
"How the craniocervical junction influences brain blood flow, CSF drainage, and quality of life — and what published case-series research suggests about upper cervical chiropractic care"
Parkinson’s disease is one of the hardest diagnoses for a family to absorb. The tremor, the rigidity, the slowing of movement, the changes in voice and balance — they advance on their own timeline, and the standard medical treatments, while important, often leave patients searching for anything that can preserve quality of life along the way.
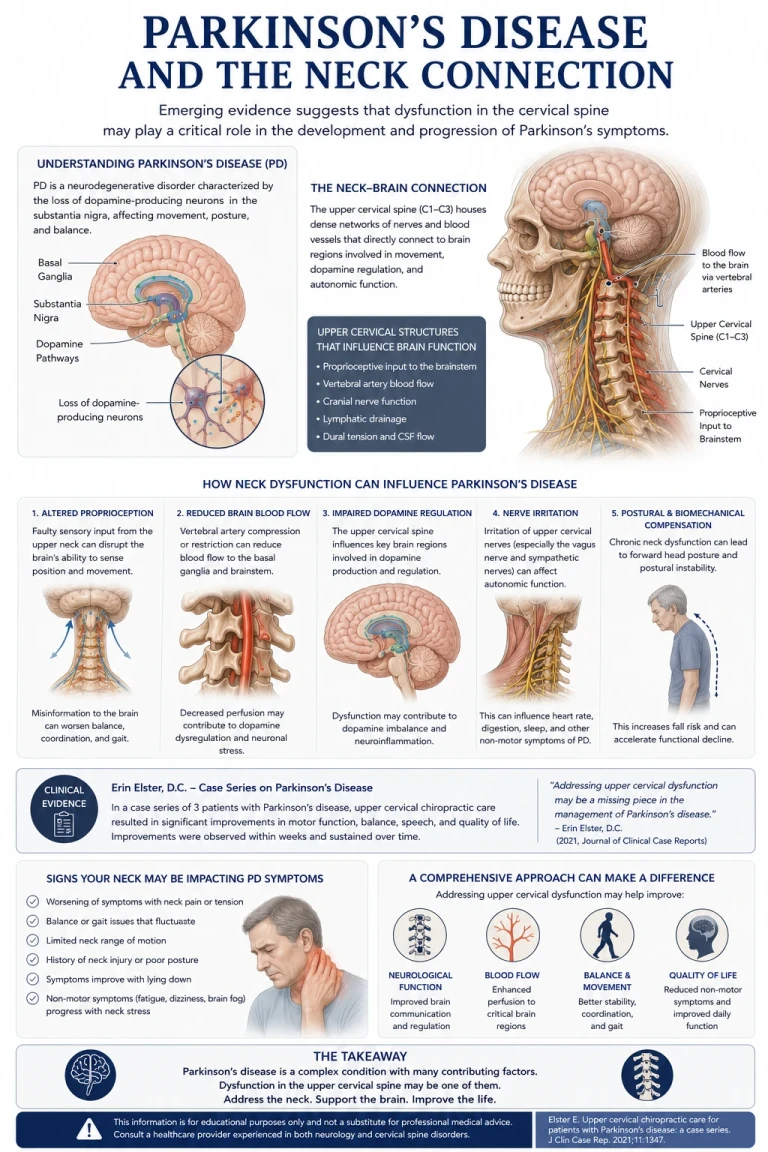
There is a body of clinical research, building since 2000, that asks a different question: what role does the top of the neck play in this disease? Specifically, what happens when the joint between the skull and the first vertebra — the craniocervical junction — is misaligned, and what changes when that misalignment is corrected? The answers are not a cure. But for many patients, they have meant a meaningful difference in how they feel and function.
The Research: Erin Elster’s Case Series and Case Reports
In 2000, upper cervical chiropractor Dr. Erin Elster published a peer-reviewed case report in the Journal of Manipulative and Physiological Therapeutics describing a 60-year-old man with Parkinson’s disease who improved measurably on the Unified Parkinson’s Disease Rating Scale (UPDRS) after nine months of upper cervical chiropractic care. The patient had a history of multiple prior head and neck injuries, and his upper cervical spine showed misalignment on precision radiographs.
In 2004, Dr. Elster published a larger retrospective analysis of 81 patients with neurodegenerative conditions — 44 with multiple sclerosis and 37 with Parkinson’s disease — all of whom presented with upper cervical misalignments and a history of prior head or neck trauma. Of the 37 Parkinson’s patients, 34 (about 92 percent) reported symptomatic improvement, and the disease did not progress further while they were under care. A 2014 case series published by Malachowski and Rubinstein reported similar improvements in Parkinson’s patients receiving a specific upper cervical chiropractic protocol.
These are case-series studies, not randomized controlled trials. They cannot prove that upper cervical care reverses Parkinson’s, and they were not designed to. What they do show is a consistent clinical pattern in patients who had run out of conventional options — patients getting better, in measurable ways, after the upper cervical spine was addressed. That pattern is significant enough that it deserves a closer look at the mechanism.
The Craniocervical Junction: A Choke Point for the Brain
The craniocervical junction (CCJ) is the anatomical region where the skull meets the atlas (C1) and axis (C2). Almost everything the brain depends on physically passes through this small area. The brainstem and upper spinal cord. The vertebral arteries supplying the back of the brain. The internal jugular veins draining blood out of the skull. The cerebrospinal fluid (CSF) channels that connect the brain to the rest of the central nervous system. Cranial nerves IX through XII.
The medical literature increasingly describes this region as a “choke point.” A 2015 paper in the Journal of Translational Medicine, summarized in PubMed Central, proposed that misalignments and malformations of the craniocervical junction may contribute to neurodegenerative conditions through their effects on CSF flow and venous drainage. When the CCJ is aligned and moving well, fluid moves through cleanly. When it is not, three things can happen at the same time, and each one matters for a Parkinson’s brain.
Three Things a Misalignment Can Disrupt
First, arterial blood flow can be reduced. The vertebral arteries pass through small openings in the upper cervical vertebrae on their way to supply the brainstem, cerebellum, and the deep structures of the brain — including the basal ganglia, where Parkinson’s disease originates. A misalignment can place mechanical stress on these vessels and reduce the volume of blood reaching the back of the brain.
Second, jugular venous drainage can be impaired. The internal jugular vein passes directly in front of the atlas on its way down the neck. When the atlas is rotated or shifted, the vein can be partially compressed, slowing the rate at which blood drains out of the skull. Blood that doesn’t drain efficiently is blood that backs up, and that pressure has to go somewhere.
Third, CSF flow and intracranial pressure can be affected. Cerebrospinal fluid is what bathes, cushions, and cleans the brain. It also plays a critical role in waste clearance — including the clearance of the misfolded proteins that accumulate in Parkinson’s disease. CSF moves between the skull and the spine through the same narrow passage at the craniocervical junction. When that passage is mechanically distorted, CSF flow becomes turbulent or restricted, intracranial pressure can rise, and the brain’s built-in cleaning system loses efficiency.
Reduced arterial inflow. Restricted venous outflow. Disrupted CSF dynamics. All three of these can occur simultaneously when the craniocervical junction is misaligned, and all three matter for brain function.
What Patients Notice: Muscle Tone, Movement, and Quality of Life
Beyond the vascular and fluid mechanics, the upper cervical spine is one of the densest mechanoreceptor regions in the body. Its input goes directly into the brainstem, where it helps coordinate muscle tone throughout the entire body. For a Parkinson’s patient, whose disease is partly defined by rigidity and abnormal muscle tone, the quality of that input matters.
When a misalignment is corrected, patients commonly report that their muscles feel less tight, their movement feels less effortful, their sleep improves, and the activities of daily living — dressing, walking, getting in and out of a chair — become easier. These are not cures. The disease is still there. But the patient’s functional reserve, the margin between what they can do and what the disease is taking from them, gets a little wider. Over months of care, that wider margin shows up as a real difference in quality of life.
This is consistent with what Elster’s patients reported, what the Malachowski and Rubinstein case series described, and what we see in our own practice when patients come in with a Parkinson’s diagnosis and a history of prior head or neck trauma.
CBCT Imaging: Precision Before Anything Else
Before any care begins in our Sarasota office, we use Cone Beam Computed Tomography (CBCT) imaging of the upper cervical spine. CBCT is a precision imaging tool that produces three-dimensional views of the skull base, atlas, axis, and surrounding structures — detail that flat two-dimensional X-rays cannot provide.
Every craniocervical junction is built differently. The angles, the orientations, and the relationships between the skull, C1, and C2 are unique to each person. Without precision measurements, an upper cervical correction is a guess. With them, the correction can be specific, gentle, and tailored to your anatomy.
For a patient with Parkinson’s, this matters even more. The disease changes posture, muscle tone, and balance. A non-specific, force-based approach is not appropriate. Precision imaging allows us to see exactly what we are working with and to plan a correction that respects the disease, the anatomy, and the individual.
No Twisting. No Cracking. No Pulling of the Neck
Most people picture a chiropractic adjustment as a fast head-turn and a popping sound. That is not what we do. The correction we deliver is specific, low-force, and based directly on the measurements taken from your CBCT scan. There is no twisting, cranking, or pulling. No cavitation noise. You lie on your side with your head supported. The correction takes seconds.
For a Parkinson’s patient, this is essential. The nervous system is already under load. A forceful manipulation is the wrong tool. Our approach is built specifically to give the brainstem cleaner input from the upper cervical joints — and to let the natural mechanics of the craniocervical junction restore themselves — without adding stress to a system that is already working hard.
What a Realistic Conversation Looks Like
Upper cervical chiropractic care does not cure Parkinson’s disease, and we do not claim it does. What it can do, in patients who have an upper cervical component to their case, is help normalize the factors at the craniocervical junction — muscle tone, blood flow, fluid dynamics, mechanoreceptor input — that influence how the brain functions day to day. The goal is to give the body its best chance to work with the disease, not against it.
A first visit in our Sarasota office includes a thorough consultation, a focused examination, and CBCT imaging of the upper cervical spine. We pay particular attention to your history of head and neck trauma — falls, accidents, concussions, whiplash — because the published research consistently identifies prior trauma as a thread running through these cases. After we review the imaging with you, we will tell you honestly whether upper cervical care looks like a good fit. If it is, we build a plan. If it is not, we say so.
If You’re in Sarasota and Living with Parkinson’s
Parkinson’s asks a lot of patients and families. Anything that helps the body function better — even modestly — is worth understanding. The published case-series research on upper cervical chiropractic care for Parkinson’s is not a cure, but it has been consistent enough, for long enough, to take seriously. Combined with what we now understand about the craniocervical junction’s role in brain blood flow and CSF dynamics, the case for at least evaluating the upper cervical spine in a Parkinson’s patient is strong.
If you or a loved one has been diagnosed with Parkinson’s and you want to understand whether the upper cervical spine could be part of the picture, the first step is a conversation. We will look at your history, image your craniocervical junction, and give you a straight answer about whether this approach makes sense for you.
Ready to take the next step? Schedule a consultation at our Sarasota office to find out whether upper cervical chiropractic care could fit into your Parkinson’s care plan.
References:
Elster EL. Upper cervical chiropractic management of a patient with Parkinson’s disease: a case report. J Manipulative Physiol Ther. 2000;23(8):573-577. • Elster E. Eighty-One Patients with Multiple Sclerosis and Parkinson’s Disease Undergoing Upper Cervical Chiropractic Care to Correct Vertebral Subluxation: A Retrospective Analysis. J Vertebral Subluxation Res. 2004. • Malachowski T, Rubinstein R. Improved Health Outcomes in Parkinson’s Disease Utilizing Specific Upper Cervical Chiropractic Protocol: A Case Series. J Upper Cervical Chiropr Res. 2014. • Flanagan MF. The Role of the Craniocervical Junction in Craniospinal Hydrodynamics and Neurodegenerative Conditions. Neurol Res Int. 2015.
Disclaimer: This article is for educational purposes only and does not constitute medical advice or a substitute for care from your neurologist. Upper cervical chiropractic care does not diagnose, treat, or cure Parkinson’s disease. The case-series research cited above describes observed clinical improvements but does not constitute proof of efficacy. Individual results vary. Patients with Parkinson’s disease should continue working with their medical team.



Leave a comment