meaningful improvement. These interventions address the underlying contributing factors directly.
Saline nasal sprays and irrigation
Saline applied to the nasal passages can produce temporary tissue swelling around the Eustachian tube opening, providing symptom relief. Some patients use these regularly for symptom management.
Estrogen creams or other topical agents
Various topical agents applied to the nasal cavity have been used to produce tissue swelling around the Eustachian tube opening. These are used in selected cases and require professional guidance.
Behavioral modifications
Avoidance of behaviors that worsen symptoms — vigorous nose-blowing, certain breathing patterns, prolonged speaking — can provide partial relief. Some patients learn to manage their symptoms through these adaptations.
Surgical approaches
For severe cases not responsive to conservative management, surgical options include Eustachian tube injection with bulking agents, surgical narrowing of the tube, and tympanostomy tube placement. Surgical management is typically reserved for severe, disabling cases that have not responded to other approaches.
Where the Craniocervical Junction Fits Into the Picture
The connection between upper cervical structural problems and patulous Eustachian tube dysfunction is less direct than for some other ear-related conditions, but specific anatomical and physiological relationships make consideration of the cervical component appropriate for certain patient subsets. Patients deserve an honest account of where this evidence stands.
The anatomical proximity and shared neural control
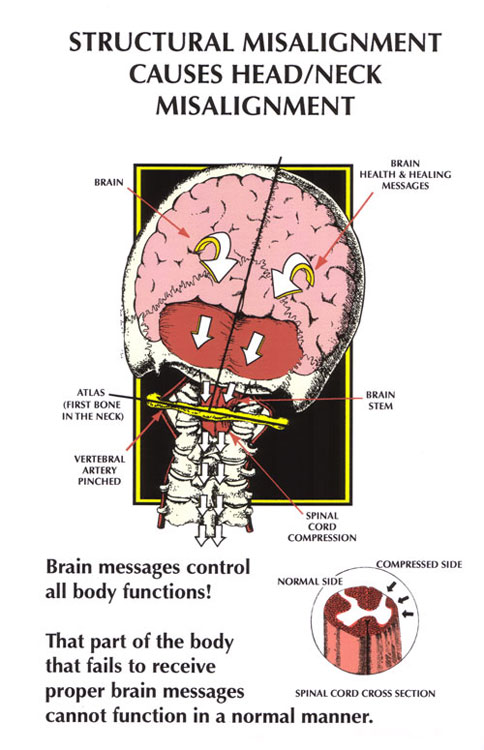
The Eustachian tube is opened and closed by the action of two muscles — primarily the tensor veli palatini, with contribution from the levator veli palatini. The tensor veli palatini is innervated by the mandibular branch of the trigeminal nerve (cranial nerve V), and the levator veli palatini is innervated by the pharyngeal plexus, which receives contributions from cranial nerve X (vagus) and the cervical sympathetic chain. These cranial nerves emerge from the brainstem, which sits within the bony corridor formed by the skull, atlas (C1), and axis (C2). The cervical sympathetic chain runs along the front of the upper cervical spine. The autonomic and motor control of the Eustachian tube musculature thus passes through or near the craniocervical region.
Related article
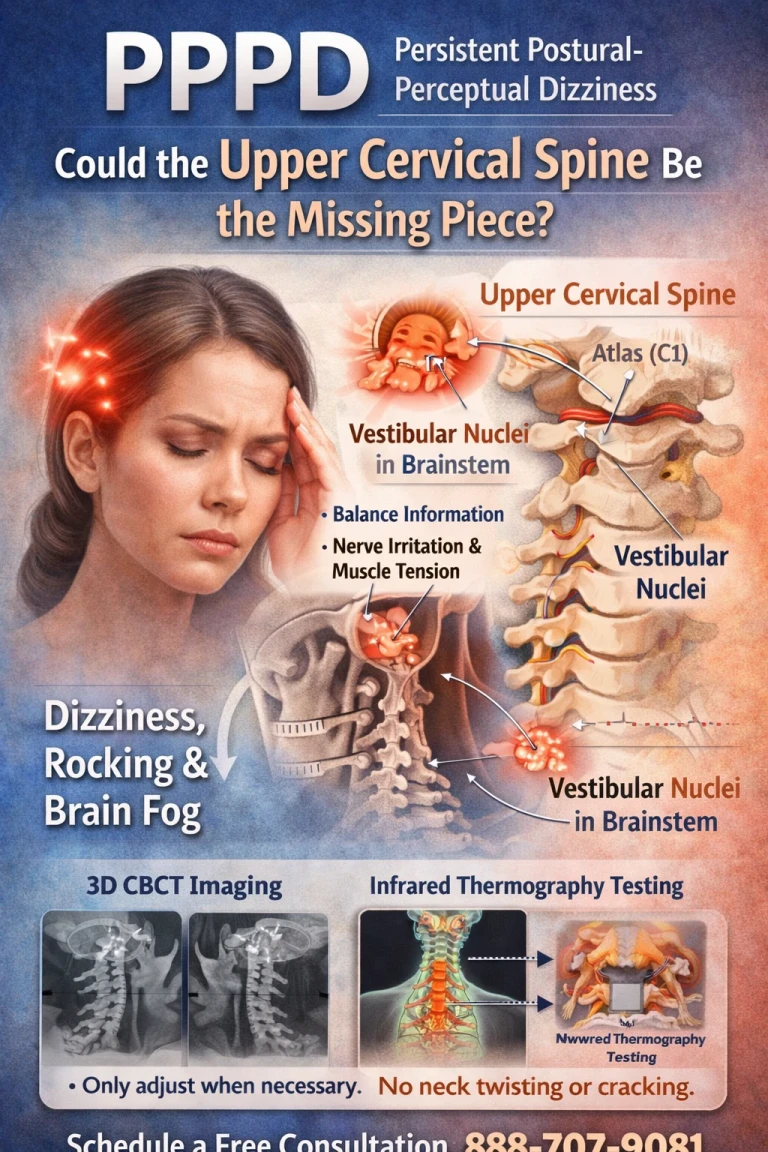
PPPD Treatment in Sarasota: Could the Upper Cervical Spine Be the Missing Piece?
Mar 25, 2026When the upper cervical structure is significantly misaligned — particularly after trauma — the mechanical environment of the brainstem and the surrounding cranial nerves can be affected. Chronic low-grade mechanical irritation, altered autonomic balance, and effects on the cervical sympathetic chain can plausibly influence the neural control of the Eustachian tube musculature, contributing to abnormal tube tone.
The autonomic angle
Patulous Eustachian tube dysfunction often worsens with stress and improves with rest, lying down, and other parasympathetic-dominant states. This pattern suggests autonomic regulation is contributing to symptom severity. The vagus nerve is the primary parasympathetic input to the head and neck region, and it emerges from the brainstem and passes through the craniocervical region. Chronic craniocervical structural irritation can affect autonomic balance, contributing to the autonomic state in which patulous symptoms are more pronounced.
The post-traumatic subset
Patients whose patulous Eustachian tube dysfunction began after head or neck trauma represent the subset for whom the cervical connection is most plausible. The trauma that triggered the ear symptoms also produced upper cervical structural injury, and the broader picture in these patients typically includes neck pain, suboccipital tension, possible cervicogenic headache, and sometimes vestibular or visual symptoms — all suggesting the cervical involvement extends beyond just the ear symptoms.
Honest framing of the evidence
Direct research connecting upper cervical chiropractic to patulous Eustachian tube dysfunction outcomes is limited. The framework rests on anatomical relationships and clinical observation rather than on randomized controlled trial evidence. Patients considering upper cervical evaluation for patulous Eustachian tube dysfunction should understand that this represents a hypothesis-driven consideration for specific patient subsets, not an established treatment supported by formal clinical research. For most patients, addressing weight, hydration, and other identified contributing factors should be the primary approach, with structural evaluation considered for the subset of patients with trauma history or associated cervical symptoms.
How Upper Cervical Care Addresses the Structural Component
Upper cervical chiropractic is a specialty within the broader chiropractic profession that focuses specifically on the precise structural relationship between the skull, atlas, and axis. For patients with patulous Eustachian tube dysfunction in whom a structural cervical contribution is suspected, the evaluation can identify whether meaningful misalignment is present.
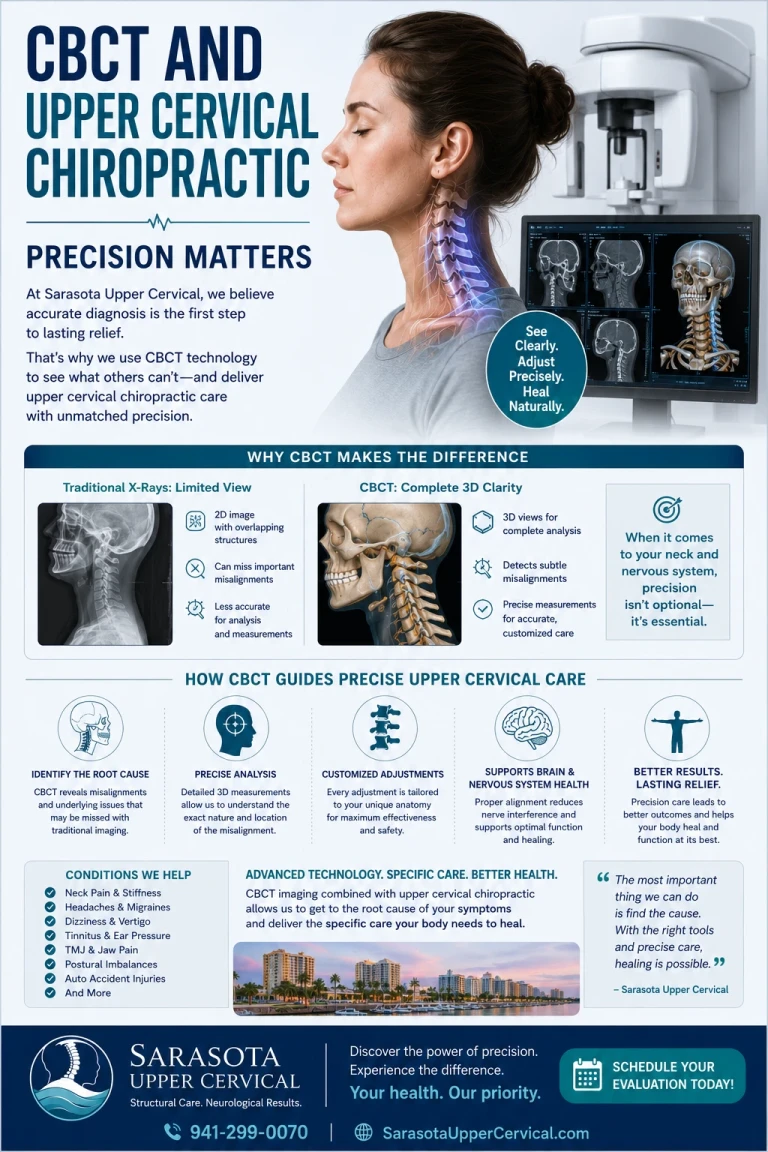
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree — precision that standard X-rays cannot match. The imaging allows the practitioner to determine whether a meaningful structural component is present and exactly what its direction and magnitude are.
Objective testing before any intervention
Two objective tests are performed at every visit. Leg length analysis measures functional postural asymmetry that reflects upper cervical misalignment. Paraspinal infrared thermography measures asymmetric autonomic activity along the cervical spine. If both tests indicate the spine is in alignment, no adjustment is delivered. If they indicate a shift, a precise correction is delivered along the vector calculated from the CBCT analysis.
Precision without manipulation
When corrections are indicated, they are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. For patients with ear symptoms — whose inner ear and Eustachian tube systems are already sensitized — this precision matters.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation is worth considering for patulous Eustachian tube dysfunction patients when any of the following are true:
Your symptoms began after head or neck trauma — whiplash, concussion, sports head injury, significant fall — and have persisted since. You have associated cervical symptoms — chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern — alongside the ear symptoms. Your symptoms include features beyond patulous Eustachian tube dysfunction alone — vestibular symptoms, brain fog, autonomic dysregulation — suggesting broader involvement. Standard treatments for patulous Eustachian tube dysfunction (hydration, weight management, saline, behavioral modifications) have not adequately controlled your symptoms. You have a history of chronic stress or autonomic dysregulation alongside the ear symptoms. You are pursuing comprehensive evaluation and want to ensure the structural angle has been addressed.
For patulous Eustachian tube dysfunction patients without these features — particularly those with clear weight loss, pregnancy, or hormonal triggers — the case for upper cervical evaluation is weaker, and standard approaches addressing the identified causes should be the focus.
To schedule an upper cervical evaluation at Sarasota Upper Cervical Chiropractic, call 941-259-1891.
Where to Go From Here
Patulous Eustachian tube dysfunction is a recognized, identifiable condition with distinctive symptoms and several identifiable contributing factors. For most patients, standard care addressing identified contributors — weight restoration, hydration, behavioral modification, topical agents, and in severe cases surgical intervention — should be the primary approach. For the subset of patients whose patulous Eustachian tube dysfunction began after trauma, who have associated cervical symptoms, or whose symptoms have not responded to standard treatment, the upper cervical spine deserves consideration as part of a more complete evaluation.
Sarasota Upper Cervical Chiropractic uses three-dimensional CBCT imaging and precision-based correction to address structural problems in the upper cervical region when present. To schedule an evaluation, call 941-259-1891.
References
Poe, D. S. (2007). Diagnosis and management of the patulous eustachian tube. Otology & Neurotology, 28(5), 668–677.
Ward, B. K., Ashry, Y., & Poe, D. S. (2017). Patulous eustachian tube dysfunction: Patient demographics and comorbidities. Otology & Neurotology, 38(9), 1362–1369.
Schilder, A. G. M., Bhutta, M. F., Butler, C. C., et al. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Hori, Y., Kawase, T., Hasegawa, J., et al. (2006). Audiometry with nasally presented masking noise: Novel diagnostic method for patulous eustachian tube. Otology & Neurotology, 27(5), 596–599.
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Tracey, K. J. (2002). The inflammatory reflex. Nature, 420(6917), 853–859.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with suspected patulous Eustachian tube dysfunction should pursue appropriate medical evaluation by an otolaryngologist, particularly given the importance of addressing identifiable contributing factors such as weight loss and dehydration. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment