
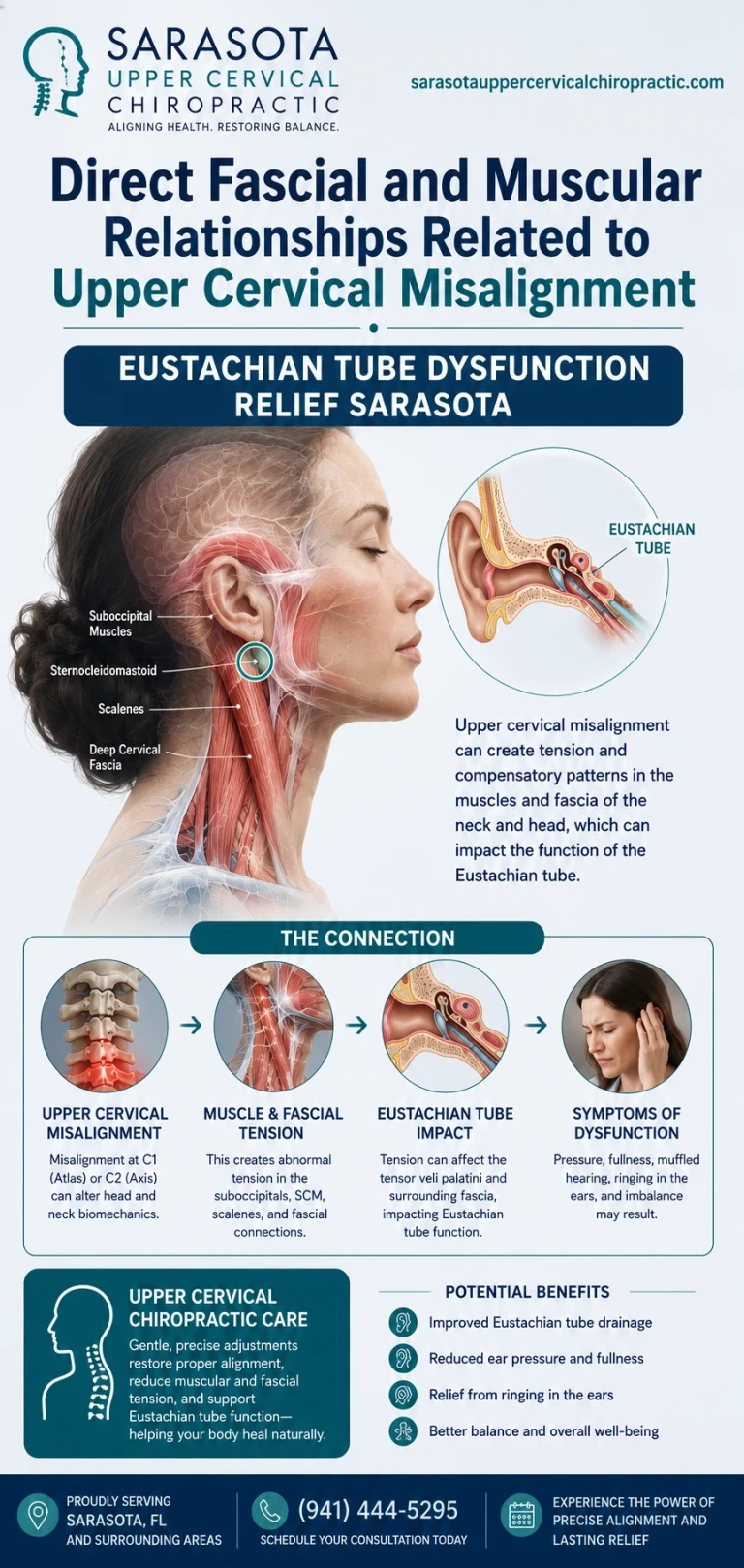
"The Eustachian tube does not sit in isolation. Its function depends on muscles and fascial systems that connect directly to the upper cervical region. Understanding these anatomical relationships clarifies why structural problems at the craniocervical junction may contribute to Eustachian tube dysfunction in appropriate patients"
The Eustachian tube is often discussed as if it were a simple anatomical pipe — a tube that opens to equalize pressure and closes to protect the middle ear. The reality is substantially more complex. The tube is embedded within a tightly interconnected anatomical system that includes specific muscles for opening it, fascial layers that surround and influence it, and direct connections to structures throughout the head and neck. Among these connections, the relationships to the upper cervical region are particularly notable. The muscles that open the Eustachian tube share fascial connections with the deep cervical musculature. The fascial layers around the tube are continuous with the cervical fascia. And the upper cervical structures themselves attach to muscles that have direct anatomical relationships with the pharyngeal and Eustachian tube region.
Schedule Your Appointment
Schedule appointmentTo schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
For patients with persistent Eustachian tube dysfunction (ETD), these anatomical relationships matter. The 2015 consensus statement on ETD by Schilder and colleagues in Clinical Otolaryngology established the framework for understanding ETD as a clinical entity with multiple potential contributors (Schilder et al., 2015), and the muscular and fascial relationships to the upper cervical region represent one potential contributor that standard medical workups do not typically address. For patients whose ETD has not resolved with standard otolaryngology care, understanding these anatomical relationships clarifies why upper cervical evaluation may be reasonable to consider as part of comprehensive care.
This article walks through the specific muscles that open and close the Eustachian tube, the fascial systems that connect the tube region to the upper cervical structures, the deep cervical musculature that has direct relationships to pharyngeal and tubal anatomy, the dural and connective tissue continuities between the upper cervical region and intracranial structures, the proposed mechanisms by which upper cervical misalignment could affect this anatomical system, and honest framing of the evidence supporting upper cervical evaluation for appropriate ETD patients.
The Muscles That Control the Eustachian Tube
Eustachian tube function depends critically on specific muscles that actively open and close the tube. Understanding these muscles and their attachments clarifies how the tube is anatomically integrated with surrounding structures including the upper cervical region.
The tensor veli palatini
The tensor veli palatini is the primary muscle responsible for active Eustachian tube opening. The muscle originates from the sphenoid bone (specifically the scaphoid fossa and the spine of the sphenoid), from the lateral cartilage of the auditory tube itself, and from surrounding fascial structures. Its tendon passes around the pterygoid hamulus (a small bony projection from the medial pterygoid plate) before spreading into the palatine aponeurosis. When the muscle contracts — typically during swallowing or yawning — it pulls on the cartilage of the Eustachian tube, opening the tube to allow pressure equalization and drainage.
The levator veli palatini
The levator veli palatini works alongside the tensor in producing Eustachian tube opening, though its role is somewhat different. The muscle originates from the petrous part of the temporal bone and from the cartilage of the auditory tube. It runs downward and medially into the soft palate. Its action contributes to soft palate elevation during swallowing, which assists tube opening through related mechanical effects. The muscle's attachments to the temporal bone create direct relationships with the skull base structures that the upper cervical region articulates with.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The salpingopharyngeus
The salpingopharyngeus muscle originates from the cartilage of the auditory tube near its opening at the nasopharynx and runs downward to blend with the palatopharyngeus muscle. The muscle contributes to elevation of the pharynx during swallowing, which has secondary effects on Eustachian tube function. The muscle's attachment to the tube cartilage means that pharyngeal mechanics directly affect the tube's mechanical environment.
Why these muscles' relationships matter
The muscles controlling the Eustachian tube do not operate in isolation. They share fascial connections with the broader pharyngeal musculature, with the cervical musculature through deep fascial continuities, and with the skull base structures that articulate with the upper cervical region. Mechanical or postural problems affecting any of these connected structures can potentially influence the function of the tube-controlling muscles, with consequences for tube opening, closing, and overall function.
The Fascial Continuities Between Upper Cervical and Eustachian Tube Regions
Fascial systems in the head and neck are not isolated planes but interconnected continuums that create mechanical relationships between distant structures. Understanding the fascial anatomy between the upper cervical region and the Eustachian tube region clarifies how mechanical changes in one region can potentially propagate to the other.
The pharyngobasilar fascia
The pharyngobasilar fascia is a dense fibrous layer that lines the upper pharynx and attaches to the base of the skull. This fascia forms part of the structural environment surrounding the upper end of the Eustachian tube. Importantly, the pharyngobasilar fascia is continuous with the buccopharyngeal fascia and connects to broader fascial systems including those reaching the cervical region. The fascia is not a closed compartment but part of an interconnected fascial framework.
Related article
The prevertebral fascia
The prevertebral fascia is the deepest layer of the deep cervical fascia, lying anterior to the cervical vertebrae and covering the deep cervical musculature (the longus capitis, longus colli, and other prevertebral muscles). This fascia is continuous with the cranial dura mater at the skull base and with fascial layers around the pharyngeal structures. The prevertebral fascia creates a direct fascial link between the upper cervical structures and the structures surrounding the Eustachian tube.
The buccopharyngeal fascia
The buccopharyngeal fascia surrounds the pharyngeal constrictor muscles and creates the outer fascial layer of the pharyngeal compartment. This fascia connects with the prevertebral fascia of the cervical region and with the pharyngobasilar fascia around the upper pharynx and Eustachian tube. The fascial continuity creates a mechanical pathway between the cervical region and the structures around the tube.
The retropharyngeal space
The retropharyngeal space lies between the buccopharyngeal fascia and the prevertebral fascia, extending from the skull base down into the upper thorax. This space, while a potential space rather than an open cavity, represents a continuous communication pathway between cervical and pharyngeal regions. Mechanical changes affecting the boundaries of this space — through cervical structural problems or other mechanisms — can potentially affect the surrounding structures including those related to Eustachian tube function.
Why fascial continuity matters mechanically
Fascial continuity creates mechanical coupling between distant structures. When fascial layers are continuous from the upper cervical region to the structures around the Eustachian tube, mechanical tension changes can propagate along these connections. Postural changes, structural misalignment, or tissue adaptations in the cervical region can produce subtle but real changes in the fascial tension reaching the tube region. The clinical significance of these mechanical relationships in any given patient varies, but the anatomical basis for the relationships is well-established.
The Deep Cervical Musculature and Its Connections
Several deep cervical muscles have direct anatomical relationships with the pharyngeal and Eustachian tube region. Understanding these muscles and their connections clarifies how cervical structural problems affecting these muscles could potentially affect tube function.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The longus capitis
The longus capitis is one of the deep prevertebral cervical muscles, running from the upper cervical transverse processes (C3-C6) to attach to the inferior surface of the basilar part of the occipital bone (basiocciput). The muscle lies anterior to the cervical vertebrae and immediately posterior to the pharyngeal structures. Its position means that the muscle is in direct anatomical relationship with the pharyngeal region including the area surrounding the Eustachian tube opening. Changes in longus capitis tension — common with cervical postural problems and structural misalignment — can potentially affect the mechanical environment of adjacent pharyngeal structures.
The longus colli
The longus colli is the second major prevertebral muscle, running along the anterior surface of the cervical and upper thoracic spine. Like the longus capitis, it lies anterior to the vertebrae and posterior to the pharyngeal structures. The muscle's three divisions (superior oblique, vertical, inferior oblique) create a complex pattern of cervical stabilization, with weakness or dysfunction in this muscle being common in patients with cervicogenic symptoms. Longus colli dysfunction can affect cervical mechanics broadly with potential downstream effects on the connected structures.
The suboccipital musculature
The deep suboccipital muscles — rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis superior, and obliquus capitis inferior — are the smallest and deepest muscles of the cervical region. They connect the skull (occiput) to the upper cervical vertebrae (atlas and axis) and provide fine motor control of the head on the neck. These muscles are densely packed with proprioceptive receptors (Kulkarni et al., 2001), and their tension states substantially affect upper cervical mechanics. Suboccipital muscle dysfunction is common in patients with cervicogenic conditions and can affect the broader cervical mechanical environment.
The myodural bridge
One of the most clinically significant anatomical findings relating cervical musculature to deeper structures is the myodural bridge. The 1995 paper by Hack and colleagues in Spine documented direct connective tissue continuity between the rectus capitis posterior minor muscle (a deep suboccipital muscle) and the spinal dura mater (Hack et al., 1995). This anatomical continuity demonstrates that cervical muscular tension directly affects the dural environment of the upper spinal cord and brainstem. While the myodural bridge does not directly connect to the Eustachian tube, its existence demonstrates the principle that cervical musculature has direct connective tissue relationships with structures far beyond the immediate cervical region — relationships that include the dural and fascial systems reaching the cranial structures.
Connections to pharyngeal mechanics
The deep cervical muscles described above have indirect but real connections to pharyngeal mechanics through their fascial relationships and their effects on overall cervical posture and function. Changes in head and neck position produced by cervical muscular dysfunction can affect pharyngeal geometry, potentially affecting the mechanical environment of the Eustachian tube. While the connections are indirect rather than direct muscle-to-muscle attachments, the mechanical effects can be real.
Proposed Mechanisms: How Upper Cervical Misalignment May Affect Eustachian Tube Function
With the anatomical relationships established, the proposed mechanisms by which upper cervical structural problems could affect Eustachian tube function become clearer. Understanding the proposed mechanisms — while maintaining honest framing about clinical evidence — helps patients consider whether upper cervical evaluation may be relevant for their situation.
Direct fascial tension effects
Structural misalignment in the upper cervical region can produce altered fascial tension throughout the connected fascial systems. The prevertebral fascia attaching to the misaligned segments may exert altered tension on its continuous fascial connections, including those reaching the pharyngobasilar fascia around the Eustachian tube. These altered tensions could potentially affect the mechanical environment of the tube and the muscles that control it.
Effects through skull base mechanics
The upper cervical structures (atlas and axis) articulate directly with the skull at the craniocervical junction. Misalignment at this junction can produce subtle effects on skull base mechanics — altered position of the occiput, altered tension across the dural attachments, altered relationships between the temporal bones and surrounding structures. Since the tensor veli palatini and levator veli palatini both originate from skull base structures (sphenoid and temporal bones respectively), changes in skull base mechanics could potentially affect these muscles' resting tension and function.
Related article
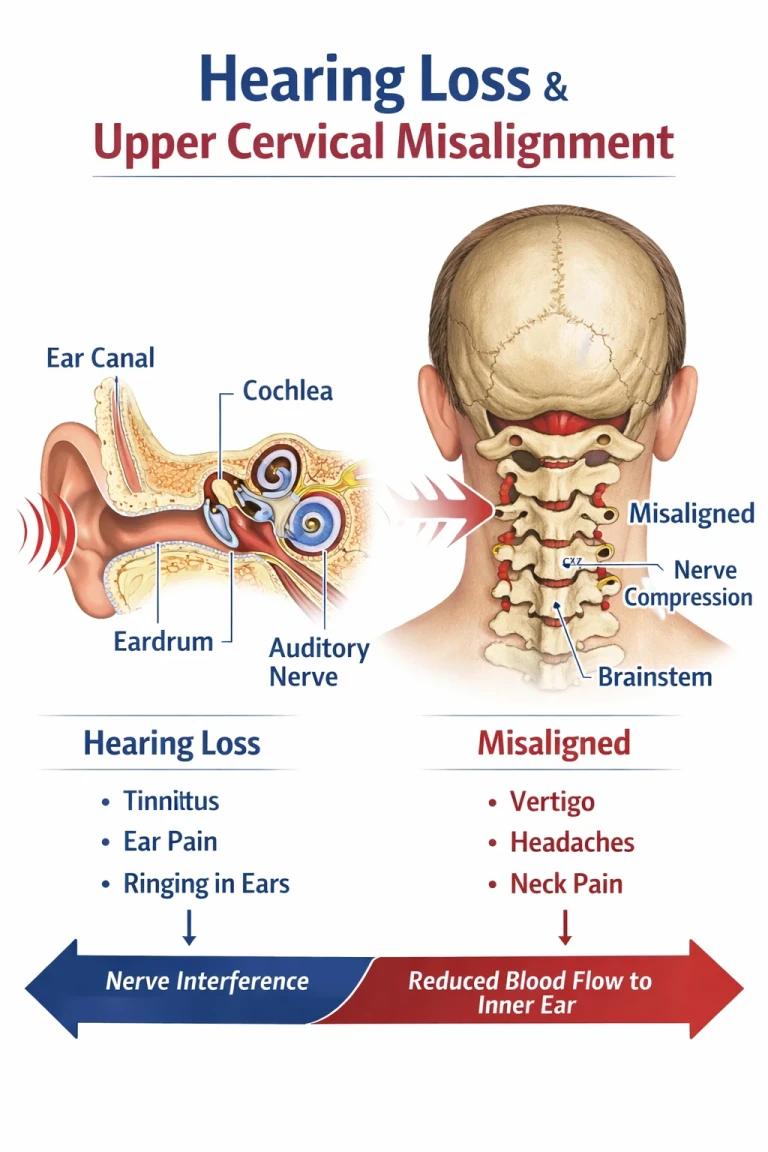
Hearing Loss Treatment in Sarasota | Understanding Eustachian Tube Dysfunction
Mar 23, 2026Effects on pharyngeal mechanics
Cervical postural changes — particularly forward head posture and altered upper cervical alignment — can affect pharyngeal mechanics. The pharynx is geometrically affected by the position of its boney attachments, and the cervical structures form important reference points for these attachments. Altered cervical position can change pharyngeal geometry subtly, with potential effects on the mechanical environment of the Eustachian tube opening.
Effects on deep cervical muscular function
Upper cervical structural problems often produce compensatory changes in the deep cervical musculature — the longus capitis, longus colli, and suboccipital muscles. These muscular changes can affect the broader cervical and pharyngeal mechanical environment. While the muscles do not directly attach to the Eustachian tube, their effects on the connected fascial systems and on overall cervical posture can have downstream effects on tube function.
Combined mechanical effects
In appropriate patients, the combined effects of altered fascial tension, altered skull base mechanics, altered pharyngeal geometry, and altered cervical muscular function could produce a meaningful mechanical impact on Eustachian tube function. The effects in any given patient depend on the specific structural problems present, the patient's overall mechanical adaptation, and other factors. The mechanical reasoning is anatomically sound; the clinical magnitude of these effects in individual patients varies.
Honest Framing of the Evidence
Patients considering upper cervical evaluation for Eustachian tube dysfunction should understand the evidence landscape clearly. The anatomical relationships described in this article are well-established; the clinical significance of these relationships for any individual ETD patient is less definitively established.
What is anatomically established
The muscular and fascial relationships between the upper cervical region and the Eustachian tube region are established anatomy. The continuity of fascial systems, the mechanical relationships between cervical and pharyngeal structures, the myodural bridge connecting cervical muscles to spinal dura, and the broader principle that the cervical region has direct anatomical connections to head and neck structures including those around the Eustachian tube — all of these are anatomically established and not controversial.
What is not established at the clinical trial level
What has not been established through randomized controlled trials is the clinical effectiveness of upper cervical chiropractic care specifically for Eustachian tube dysfunction. No RCTs specifically test upper cervical evaluation as treatment for ETD. The case for considering upper cervical evaluation in appropriate ETD patients rests on anatomical reasoning and clinical observation, not on trial-level evidence specific to this intervention for this condition.
What this means for patient decisions
Patients with persistent ETD considering upper cervical evaluation should understand that the evaluation represents a hypothesis-driven consideration based on anatomical relationships rather than an established treatment supported by formal clinical research. The evaluation may be reasonable for appropriate patients — those with persistent ETD not responding to standard treatments, those with concurrent cervical symptoms, those with trauma history affecting both regions — but should be pursued with realistic expectations and alongside continued standard otolaryngology care.
Which ETD Patients May Benefit From Upper Cervical Evaluation
Upper cervical evaluation is not appropriate for every ETD patient. Identifying the specific subsets where the evaluation may be reasonable to consider helps patients make informed decisions.
Persistent ETD with concurrent cervical symptoms
Patients whose Eustachian tube dysfunction persists alongside chronic cervical symptoms — neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern — may have layered presentations where cervical structural problems contribute to the broader picture. The cervical evaluation in these patients addresses one specific potential contributor that standard ETD treatments do not specifically target.
Post-traumatic ETD
ETD that developed after head or neck trauma — concussion, whiplash, fall, sports injury — often involves cervical structural injury alongside any direct effects on the inner ear or Eustachian tube region. A 2005 study by Kaale and colleagues in the Journal of Neurotrauma documented upper cervical ligamentous injuries from whiplash mechanisms at forces below those required for diagnosable concussion (Kaale et al., 2005). When trauma was sufficient to affect ETD, the upper cervical structures have typically experienced forces well above the threshold for their own injury. For these patients, cervical evaluation addresses the structural component that often persists after the immediate trauma effects have stabilized.
ETD with poor response to standard treatment
Patients whose Eustachian tube dysfunction has not responded adequately to standard medical management — addressing allergies and environmental triggers, optimizing nasal corticosteroids, treating any underlying sinusitis, considering pressure equalization techniques, and other evidence-based ETD treatments — may consider additional approaches alongside continued standard care. Upper cervical evaluation can be one component of comprehensive evaluation for these treatment-resistant cases.
ETD with broader head and neck dysfunction
Patients with ETD alongside other features of broader head and neck dysfunction — cervicogenic headache, TMJ involvement, cervicogenic dizziness, vestibular features, or other symptoms suggesting a broader cervical-related picture — may have systemic patterns that include the ETD as one component. Upper cervical evaluation in this broader context addresses the cervical contribution to the overall picture.
When upper cervical evaluation is not particularly indicated
For patients with acute Eustachian tube dysfunction responding to standard treatment, patients with ETD clearly explained by allergies or specific environmental factors, patients without concurrent cervical symptoms or trauma history, and patients in the acute phase of any ear or sinus pathology requiring medical evaluation, upper cervical evaluation is not particularly indicated. Standard medical management should remain the focus.
How an Upper Cervical Evaluation Works
For appropriate ETD patients, upper cervical chiropractic focuses specifically on the precise structural relationship between the skull, atlas, and axis — the region most directly relevant to the muscular and fascial connections discussed throughout this article.
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree. The imaging identifies the specific structural problems that may be relevant. For patients with ETD and suspected mechanical involvement, the imaging provides objective measurement of the structural picture rather than subjective assessment.
Related article
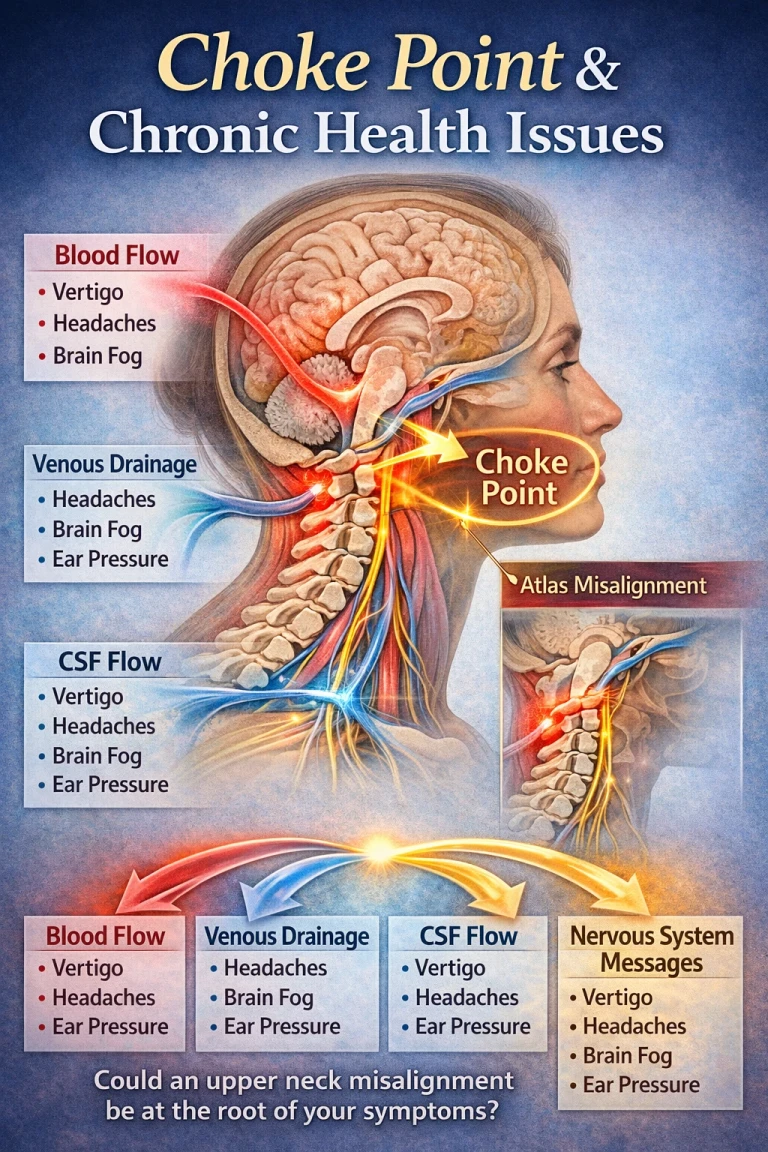
The Upper Neck as a Choke Point: Vertigo, Headaches, Brain Fog, and Ear Pressure
Apr 21, 2026Objective testing before any intervention
Leg length analysis and paraspinal infrared thermography are performed before any adjustment, and corrections are only delivered when objective findings indicate a structural shift. The principle of restraint guided by data is appropriate for ETD patients — the cervical correction is only performed when objective findings support it.
Precision without manipulation
Corrections are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. The precision is essential for ETD patients — aggressive cervical manipulation could potentially aggravate the broader mechanical picture and is not appropriate for this presentation.
Integration With Standard ETD Care
When upper cervical evaluation is appropriate, it should be added to standard ETD care rather than substituted for it.
Otolaryngology follow-up continues
Patients should maintain appropriate otolaryngology follow-up. Standard ETD management — allergy and environmental factor management, nasal corticosteroids when appropriate, treatment of underlying sinusitis, evaluation for any structural pathology, consideration of pressure equalization techniques — should continue. The standard care addresses the immediate ETD picture; upper cervical care addresses one potential contributing factor.
Realistic timeframe expectations
If upper cervical correction is going to produce benefit for ETD, the response is typically gradual over weeks to months rather than immediate. The cervical correction does not directly heal the Eustachian tube or instantly resolve mucosal congestion. It addresses one mechanical factor that may have been contributing to the broader picture, with effects accruing as the surrounding tissues adapt to the corrected mechanics.
Honest evaluation of outcomes
Patients should evaluate outcomes honestly. Improvement in ETD with upper cervical care is the desired outcome; lack of improvement does not indicate the diagnosis was wrong but rather that the cervical contribution to this particular patient's ETD was limited. Either outcome provides useful clinical information.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation may be worth considering for ETD patients when any of the following are true:
Your Eustachian tube dysfunction has not responded adequately to standard medical management despite consistent treatment. You have concurrent cervical symptoms — chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern — alongside your ETD. Your ETD developed after head or neck trauma affecting both regions. You have broader head and neck dysfunction features alongside the ETD. You have prior concussions or significant neck trauma layered on top of the current presentation. Your symptoms vary significantly with head or neck position. You have features suggesting upper cervical involvement (cervicogenic headache, cervicogenic dizziness, post-traumatic features).
For patients with acute or straightforward ETD responding to standard treatment, without concurrent cervical symptoms or trauma history, the case for upper cervical evaluation is weak. Standard medical management should remain the focus, and otolaryngology follow-up should continue as primary care.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Where to Go From Here
The muscular and fascial relationships between the upper cervical region and the Eustachian tube region are well-established anatomy. The tensor veli palatini and levator veli palatini muscles control tube opening through connections to skull base structures that articulate with the upper cervical region. The pharyngobasilar fascia surrounding the tube is continuous with the prevertebral and buccopharyngeal fasciae that connect to the cervical region. The deep cervical musculature including the longus capitis, longus colli, and suboccipital muscles has anatomical relationships with the pharyngeal mechanical environment. The myodural bridge documented by Hack 1995 demonstrates the principle of direct connective tissue continuity between cervical structures and deeper anatomical regions.
For patients with persistent Eustachian tube dysfunction not responding to standard medical management, with concurrent cervical symptoms, with trauma history, or with broader head and neck dysfunction patterns, upper cervical evaluation may be worth considering as one component of comprehensive care alongside continued standard ETD treatment. The evaluation should be pursued with realistic expectations and with continued otolaryngology follow-up as primary medical care. The anatomical relationships supporting this consideration are well-established; the clinical evidence supporting upper cervical care specifically for ETD is reasoning-based rather than trial-based, and patient decisions should reflect this evidence landscape.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Schilder, A. G., Bhutta, M. F., Butler, C. C., et al. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Mitchell-Innes, A., Saunders, T., & Irving, R. (2018). The pathophysiology of Eustachian tube dysfunction and modern management approaches. Journal of Laryngology and Otology, 132(5), 380–384.
Poe, D. S., & Hanna, B. M. (2007). Balloon dilation of the cartilaginous portion of the Eustachian tube: Initial safety and feasibility analysis in a cadaver model. American Journal of Otolaryngology, 28(5), 320–322.
Ward, B. K., Ashry, Y., & Poe, D. S. (2017). Patulous Eustachian tube dysfunction: Patient demographics and comorbidities. Otology & Neurotology, 38(9), 1362–1369.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with Eustachian tube dysfunction should pursue appropriate medical evaluation including otolaryngology consultation and engage with evidence-based medical management as the primary approach. Standard ETD treatments should remain the foundation of care. Upper cervical evaluation should be considered only for specific patient subsets as a complementary approach rather than a primary treatment. No claim is made or implied that upper cervical chiropractic cures or treats Eustachian tube dysfunction or any other specific disease.



Leave a comment