
"Why some cases of “BPPV” are really coming from the neck — and how upper cervical chiropractic care can change the picture"
If you have been told you have BPPV, gone through one or more Epley maneuvers, and the dizziness keeps coming back — you are not imagining things, and you are not alone. The Epley maneuver, when it is the right tool for the job, has a published success rate well into the 90 percent range. So when it does not work, the most useful question is not “why did the maneuver fail?” but “was this really BPPV in the first place?”
Schedule Your Appointment
Schedule appointmentFor a meaningful number of patients, the answer is no. The dizziness is real. The positional trigger is real. But the source is not loose crystals in the inner ear. It is the joints at the top of the neck.
Why Epley Fails: Misdiagnosis Is More Common Than Most People Think
Vestibular specialists openly acknowledge this. The success rate of canalith repositioning for true posterior canal BPPV is so high that when the maneuver does not work, the most likely explanation is that the diagnosis was wrong — not that the technique missed the crystals. That is a quiet truth in the vestibular world that does not always get communicated to patients sitting in the office wondering why they still feel awful.
There are several conditions that can mimic BPPV — vestibular migraine, Menière’s disease, vestibular neuritis, persistent postural-perceptual dizziness (PPPD), and others. But one of the most overlooked is cervicogenic dizziness, which originates in the upper neck. And here is where the diagnosis really gets blurry.
The Diagnostic Trap: Why BPPV Testing Can Light Up a Neck Problem
The Dix-Hallpike test is the standard provocative maneuver used to diagnose BPPV. The patient is moved into a specific position with the head turned and tilted, and the clinician looks for nystagmus and reproduction of dizziness. When the test is positive, the working diagnosis is BPPV.
Here is the problem the published literature has been pointing out for years: the Dix-Hallpike, and most other positional tests, simultaneously stimulate the inner ear and the mechanoreceptors in the upper neck. There is no clean way to fire the vestibular apparatus without also firing the cervical proprioceptors at the same time. So if a patient has a real upper cervical problem, the test position can produce dizziness, mimic crystal-related symptoms, and look like a positive BPPV finding — even when the actual source of the signal is the neck.
This is why the Epley fails. The maneuver is repositioning crystals that may not be the issue. The dizziness keeps coming back because the actual driver — the upper cervical joint — has never been addressed.
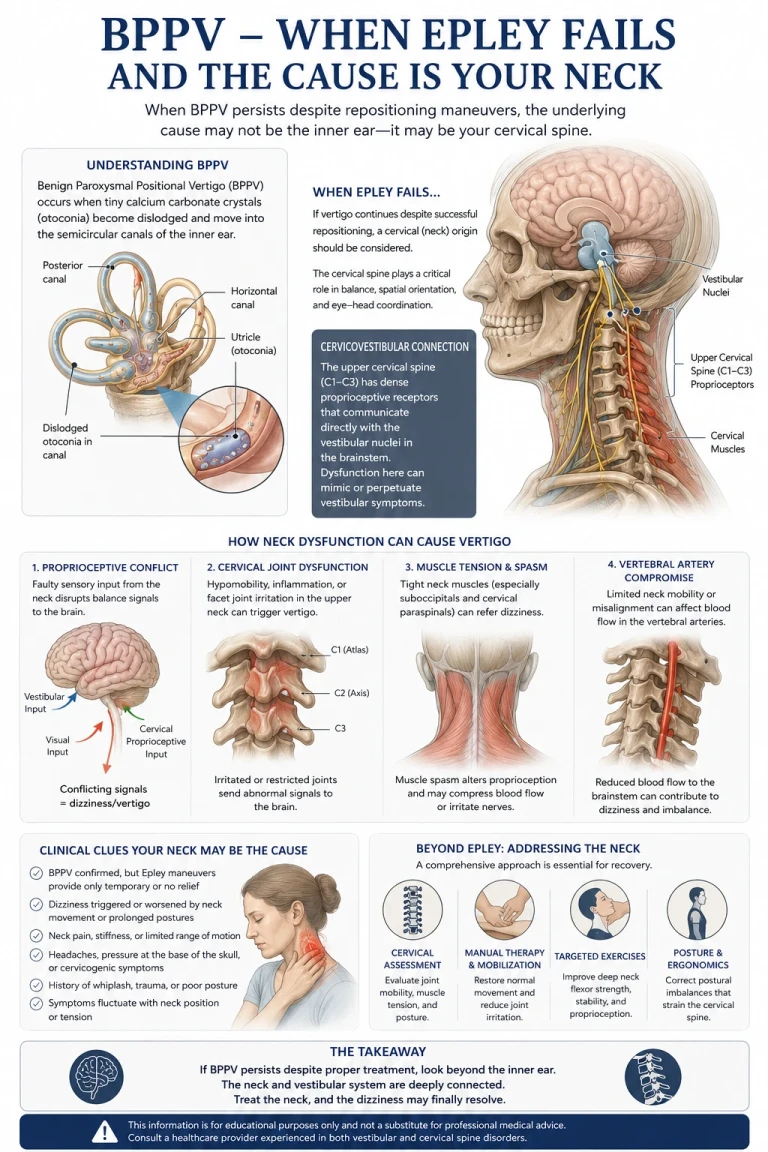
How the Upper Cervical Spine Drives Dizziness
The upper cervical spine — the atlas (C1) and axis (C2) — contains the highest density of mechanoreceptors anywhere in the spinal column. These receptors continuously feed information about head position and movement up into the brainstem, where it converges with input from the inner ear and the eyes inside the vestibular nuclei. The brain uses all three streams together to figure out where you are in space and to keep your balance.
When the upper cervical joints are misaligned or restricted, the proprioceptive signal coming up to the vestibular nuclei becomes distorted. The inner ear may be saying one thing. The eyes may be saying something consistent. But the neck is sending a third, conflicting message. That sensory mismatch is what the brain experiences as dizziness, unsteadiness, or true vertigo — and it can be triggered or worsened by certain head and neck positions, exactly like BPPV.
Specific neck movements can fire these aberrant pathways. Looking up. Turning quickly to one side. Lying down with the head turned. The same positions that show up in BPPV testing are the positions most likely to provoke a cervicogenic dizziness episode. To the patient — and sometimes to the clinician — it looks identical. The difference is where the bad signal is coming from.
CBCT Imaging: Seeing What Is Actually Going On
Related article
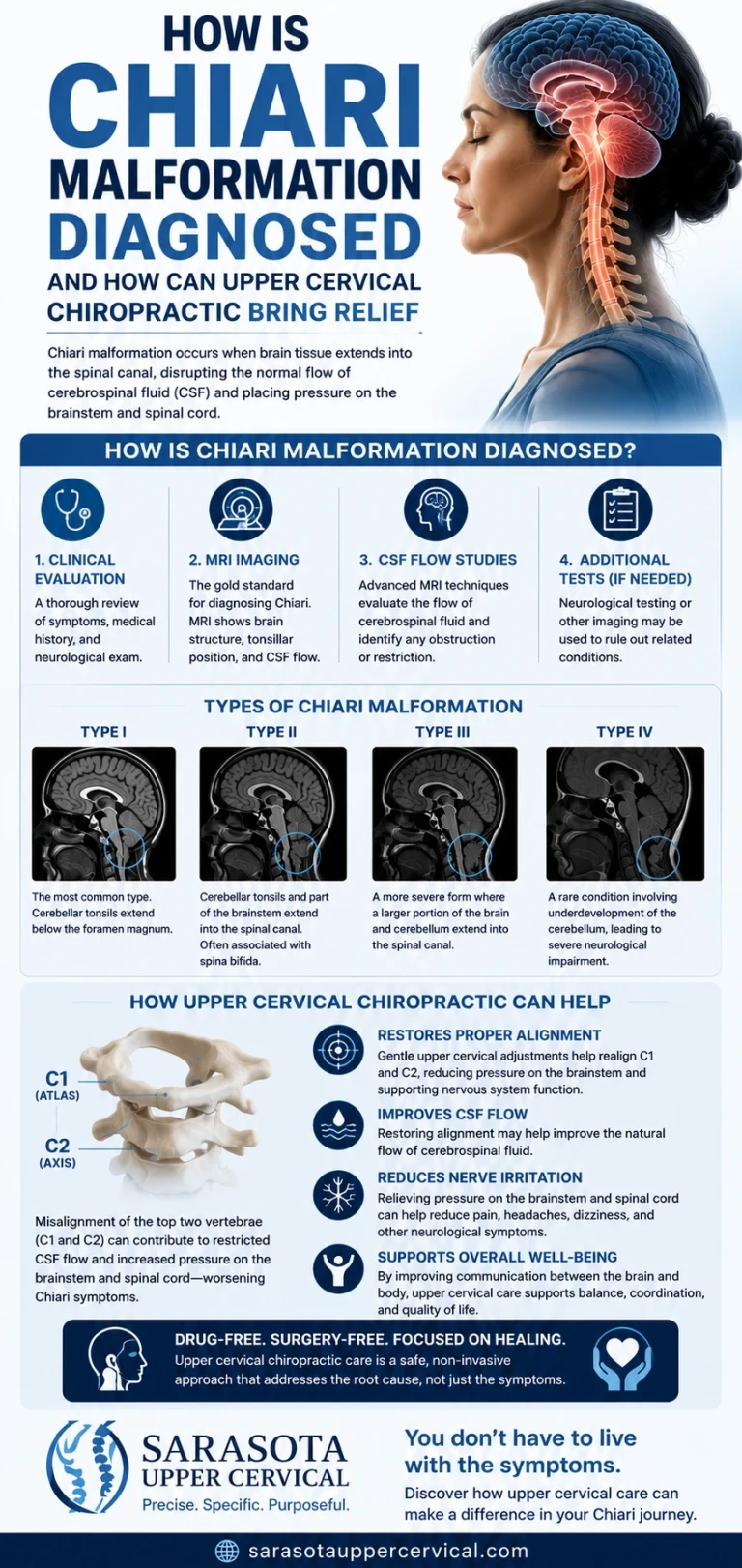
How is chiari malformation diagnosed and how can upper cervical chiropractic bring relief
Jul 12, 2026
Before any care begins in our office, we use Cone Beam Computed Tomography (CBCT) imaging of the upper cervical spine. CBCT is a precision imaging tool that produces three-dimensional views of the atlas, the axis, and the surrounding structures — detail that flat two-dimensional X-rays simply cannot show.
We use these images to measure. Every spine is built differently — the angles, the orientations, and the relationships between the skull, C1, and C2 are unique to each person. Without precise measurements, an upper cervical correction is a guess. With them, the correction can be specific, gentle, and matched to your exact anatomy.
For someone whose dizziness has been blamed on crystals for months or years, this is often the first time the actual driver is being looked at directly. Patients regularly tell us they had MRIs, ENG studies, and ENT workups — all focused on the inner ear, none focused on the structure at the top of the neck where the mechanoreceptor input is generated.
No Twisting. No Cracking. No Pulling of the Neck
When most people think of a chiropractic adjustment, they picture a fast head-turn and a popping sound. That is not what we do. The correction we deliver is specific, low-force, and based directly on the measurements taken from your CBCT scan. There is no twisting of the head. No cranking. No pulling. No cavitation noise.
You lie on your side with your head supported. The contact is light. The correction takes seconds. People who have been dealing with dizziness for a long time are understandably wary of anyone moving their head, and that wariness is appropriate — a forceful neck manipulation in someone whose vestibular system is already irritated is the last thing they need. Our approach is built specifically to avoid that.
Gentle does not mean ineffective. Gentle means we are working with the nervous system rather than against it. The goal is to restore clean input from the upper cervical joints into the brainstem so the vestibular nuclei can process information without the conflicting signal that has been driving the dizziness.
Who This Tends to Help

The patient we see most often in this category has a similar story. Sudden onset of dizziness, sometimes after a fall, a car accident, a dental procedure, or even something as simple as a long flight. A diagnosis of BPPV. One, two, or three Epley maneuvers. Some short-term improvement followed by relapse. Sometimes a referral to vestibular therapy. Sometimes medication. And a slow, growing suspicion that whatever is going on, it is not really being addressed.
Common features include dizziness that comes and goes with neck position, a sense of unsteadiness or imbalance rather than a pure spinning sensation, neck stiffness or pain that the patient may not have connected to the dizziness, and symptoms that get worse with stress, fatigue, or prolonged screen time. None of those features are diagnostic on their own — but together, they raise the question of whether the upper cervical spine deserves a closer look.
What a Realistic First Visit Looks Like
A first visit in our office is a conversation, an examination, and CBCT imaging of the upper cervical spine. We want to understand your full history — every diagnosis, every maneuver, every medication, every theory. We examine the upper cervical spine specifically. We image it. Then we sit down with you and walk through what we found.
If the upper cervical spine looks like a likely contributor to your dizziness, we will tell you that, explain what we would do, and build a plan with you. If it does not, we will tell you that too, and point you toward what is more likely to help. Honesty about fit is part of the job.
If You’re Still Dizzy After Epley, You Have Options
Persistent dizziness is exhausting. It affects how you drive, how you work, how you sleep, and how confident you feel doing simple things like turning your head in the shower. After multiple failed maneuvers, it is normal to start wondering whether anyone really knows what is going on or whether you are just going to live with this.
The next step is not necessarily another Epley. It may be a fundamentally different conversation about whether crystals were ever the right answer in the first place. Upper cervical chiropractic care, delivered with precision imaging and a gentle, non-twisting correction, addresses the structural and neurological side of dizziness that the standard BPPV pathway is simply not designed to look at.
Ready to find out if your dizziness is coming from your neck? Schedule a consultation at our Sarasota office to start with a complete upper cervical evaluation and CBCT imaging.
Disclaimer: Upper cervical chiropractic corrects structural misalignments in the neck which lead to better function. The adjustment doe not treat an condition but it does allow the body to funtion better and gives it the best chance to heal.



Leave a comment