

"The atlas vertebra (C1) is one of the most proprioceptively important structures in your body. When it is misaligned, the consequences extend far beyond local neck symptoms — they reach into balance, spatial orientation, and the way your brain processes head position. Understanding the C1-proprioception relationship clarifies why upper cervical correction can address symptoms that seem unrelated to the neck"
Most people understand that the neck contains muscles, joints, and structures that can produce neck pain. Far fewer people understand that the upper cervical region — particularly the area around the first cervical vertebra, the atlas (C1) — is one of the most neurologically dense and proprioceptively important regions in the entire body. The atlas is not just a structural support for the head; it is the location where some of the most concentrated proprioceptive input in the body originates. When the atlas is misaligned, the consequences are not limited to neck symptoms. They extend into balance, spatial orientation, dizziness, and the broader way the brain processes head position relative to the rest of the body.
Schedule Your Appointment
Schedule appointmentUnderstanding why C1 has this disproportionate importance requires understanding what proprioception is, why the upper cervical region is exceptional, and how the atlas specifically connects to the brain's balance processing centers. The neuroscience supporting this connection is well-established mainstream research, with key papers documenting the receptor density in the suboccipital muscles, the mechanoreceptor populations in the upper cervical joints, and the direct neural pathways from these structures to the vestibular nuclei in the brainstem. When this proprioceptive system functions normally, balance and spatial orientation operate seamlessly. When the atlas is misaligned, the system sends distorted information to the brain, with consequences that can manifest as dizziness, unsteadiness, motion sensitivity, and the broader symptom patterns of cervicogenic dizziness and contributing factors in other vestibular conditions.
This article walks through what proprioception is and why it matters, why the upper cervical region around C1 is exceptionally important for proprioception, the specific anatomical structures that make C1 a proprioceptive hub, how the atlas connects to the brain's balance processing, what happens when C1 is misaligned, the clinical features that emerge from C1-related proprioceptive distortion, and how upper cervical correction specifically addresses these issues for appropriate patients in Sarasota and surrounding communities.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
What Proprioception Is and Why It Matters
Before exploring why the atlas is proprioceptively unique, it helps to understand what proprioception is generally. Proprioception is one of the most important senses in the body, yet it operates almost entirely below conscious awareness — which is why most people are unaware of how essential it is until something goes wrong.
The sense you don't notice
Close your eyes and lift your hand. You know where your hand is in space — its position relative to your body, the angle of your wrist and elbow, whether your fingers are extended or curled. You did not need to see your hand to know these things. This awareness is proprioception — the sense of body position and movement that operates continuously, providing the brain with constant information about where every part of the body is. Without proprioception, even simple movements would require constant visual monitoring. With normal proprioception, the body operates as a coordinated whole with the brain knowing where everything is at all times.
How proprioception works
Proprioception is mediated by specialized sensory receptors throughout the body. Muscle spindles detect muscle length and rate of length change. Golgi tendon organs detect muscle tension. Joint mechanoreceptors detect joint position and movement. Cutaneous receptors contribute information about skin stretch and pressure. These receptors send continuous signals to the central nervous system, where the information is integrated to produce the brain's representation of body position. The integration happens through specific neural pathways with extensive connections to balance, motor control, and spatial orientation centers.
Why proprioception is essential for balance
Balance is not produced by any single sensory system but by integration of three main inputs: vestibular input from the inner ear (detecting head motion), visual input from the eyes (detecting the visual environment), and proprioceptive input from throughout the body (detecting body position). When all three inputs are accurate and consistent, balance processing produces accurate awareness of position and motion. When one input is distorted, the integration produces less accurate results. The brain may perceive motion that is not occurring, may feel unsteady when actually stable, or may experience sensory conflict that produces dizziness.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Why the cervical region matters specifically
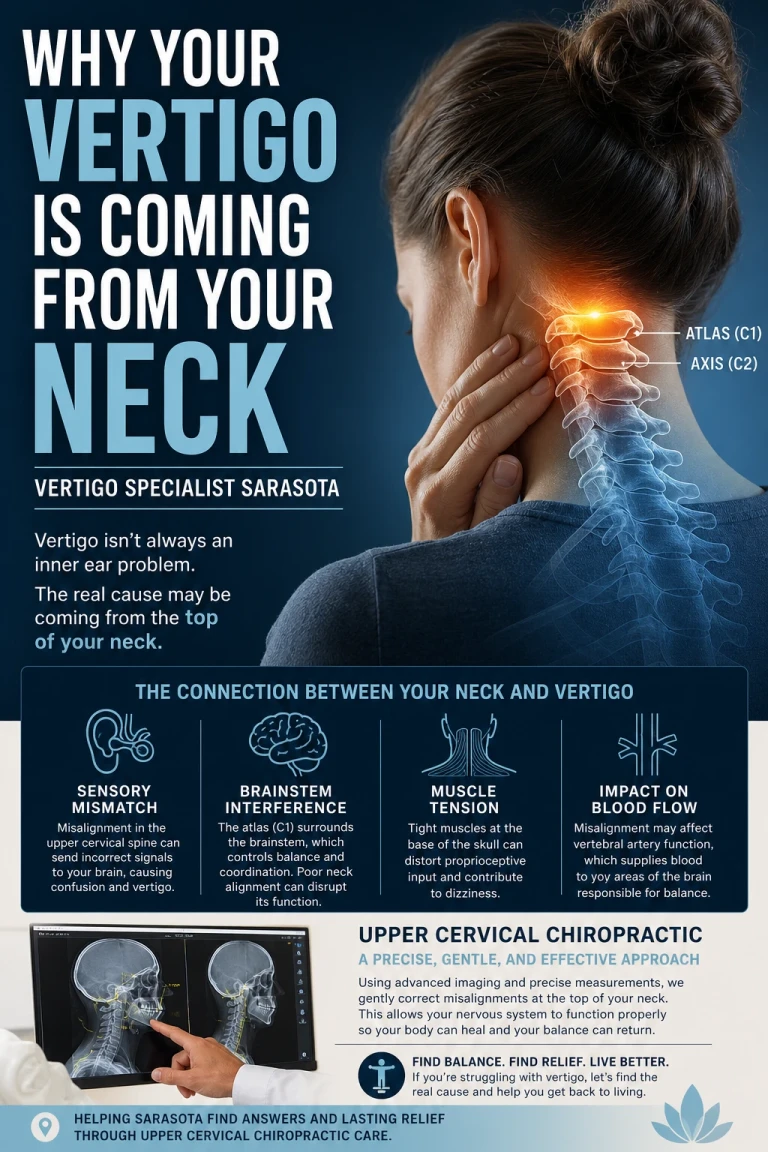
Among proprioceptive sources throughout the body, the cervical region is exceptionally important for balance. This special status reflects several factors: the head's mobility relative to the body, the proximity of the cervical receptors to the balance processing centers, the dense receptor populations in the upper cervical structures, and the direct neural pathways from cervical receptors to the brainstem balance centers. The cervical contribution to balance is so substantial that distortion of cervical proprioception can produce dizziness comparable to that produced by inner ear conditions — even when the inner ear itself is functioning normally.
Why C1 Is Exceptionally Important for Proprioception
Within the cervical region, the upper cervical area around C1 (the atlas) has disproportionate importance for proprioception. Understanding why requires looking at the specific anatomy of this region and what makes it different from the rest of the spine.
The unique anatomy of the atlas
The first cervical vertebra — the atlas, named after the mythological figure who supported the world on his shoulders — is unlike any other vertebra in the spine. It has no vertebral body. It is essentially a ring of bone designed to articulate with the skull above and the axis (C2) below. The arrangement allows for extensive head movement — head rotation primarily occurs at the C1-C2 level, while head flexion-extension primarily occurs at the C0-C1 (skull-atlas) level. The atlas does not bear weight in the same way as other vertebrae; instead, it functions as a precise articulating structure that allows the head to move freely on the cervical spine.
The atlanto-occipital and atlanto-axial joints
Two specialized joint complexes involve the atlas: the atlanto-occipital joint (between the skull and C1) and the atlanto-axial joint (between C1 and C2). These joints are different from typical spinal joints in several important ways. They allow much greater range of motion than typical facet joints. They have specialized capsular structures with extensive ligamentous support including the alar ligaments, transverse ligament, and other specialized structures. And critically for proprioception, they have exceptionally dense mechanoreceptor populations. The 1994 paper by McLain in Spine documented dense mechanoreceptor innervation in cervical facet joints, with the upper cervical joints showing particularly rich receptor populations (McLain, 1994). The receptors in these joints provide the brain with detailed information about the position and motion of the head relative to the upper neck.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Related article
Brain Fog Might Be Coming From an Upper Neck Misalignment | Brain Fog Relief Sarasota
Mar 22, 2026The suboccipital muscles and their proprioceptive richness
Surrounding the atlas are four small muscles that form the suboccipital group: the rectus capitis posterior major, the rectus capitis posterior minor, the obliquus capitis superior, and the obliquus capitis inferior. These muscles are small — much smaller than the larger muscles of the neck — but they have an extraordinary proprioceptive density. The 2001 study by Kulkarni and colleagues in Neurology India quantified the muscle spindle density in these suboccipital muscles and found substantially higher density than in most other muscles in the body (Kulkarni et al., 2001). The receptors in these muscles provide the brain with extraordinarily detailed information about head position and motion.
What this density means functionally
The combination of dense joint mechanoreceptors and exceptionally rich muscle spindle populations means the upper cervical region around C1 generates a disproportionate amount of the proprioceptive information the brain uses for head position awareness. While proprioceptive input comes from receptors throughout the body, the upper cervical input is particularly important for the specific function of knowing where the head is relative to the body. This information is essential for balance, for coordinated head and eye movements, and for the brain's broader spatial orientation processing.
Why evolution made it this way
The exceptional proprioceptive density at the upper cervical region reflects the functional importance of accurate head position awareness. The head contains the primary sensory organs — eyes, ears, vestibular apparatus — and the brain needs to know precisely where the head is positioned and how it is moving to make sense of the information from these sensory organs. The brain's interpretation of visual motion depends on knowing whether the head is moving or whether the visual field is moving. The brain's processing of vestibular signals from the inner ear depends on knowing the head's position relative to gravity. The dense proprioceptive input from the upper cervical region provides this essential reference information.
How C1 Connects to the Brain's Balance Processing
Beyond the receptor density at C1, the neural pathways from these receptors connect directly to the brain's balance processing centers in ways that make the C1-balance relationship particularly direct.
The proximity to the brainstem
The atlas sits immediately below the skull, and the spinal cord transitions through the foramen magnum into the brainstem just above this level. The proximity means the proprioceptive signals from C1 and surrounding structures reach the brainstem with minimal travel distance. Unlike proprioceptive input from the feet or other distant body regions that travels through the spinal cord before reaching the brainstem, upper cervical proprioceptive input is essentially adjacent to its target processing centers.
The vestibular nuclei
The brainstem contains the vestibular nuclei — four major nuclei (superior, lateral, medial, and inferior vestibular nuclei) located in the upper medulla and lower pons. These nuclei serve as the central integration hub for balance processing. They receive input from the inner ear vestibular apparatus, from visual systems, and importantly from proprioceptive sources particularly the cervical region. The 2000 study by Gdowski and McCrea in Experimental Brain Research documented direct cervical proprioceptive input to vestibular nucleus neurons (Gdowski & McCrea, 2000). This direct connection means upper cervical input is integrated with vestibular input at the brainstem level, contributing to balance processing.
Why this integration matters
The integration of cervical proprioceptive input with vestibular input is essential for accurate balance processing. The vestibular apparatus tells the brain about head motion. The cervical proprioceptive input tells the brain about head position relative to the body. Without integrating both pieces of information, the brain cannot distinguish between the head turning while the body remains still versus the body turning while the head remains still — these produce different vestibular signals but both produce head motion. The cervical input clarifies which scenario is occurring, allowing accurate interpretation.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The output to multiple systems
After integration, the brainstem processing produces output to multiple systems. The vestibulo-ocular reflex stabilizes vision during head movement by producing compensatory eye movements. The vestibulospinal pathways adjust postural muscles to maintain upright posture. The autonomic regulatory regions adjust cardiovascular and other autonomic functions appropriately. The cortical projections produce conscious awareness of position and orientation. All of these outputs depend on accurate integration that itself depends on accurate input — including accurate proprioceptive input from the upper cervical region around C1.
The cortical balance network
Beyond the brainstem processing, balance information is processed in extensive cortical regions including the insular cortex, parieto-insular vestibular cortex, parts of the temporal lobe, and connections with attention and emotion regions. The cortical processing creates conscious balance experience and supports adaptive behavioral responses. Distorted input from C1-related proprioceptive problems affects this cortical processing too, contributing to the conscious experience of dizziness or unsteadiness that patients report.
What Happens When C1 Is Misaligned
When the atlas is structurally misaligned, the proprioceptive system that depends on accurate C1 position malfunctions in specific ways. Understanding what happens clarifies why C1 misalignment can produce symptoms that seem unrelated to the neck itself.
The mechanical reality of misalignment
C1 misalignment can occur from various causes — direct trauma (concussion, whiplash, sports impacts, falls), repetitive postural problems (forward head posture from prolonged computer or device use), accumulated minor trauma over years, or other factors. The misalignment may be subtle in terms of millimeters or fractions of a degree but produces disproportionate functional consequences because of the precision required at this joint. The atlas does not have a vertebral body to provide built-in alignment stability — it depends on ligamentous and muscular structures to maintain its position. When these structures are disrupted or chronically tensed, alignment can become abnormal.
Distorted proprioceptive signaling
When C1 is misaligned, the proprioceptive receptors around it send signals reflecting the abnormal position. The joint mechanoreceptors in the atlanto-occipital and atlanto-axial joints report joint positions that differ from the normal pattern. The muscle spindles in the suboccipital muscles report muscle lengths that reflect the compensatory tension required to maintain head position despite the structural problem. The signals are not random — they accurately reflect the current state of the structures. But the current state is abnormal, and the resulting signals create a distorted picture of head position.
Compensatory muscle tension
The suboccipital muscles surrounding C1 must work continuously to maintain functional head position despite structural misalignment. This compensatory tension is not a brief response — it is chronic, lasting as long as the structural problem persists. The muscles remain partially contracted, which has multiple consequences. The chronically contracted state produces metabolic stress in the muscles. The proprioceptive signaling from the muscles becomes increasingly distorted as the muscles operate outside their normal length-tension range. Trigger points develop in the chronically tense tissue. And the broader pattern of compensation often extends to other cervical and shoulder muscles.
Sensory conflict at the brainstem
The distorted proprioceptive input from misaligned C1 reaches the vestibular nuclei where it is integrated with vestibular and visual input. The integration process expects consistent inputs from all three sources. When the proprioceptive input doesn't match the vestibular and visual input, the integration produces conflicting results. The brain may calculate that the head is in one position based on proprioception but in a different position based on vestibular input. This sensory conflict can be interpreted by the brain as motion that is not occurring, as instability, or as a sensory environment that does not match reality.
Joint position error
One of the most measurable consequences of C1-related proprioceptive distortion is joint position error — the inability to accurately sense and reproduce head positions. The 2003 study by Treleaven and colleagues in the Journal of Rehabilitation Medicine documented measurable cervical joint position error in whiplash patients with dizziness (Treleaven et al., 2003). When asked to return their heads to a remembered neutral position after movement, these patients showed systematic errors. They could not accurately sense where their head was, reflecting the distorted proprioceptive processing. Joint position error is now used clinically as a marker of cervicogenic dizziness and as a target for rehabilitation.
Why this produces persistent symptoms
The combination of distorted proprioceptive input, sensory conflict at the brainstem, and joint position error creates persistent rather than episodic symptoms. The patient is not having occasional brief episodes — they are receiving continuously distorted balance information, with the brain attempting to make sense of inputs that don't match. The persistent nature of the underlying cause produces the persistent unsteadiness, dizziness, motion sensitivity, and broader symptoms characteristic of cervicogenic conditions.
Clinical Features That Emerge from C1 Misalignment
When C1 misalignment produces proprioceptive distortion, the resulting clinical features can be specific and recognizable. Understanding these features helps patients identify whether their symptoms may relate to upper cervical involvement.
Persistent unsteadiness rather than spinning
Patients with C1-related proprioceptive distortion typically describe persistent unsteadiness, disequilibrium, or a sense that something is off with their balance — rather than the discrete spinning vertigo episodes characteristic of BPPV or vestibular migraine. The unsteadiness is often described as a constant background sensation that may be subtle but is continuously present. Some patients describe feeling like they are walking on a boat, having a sense of being slightly off-center, or experiencing brief moments of imbalance throughout the day.
Symptoms that vary with head and neck position
Because the symptoms originate from cervical proprioceptive distortion, they typically vary with head and neck position. Sustained postures often worsen symptoms — long periods at a computer, prolonged driving, or other situations where the head is held in one position for extended time. Specific head positions may reliably trigger or worsen symptoms. Movement of the head and neck often affects symptoms in ways that pure inner ear conditions would not.
Associated cervical symptoms
Patients with C1-related proprioceptive symptoms typically have associated cervical symptoms — chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern, or tenderness at the base of the skull. These associated symptoms reflect the underlying structural problem and the compensatory muscle tension. The cervical features alongside the balance symptoms support the cervicogenic interpretation rather than purely inner ear-based conditions.
Motion sensitivity
Many patients with C1-related proprioceptive distortion have motion sensitivity — discomfort with motion in their visual environment, difficulty in busy visual settings like grocery stores or crowded venues, discomfort with motion in films or screen content. The motion sensitivity reflects the broader integration disturbance at the brainstem, with the sensory system having difficulty processing complex motion when proprioceptive input is unreliable.
Difficulty with head movements
Specific head movements often trigger or worsen symptoms — turning the head to check blind spots while driving, looking up at high shelves, sustained looking down at work or reading. These movements activate the proprioceptive system in ways that produce noticeable symptoms when the system is distorted, whereas they would be unremarkable in patients with normal cervical proprioception.
Trauma history is often present
Many patients with C1 misalignment-related proprioceptive symptoms have a history of head or neck trauma — concussion, whiplash, sports injuries, falls — that may have initiated or contributed to the structural problem. The 2005 study by Kaale and colleagues in the Journal of Neurotrauma documented that whiplash mechanisms produce upper cervical ligamentous injuries at forces below those required for diagnosable concussion (Kaale et al., 2005). The dual injury reality means trauma sufficient to produce vestibular symptoms essentially always produced upper cervical structural injury as well.
The cervicogenic dizziness pattern
When these features cluster together — persistent unsteadiness rather than spinning, symptom variation with head position, associated cervical features, motion sensitivity, difficulty with head movements, and often trauma history — they form the clinical picture of cervicogenic dizziness. The 2017 paper by Reiley and colleagues in Archives of Physiotherapy outlined the diagnostic framework for this condition (Reiley et al., 2017), with the 2022 paper by Peng and colleagues in the Journal of Clinical Medicine providing the comprehensive review (Peng et al., 2022). C1 misalignment is one of the most common structural causes producing this clinical picture.
C1 Proprioceptive Contribution to Other Vestibular Conditions
Beyond cervicogenic dizziness, C1-related proprioceptive distortion can contribute to other vestibular conditions in appropriate patients. Understanding these contributions clarifies why C1 evaluation can be relevant across a range of vestibular presentations.
Post-concussion vestibular dysfunction
Post-concussion patients essentially always have C1 involvement because the trauma that produced the concussion also affected the upper cervical structures. The proprioceptive distortion from C1 misalignment adds to the broader post-concussion picture, contributing to the persistent dizziness and balance problems many post-concussion patients experience. Addressing the C1 component during recovery can support the central compensation that vestibular rehabilitation is targeting.
PPPD (Persistent Postural-Perceptual Dizziness)
PPPD involves a maladaptive central pattern that fails to resolve after an acute precipitating event. For PPPD that developed after head or neck trauma, the concurrent C1 misalignment can contribute to maintaining the maladaptive pattern by providing ongoing distorted proprioceptive input. The brain attempting to recover from the original event receives unreliable input from the misaligned C1, potentially preventing normal recalibration.
Vestibular migraine
Vestibular migraine involves the trigeminocervical complex where trigeminal and upper cervical input converge in the brainstem. C1 misalignment affecting the cervical input to this complex can contribute to migraine system activation in susceptible patients. The contribution is particularly relevant for post-traumatic vestibular migraine and for cases with prominent cervical features.
Recovery from labyrinthitis or vestibular neuritis
Recovery from acute vestibular events depends on central compensation, which requires accurate proprioceptive input. C1 misalignment producing distorted proprioception can complicate recovery by feeding unreliable information into the compensation process. For patients with stalled recovery from acute vestibular events, particularly when trauma was part of the precipitating event, C1 evaluation can be relevant.
How C1 Correction Addresses the Proprioceptive Distortion
For patients with C1-related proprioceptive distortion contributing to their symptoms, structural correction of the atlas can address the root cause of the distorted input. Understanding how the correction works clarifies what to expect from upper cervical evaluation and care.
Related article
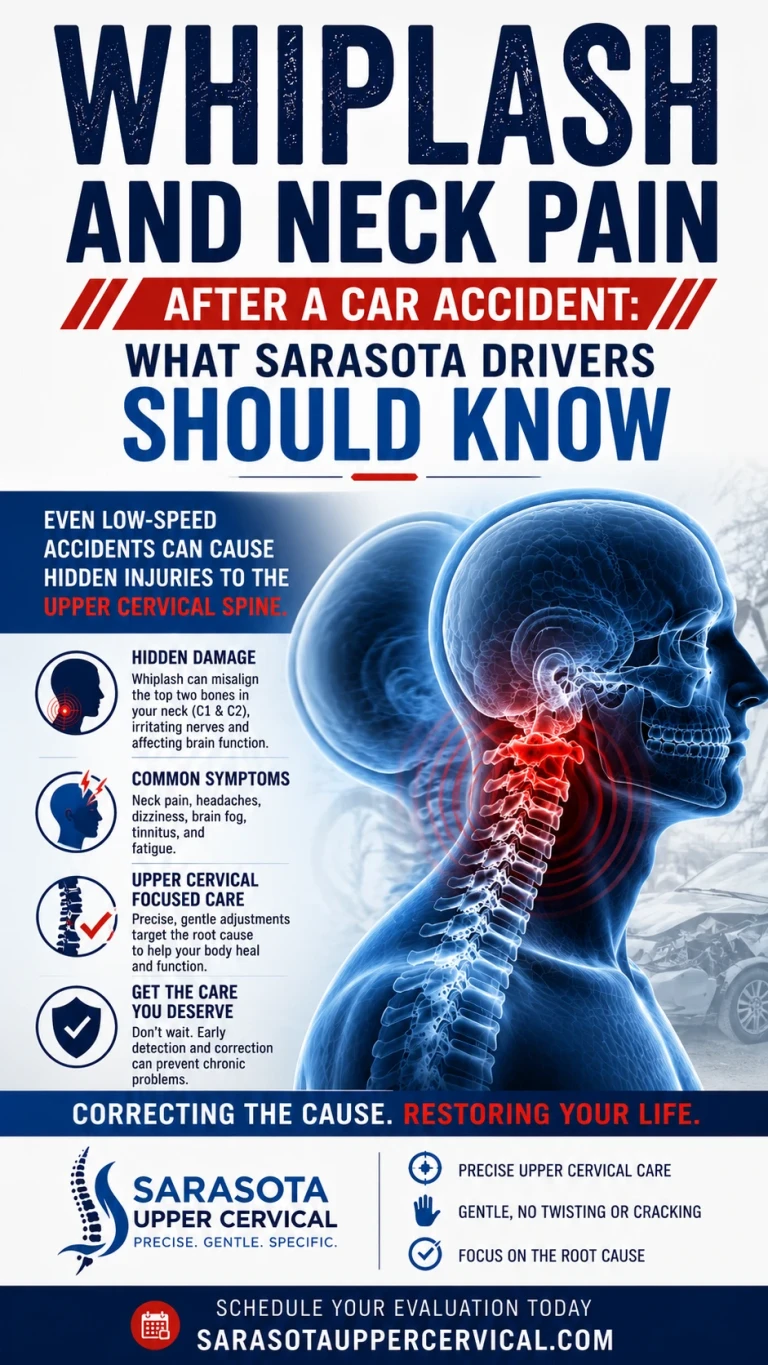
Whiplash and Neck Pain After a Car Accident: What Sarasota Drivers Should Know
Jul 19, 2026Restoring structural alignment
Upper cervical chiropractic correction restores the atlas to its proper structural relationship with the skull above and the axis below. The correction is specific to the upper cervical segment, delivered with precision based on three-dimensional cone beam CT imaging measurements. The force used is low — there is no twisting, no popping, no full-spine manipulation. The precision matters particularly for patients whose proprioceptive systems are sensitized from prolonged distorted input.
Allowing muscle normalization
Once structural alignment is restored, the compensatory muscle tension that had developed begins to resolve. The suboccipital muscles can return to their normal resting length and tension patterns. This process is gradual — the muscles have adapted to the abnormal pattern over time and require weeks to months to return fully to normal. As the muscles normalize, their proprioceptive signaling becomes more accurate, sending signals that reflect normal muscle states rather than the compensatory pattern.
Resolving sensory conflict
As the proprioceptive input from the corrected C1 becomes more accurate, the integration at the brainstem produces less conflict. The vestibular nuclei receive proprioceptive input that matches the vestibular and visual input, allowing coherent integration. The cortical processing produces more accurate awareness of position and motion. The cumulative effect is reduction of the symptoms that arose from the original sensory conflict.
Joint position error improvement
As proprioceptive accuracy improves, joint position error gradually decreases. Patients can more accurately sense their head position. The cervical proprioceptive retraining that vestibular rehabilitation provides becomes more effective because it is now working with a structurally normal C1 rather than a misaligned one. The combination of structural correction and proprioceptive retraining often produces better outcomes than either alone.
The timeline of response
Patients should expect gradual rather than immediate improvement. The structural correction is performed in a single session or over multiple sessions, but the muscular and neurological adaptations that produce symptom resolution take weeks to months. The chronically tense muscles need time to return to normal. The proprioceptive system needs time to recalibrate based on the new accurate input. The brain's central processing needs time to adjust to the changed sensory environment. Throughout this process, patients typically notice gradual symptom improvement as the system normalizes.
Honest Framing of the Evidence
Patients considering upper cervical evaluation for proprioceptive contributions to their symptoms should understand the evidence landscape clearly.
What is well-established
The neuroscience supporting cervical proprioception's role in balance is well-established. The dense receptor populations in the upper cervical region (McLain 1994, Kulkarni 2001), the direct neural pathways to the vestibular nuclei (Gdowski & McCrea 2000), the joint position error in patients with cervical dizziness (Treleaven 2003), and the broader cervicogenic dizziness framework (Reiley 2017, Peng 2022) all rest on mainstream peer-reviewed research. The basic principle that cervical proprioception affects balance, and that distortion of this proprioception can produce balance symptoms, is established neuroscience.
What this means for patient decisions
Patients with persistent vestibular symptoms that may have cervical proprioceptive contribution should consider upper cervical evaluation as one component of comprehensive evaluation alongside continued standard care. The evaluation may identify structural problems that, when corrected, may support better balance function. The reasoning is anatomically and physiologically sound; the trial-level evidence specific to upper cervical care for this purpose is more limited. Realistic expectations and continued engagement with appropriate standard treatments matter.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation may be worth considering when any of the following are true:
You have persistent unsteadiness, dizziness, or motion sensitivity that varies with head and neck position. You have associated cervical symptoms (chronic neck pain, suboccipital tension, restricted range of motion, cervicogenic headache) alongside your balance symptoms. Your symptoms developed after head or neck trauma — concussion, whiplash, sports injury, or fall. You have a clinical picture suggesting cervicogenic dizziness or you have been told your symptoms may have cervical contribution. Your vestibular symptoms have not responded fully to standard treatment. You have prior concussions or significant neck trauma layered on top of your current symptoms. You have post-traumatic vestibular migraine, post-traumatic PPPD, or stalled recovery from a vestibular event.
For patients with vestibular symptoms responding to standard treatment, patients with BPPV requiring canalith repositioning, patients in acute phases requiring medical evaluation, and patients with conditions that are not particularly related to cervical mechanisms, upper cervical evaluation is not the appropriate first step. Standard medical and rehabilitation care should remain the focus.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Where to Go From Here
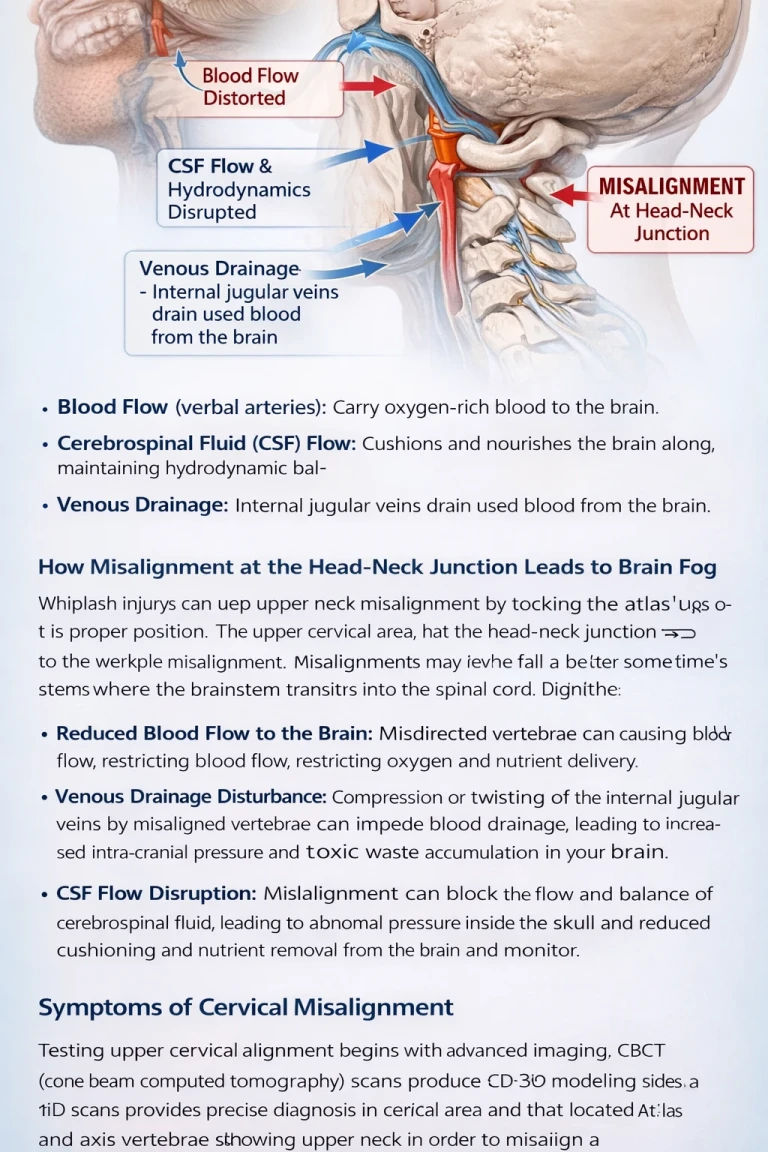
The atlas (C1) is one of the most proprioceptively important structures in the body, with dense joint mechanoreceptors and exceptionally rich muscle spindle populations in the surrounding suboccipital muscles. The proprioceptive input from this region travels directly to the brainstem vestibular nuclei where it is integrated with vestibular and visual input to produce coherent balance processing. When C1 is misaligned, the proprioceptive system sends distorted information to the brain, producing sensory conflict that can manifest as persistent unsteadiness, motion sensitivity, dizziness, and the broader symptoms of cervicogenic dizziness and related conditions.
For patients in Sarasota and surrounding communities with persistent balance symptoms that may have cervical proprioceptive contribution, upper cervical evaluation focused on the atlas can be a meaningful component of comprehensive care. The evaluation identifies whether C1 misalignment is present, and if so, structural correction can address the root cause of the proprioceptive distortion. The approach should be pursued alongside continued standard medical care and vestibular rehabilitation when appropriate, with realistic expectations about gradual improvement as the proprioceptive system normalizes.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
Gdowski, G. T., & McCrea, R. A. (2000). Neck proprioceptive inputs to primate vestibular nucleus neurons. Experimental Brain Research, 135(4), 511–526.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Treleaven, J., Jull, G., & Sterling, M. (2003). Dizziness and unsteadiness following whiplash injury: Characteristic features and relationship with cervical joint position error. Journal of Rehabilitation Medicine, 35(1), 36–43.
Peng, B., Yang, L., Yang, C., Pang, X., Chen, X., & Wu, Y. (2022). Proprioceptive cervicogenic dizziness: A narrative review of pathogenesis, diagnosis, and treatment. Journal of Clinical Medicine, 11(21), 6293.
Reiley, A. S., Vickory, F. M., Funderburg, S. E., Cesario, R. A., & Clendaniel, R. A. (2017). How to diagnose cervicogenic dizziness. Archives of Physiotherapy, 7, 12.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with persistent vestibular symptoms should pursue appropriate medical evaluation including consultation with otolaryngology, neurology, or other appropriate specialists to establish accurate diagnosis. Standard evidence-based treatments for each specific vestibular condition should form the foundation of care. Upper cervical evaluation should be considered only for specific patient subsets as a complementary approach alongside continued standard medical management. Patients with acute severe vertigo, new neurological symptoms, sudden hearing loss, or significant vascular risk factors should seek urgent medical evaluation. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment