
"Why your ear symptoms change with sleep position, screen use, and head angle — and what this can tell you about the underlying structural factors in your condition"
Patients with Eustachian tube dysfunction often notice patterns in their symptoms that are easy to dismiss but that actually reveal something important about the underlying problem. Symptoms worsen when sitting at a computer for long stretches. They improve after lying down for a while. They flare during reading sessions. They are particularly noticeable in the morning after sleeping in a specific position. They get worse during long drives. These patterns are not random. They reflect the real mechanical and physiological relationship between head and neck position and the function of the Eustachian tube.
Schedule Your Appointment
Schedule appointmentUnderstanding why postures and head positions affect Eustachian tube function is useful in three ways. It helps patients recognize the positions that worsen their symptoms so they can make practical adjustments. It helps distinguish ETD from other ear conditions that do not have the same positional patterns. And it suggests that for patients with strong positional patterns in their ETD, the underlying structural environment of the head and neck region may be contributing to their condition in ways that go beyond the standard inflammatory and anatomical explanations.
This article walks through the specific ways head position and posture affect Eustachian tube function, the daily activities that most commonly worsen ETD symptoms, the postures that can provide temporary relief, and what strong positional patterns in your symptoms can tell you about whether structural cervical factors deserve consideration in your workup.
Why Head Position Affects Eustachian Tube Function
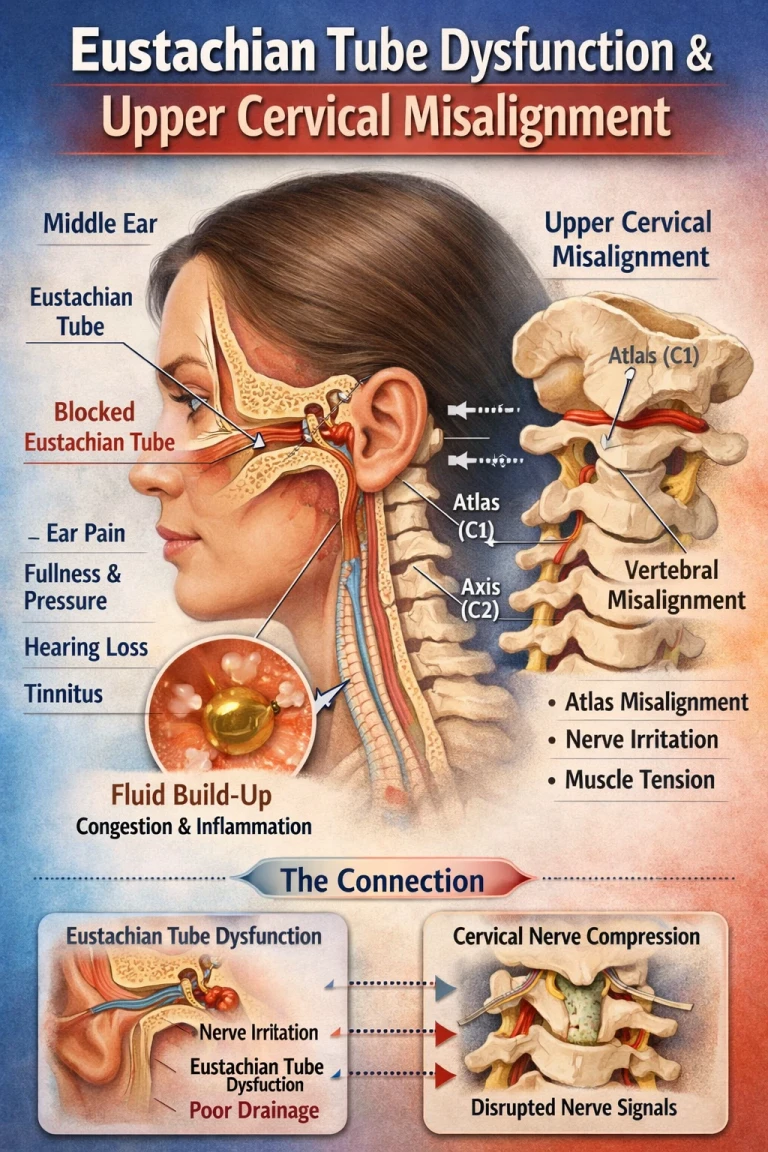
The Eustachian tube is not a passive pipe. It is an active, dynamic structure surrounded by muscles, soft tissues, vascular elements, and connective tissue, all of which are sensitive to position and gravity. Multiple distinct mechanisms link head position to tube function.
Gravity effects on surrounding tissues
The tissues surrounding the Eustachian tube — fat pads, vascular structures, lymphatic tissue, mucous membranes — are subject to gravitational effects that change with body and head position. When the head is upright and erect, these tissues sit in their typical configuration. When the head is tilted forward (looking at a phone or computer), tilted back, or held in sustained side-bent positions, the surrounding tissues shift, the vascular drainage patterns change, and the mechanical environment of the tube changes accordingly.
Vascular and lymphatic drainage
The head, particularly the upper face and sinonasal region, depends on functional vascular and lymphatic drainage that is sensitive to position. Sustained head-down positions or positions that compress the upper cervical region can impair drainage, producing tissue congestion that affects the mucosal environment around the Eustachian tube opening. Patients who notice their ear symptoms are worse in the morning often have this pattern — overnight position has produced some degree of upper airway congestion that affects tube function.
Cervical muscle tension effects
The muscles of the upper neck, particularly the deep suboccipital muscles, are intimately connected to the broader cervicocranial musculature, including the muscles that control the Eustachian tube. The tensor veli palatini and levator veli palatini muscles do not work in isolation — their function is influenced by the broader pattern of head and neck muscle activity. Sustained postures that produce upper cervical muscle tension can affect, through these neuromuscular linkages, the tone and function of the tube-controlling muscles.
Direct effects on upper cervical structure
Sustained head positions place specific loads on the upper cervical joints. Forward head posture loads the atlas-axis joints in a particular way. Head-tilted-to-one-side positions load them differently. Head-back positions create yet another loading pattern. When the upper cervical structure is already compromised by misalignment or prior injury, these loading patterns can produce changes in cervical structural relationships that affect the broader neural and vascular environment of the head — including the environment around the Eustachian tube.
Autonomic effects on mucosal function
The mucosa lining the upper airways, including the area around the Eustachian tube opening, is under continuous autonomic regulation. Sympathetic and parasympathetic input controls blood flow, secretion, and inflammatory tone in these tissues. Sustained postures that affect the cervical sympathetic chain or that alter autonomic balance can influence the mucosal environment around the tube, affecting its function.
Specific Postures and Activities That Commonly Affect ETD
Several common daily postures and activities frequently worsen Eustachian tube dysfunction symptoms. Recognizing these can help patients understand their patterns and make practical adjustments.
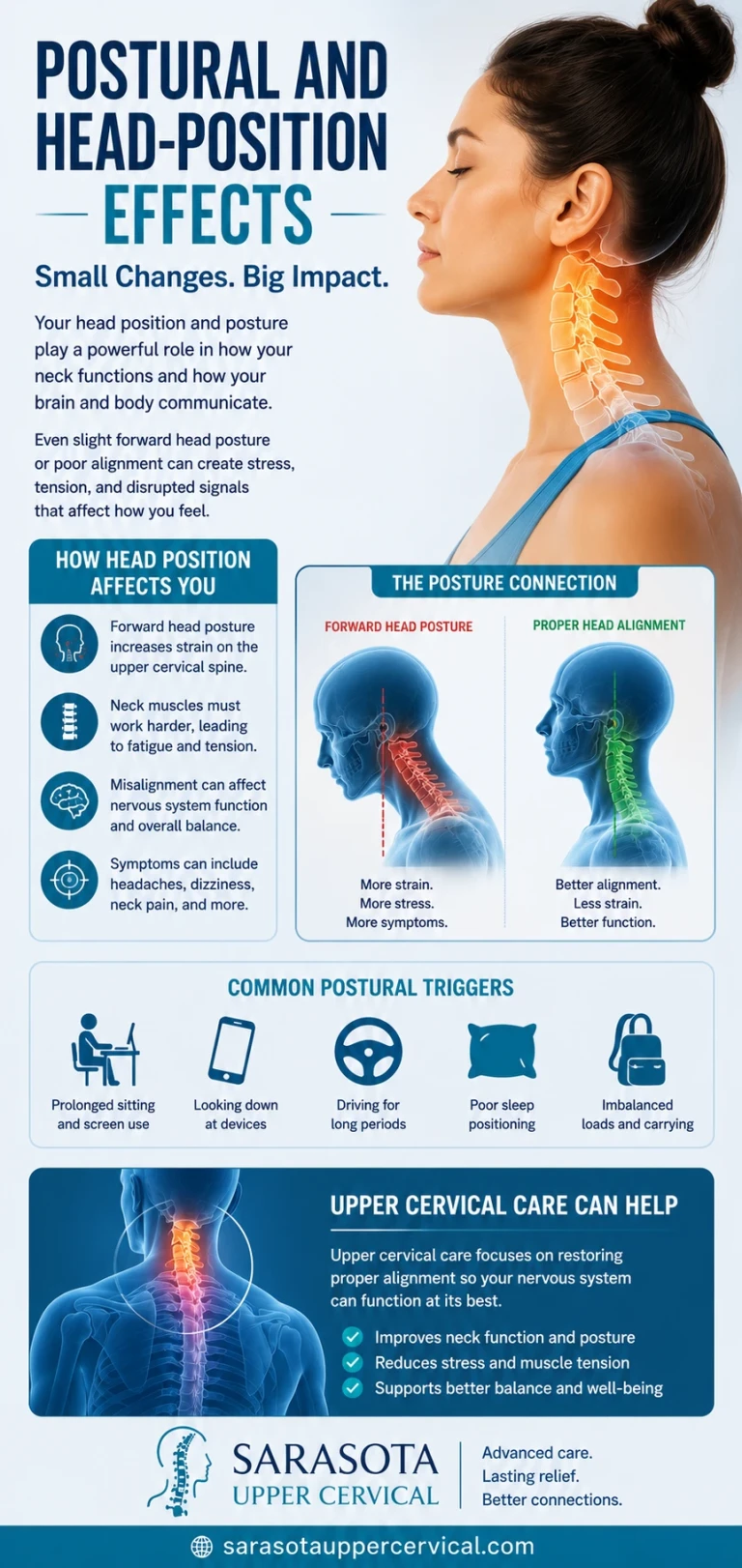
Prolonged screen use and forward head posture
Sustained forward head posture — the position assumed during prolonged computer use, phone use, reading, or any activity that pulls the head forward of the shoulders — affects ETD in multiple ways. The upper cervical muscles work continuously to support the forward-displaced head, producing tension that can affect the broader cervicocranial neuromuscular system. The position can affect vascular and lymphatic drainage. And the sustained load on the upper cervical joints creates the loading pattern that produces the most common type of cervical structural problem. Many patients with chronic ETD describe symptom worsening during or after extended computer or phone use.
Sleep position
Sleep position affects ETD in ways that produce morning symptoms in many patients. Sleeping on one side consistently can produce asymmetric morning ear symptoms reflecting the night-long compression of one side. Sleeping with the head positioned at an awkward angle on inadequate pillows produces sustained upper cervical loading that may affect morning symptoms. Stomach sleeping with the head turned to one side for hours places extreme rotational stress on the upper cervical structures. Patients with morning ear symptoms or symptoms that vary with which side they slept on should consider sleep position as a contributing factor.
Reading position
Reading typically involves a sustained forward-down head position that loads the upper cervical region heavily. Reading in bed with the head propped up against pillows produces a particularly demanding loading pattern. Patients who notice ear symptom worsening during or after extended reading sessions are demonstrating the relationship between cervical loading and tube function.
Driving
Driving involves sustained head position, often with subtle forward head posture and the cervical muscles working to maintain visual orientation across hours of static positioning. Long drives commonly worsen ETD symptoms. The effect is particularly noticeable in patients with otherwise mild ETD whose conditions tolerate routine activities but flare with the sustained postural demands of driving.
Bending forward repeatedly
Activities that involve repeated forward bending — gardening, certain exercise routines, picking up items from the floor — produce repeated changes in head position that can affect Eustachian tube function. For patients with patulous ETD, the head-down position often paradoxically improves symptoms temporarily. For patients with obstructive ETD or baro-challenge-induced ETD, the same position can worsen the picture.
Sustained head-back positions
Activities involving sustained head-back posture — looking up at presentations or screens, certain athletic positions, dental procedures, lying back in barber chairs — load the upper cervical region in a different way than forward head posture and can worsen symptoms for some patients. The effect varies by individual ETD pattern.
Asymmetric postures
Activities that involve sustained asymmetric head positions — holding a phone between ear and shoulder, sleeping on one side consistently, working at a poorly arranged computer setup that requires constant head turning — produce sustained asymmetric upper cervical loading. The asymmetry often correlates with which ear is more symptomatic in patients with unilateral ETD.
Positions That Can Provide Temporary Relief
Just as some positions worsen ETD symptoms, others can provide temporary relief. Recognizing these can help patients manage their symptoms and can also help confirm the diagnosis and characterize the subtype.
Lying flat
Lying horizontal often improves Eustachian tube symptoms by removing the gravitational load that pulls tissues away from the tube opening. Many patients notice their symptoms improve within 15 to 30 minutes of lying down. This relief is one of the reasons rest helps, beyond just the general relaxation effect.
Head-down or head-tilted-forward positioning (patulous ETD)
Patients with patulous ETD specifically often experience symptom relief with head-down positioning — bending forward, lying with the head below the heart, or specific yoga positions that put the head in a dependent position. The mechanism involves increased blood flow and tissue engorgement that helps close the abnormally open tube. This positional improvement is one of the most distinguishing features of patulous ETD.
Neutral upright posture
Maintaining the head balanced over the shoulders — neutral upright posture without forward head positioning — is the position that places the least sustained load on the upper cervical structures and surrounding tissues. For patients with chronic ETD, sustained neutral posture during desk work, driving, and other prolonged activities reduces the cumulative postural load on the system.
Side-lying with the affected ear up
For patients with unilateral ETD, lying on the unaffected side (with the affected ear up) can produce gravity-assisted drainage of the affected middle ear and provide symptom relief. This position is sometimes recommended for relief during acute flares.
What Strong Positional Patterns Tell You About Your Condition
The presence and strength of positional patterns in your ETD symptoms provide useful diagnostic information that often gets overlooked.
Strong positional patterns suggest a meaningful structural component
Patients whose ETD symptoms reliably worsen with specific positions, improve with others, and vary substantially with daily postural patterns are demonstrating that the structural environment of their head and neck is contributing to their condition. The tube itself does not change with position — the surrounding environment does. Strong positional symptom patterns indicate that the environment is what is driving the dysfunction, which means addressing the structural environment may produce meaningful improvement.
Weak or absent positional patterns suggest the cause lies elsewhere
Patients whose ETD symptoms are essentially constant regardless of position, or whose symptoms relate primarily to specific triggers (a recent cold, a recent flight, recent weight loss) rather than to ongoing postural patterns, are demonstrating that something other than the surrounding structural environment is the primary driver. For these patients, addressing the specific underlying trigger — treating the upper respiratory infection, managing the weight stability, addressing the inflammation — is likely more important than structural cervical evaluation.
Asymmetric symptoms with asymmetric postures
When ETD symptoms are unilateral and correlate with chronic asymmetric postures — symptoms worse on the side the patient sleeps on, on the side where they hold their phone, on the side affected by their work setup — the structural relationship between posture and tube function is being clearly demonstrated. The asymmetry can also suggest an asymmetric upper cervical structural problem that contributes to the asymmetric symptom picture.
Position-related symptoms that persist after addressing other factors
If standard ETD treatment has addressed inflammatory factors, hydration, weight management, and other identified contributors but positional symptoms persist, the structural environment is likely contributing to the residual dysfunction. This subset of patients often responds to structural intervention that the other treatments did not provide.
Where Upper Cervical Structure Fits Into the Postural Picture
The connection between postural patterns and Eustachian tube function ultimately runs through the upper cervical structure. The upper cervical region — the joints between the skull, atlas, and axis — is the link between posture and the broader head and neck environment that affects tube function.
How postures affect upper cervical structure
Sustained head positions place specific loads on the upper cervical joints, with forward head posture being the most common and most clinically significant. Over time, sustained loading patterns can produce upper cervical structural changes — misalignment, restricted motion, altered joint relationships — that persist even when the patient is not actively in the loading posture. The structural changes then influence the surrounding tissues, vascular drainage, autonomic regulation, and mucosal environment that affect Eustachian tube function.
When postural correction alone is insufficient
Patients whose ETD has a postural component sometimes try to address it through postural correction alone — ergonomic improvements, posture awareness, exercises, physical therapy approaches. These interventions can be helpful and are often appropriate first steps. But for patients whose sustained postures have already produced upper cervical structural changes, postural correction alone may be insufficient. The structural changes persist regardless of current posture, and the patient continues to experience the downstream effects of those changes on tube function and other symptoms. For these patients, addressing the structural component specifically may be necessary to fully resolve the postural-influenced symptoms.
When postural patterns indicate cervical evaluation
Strong positional symptoms, asymmetric symptoms correlating with asymmetric postures, persistent positional symptoms despite postural improvement, and associated cervical symptoms (neck pain, suboccipital tension, cervicogenic headache) together suggest that the upper cervical structural environment deserves evaluation. The patient may have a structural component that is amplifying the postural effects on tube function, and addressing it can produce improvement beyond what postural correction alone provides.

How an Upper Cervical Evaluation Works
Upper cervical chiropractic is a specialty within the broader chiropractic profession that focuses specifically on the precise structural relationship between the skull, atlas, and axis. For patients with positional ETD patterns suggesting a structural cervical contribution, the evaluation can identify whether meaningful misalignment is present.
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree. The imaging captures the structural relationships that postural patterns can suggest but cannot directly visualize.
Objective testing before any intervention
Leg length analysis measures functional postural asymmetry, and paraspinal infrared thermography measures asymmetric autonomic activity along the cervical spine — directly relevant given the autonomic component of postural ETD. If both tests indicate the spine is in alignment, no adjustment is delivered. If they indicate a structural shift, a precise correction is delivered along the vector calculated from the CBCT.
Precision without manipulation
Corrections are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. The motion is small.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation is worth considering for patients with ETD when any of the following are true:
Your ETD symptoms vary significantly with head and neck position. Your symptoms reliably worsen with specific postural patterns — screen use, sleep position, reading, driving — and improve in others. You have asymmetric ETD symptoms that correlate with asymmetric postural habits. You have associated cervical symptoms — neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern — alongside the ETD. Your ETD developed after head or neck trauma. Your ETD has not responded fully to standard treatment addressing inflammatory factors, hydration, weight, and other identified contributors. Your positional symptoms have persisted despite engagement with postural correction, ergonomic improvements, or general physical therapy.
For ETD patients without strong positional patterns and with clear non-postural causes — recent illness, identified weight loss, pregnancy, hormonal triggers — the case for upper cervical evaluation is weaker, and standard approaches addressing the identified causes should be the focus.
To schedule an upper cervical evaluation at Sarasota Upper Cervical Chiropractic, call 941-259-1891.
Where to Go From Here
The positional and postural patterns in your ETD symptoms provide useful information about the underlying drivers of your condition. Strong positional patterns suggest that the structural environment of your head and neck is contributing to your symptoms in ways that go beyond the typical inflammatory and anatomical explanations. For many patients, addressing the postural component through ergonomic and behavioral changes provides meaningful improvement. For patients whose positional symptoms persist despite postural correction, or who have associated cervical symptoms alongside their ETD, an upper cervical evaluation can identify whether structural cervical factors deserve attention as part of a more complete approach.
Sarasota Upper Cervical Chiropractic uses three-dimensional CBCT imaging and precision-based correction to address structural problems in the upper cervical region when present. To schedule an evaluation, call 941-259-1891.
References
Schilder, A. G. M., Bhutta, M. F., Butler, C. C., et al. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Bluestone, C. D. (2008). Eustachian tube: Structure, function, role in otitis media. PMPH-USA.
Smith, M. E., & Tysome, J. R. (2015). Tests of Eustachian tube function: A review. Clinical Otolaryngology, 40(4), 300–311.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Tracey, K. J. (2002). The inflammatory reflex. Nature, 420(6917), 853–859.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with persistent Eustachian tube dysfunction should pursue appropriate medical evaluation by an otolaryngologist alongside any structural assessment. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment