
"The ETD subtype that produces problems with flying, diving, and altitude — why it happens, how it's treated, and the structural angle worth considering when the picture has not improved with standard care"
Some patients have ear function that seems essentially normal during everyday life. They breathe normally. They swallow normally. They hear normally. They have no chronic ear pressure or fullness. And yet when these same patients board an airplane, dive beneath the surface of the water, or drive into the mountains, their ears refuse to do what ears are supposed to do. Pressure builds. Pain develops. The familiar swallow-and-pop maneuver fails to relieve the problem. For severe cases, hearing loss, vertigo, or even bleeding into the middle ear can occur from the pressure differential the ear cannot equalize.
Schedule Your Appointment
Schedule appointmentThis is baro-challenge-induced Eustachian tube dysfunction — a recognized form of ETD that becomes apparent only when the ear is challenged with significant pressure changes. The condition was formally identified as a distinct subtype in the 2015 ETD consensus statement (Schilder et al., 2015), and it affects a population that is harder to identify than patients with obvious chronic ear problems. Pilots, flight attendants, scuba divers, frequent flyers, mountain athletes, and military aviators are particularly affected. For many of these patients, baro-challenge-induced ETD is not just a quality-of-life issue but a career-limiting or activity-ending problem.
This article walks through what baro-challenge-induced ETD actually is, the symptoms that define it, the recognized causes, the diagnostic process, the standard treatment options, and the specific subset of patients in whom structural cervical factors may deserve consideration as part of a more complete approach.
What Baro-Challenge-Induced ETD Is
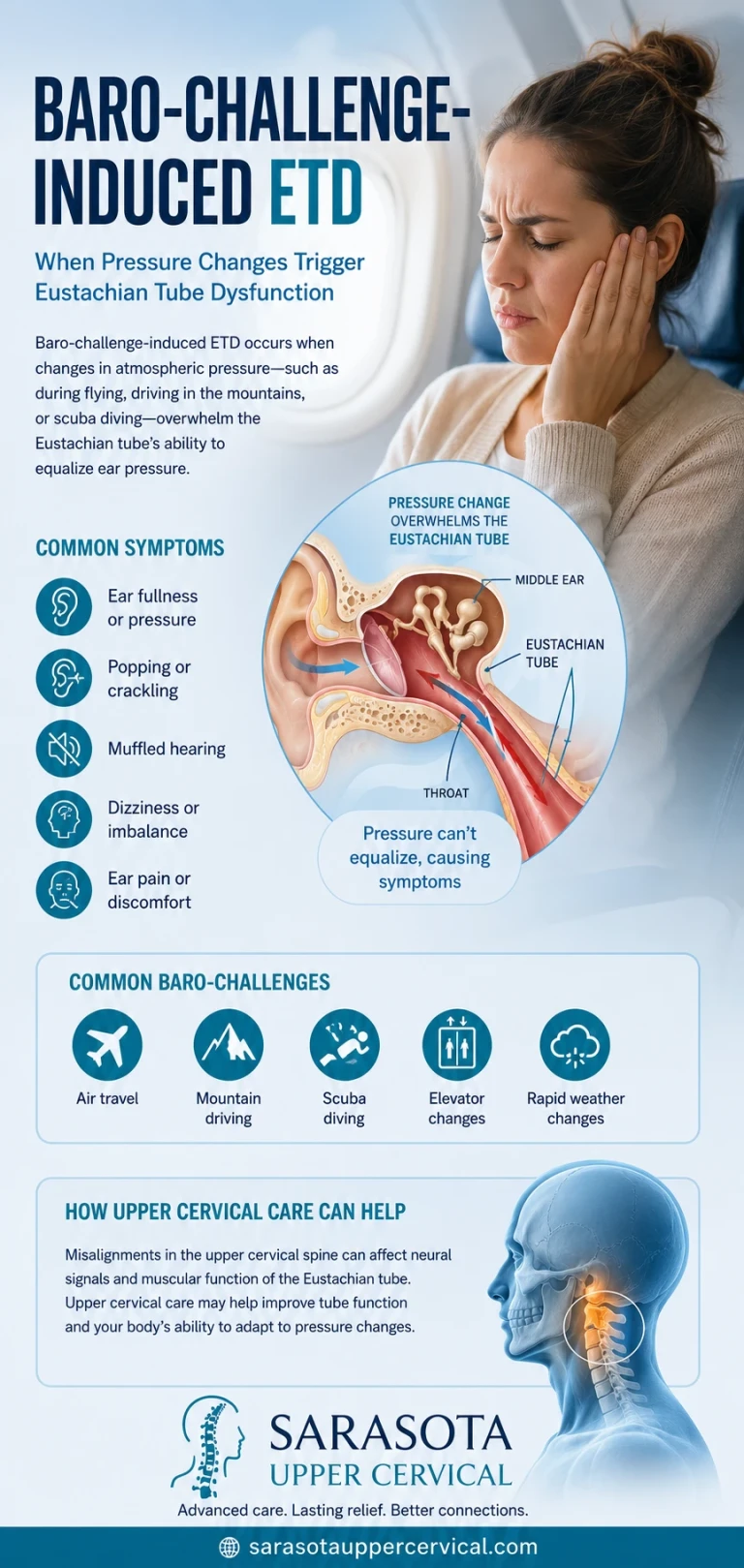
The Eustachian tube is a small canal connecting the middle ear to the back of the throat. Its primary job is pressure equalization — the tube briefly opens during swallowing, yawning, or jaw movement to allow air to move between the middle ear and the outside environment, keeping the pressure on both sides of the eardrum equal. For most of the day, this happens automatically and without any conscious awareness.
Routine pressure equalization works for small, gradual pressure changes. The tube needs to open only briefly, only against modest pressure differentials, and only intermittently. Baro-challenge situations are different. During airplane descent, scuba diving, or rapid altitude change, the external pressure changes substantially and quickly, requiring the Eustachian tube to function actively and repeatedly against large pressure gradients. For a tube that works adequately at rest but is subclinically compromised, the baro-challenge reveals what routine activities did not.
Baro-challenge-induced ETD is essentially a stress test of Eustachian tube function. The tube is doing well enough during routine life — sufficient to prevent chronic symptoms — but not well enough to handle the demands of significant pressure change. The diagnosis is made when the clinical picture matches the pattern: normal function at baseline, characteristic symptoms during or after baro-challenge, and exclusion of other causes.
The Symptoms That Define the Condition
The symptoms of baro-challenge-induced ETD appear during or shortly after exposure to pressure change and often resolve over hours to days after returning to baseline pressure. The pattern of appearing with baro-challenge and resolving afterward is one of the most characteristic features.
Ear pain during pressure change
The signature symptom. Sharp, intense pain in the affected ear during airplane descent (most commonly), during dive descent (for divers), or during rapid altitude change. The pain typically begins gradually, intensifies as pressure differential increases, and reaches peak severity when the patient is unable to equalize. For severe cases, the pain can be incapacitating.
Ear fullness and pressure
A sense of fullness, blockage, or pressure in the affected ear during and after baro-challenge. The sensation often persists for hours after the pressure change has resolved, gradually improving as the ear returns to baseline. Some patients describe the feeling as if the ear is stuffed with cotton.
Hearing loss
Muffled hearing or partial hearing loss during and after baro-challenge. The hearing loss reflects pressure-related changes in the middle ear that affect tympanic membrane mobility. In most cases the hearing returns to normal as the ear equalizes over hours to days, but severe cases can produce more lasting changes.
Tinnitus
Ringing, buzzing, or roaring in the affected ear during or after baro-challenge. The tinnitus typically reflects the abnormal middle ear environment rather than permanent inner ear damage in most cases.
Vertigo or disequilibrium
Some patients experience vertigo, dizziness, or balance disturbance during baro-challenge. This reflects alternobaric vertigo, in which pressure differentials between the two ears produce asymmetric vestibular stimulation. The vertigo is typically brief but can be intense and is a known cause of accidents in divers and pilots.
Failure to clear with standard maneuvers
A defining feature of the condition is the inability to clear the ears with standard equalization techniques — swallowing, yawning, the Valsalva maneuver, the Toynbee maneuver, the Frenzel maneuver. Patients with baro-challenge-induced ETD often know multiple equalization techniques and have tried them repeatedly without success during the affected event.

Severe cases: barotrauma
In severe cases, the pressure differential the tube cannot equalize produces actual tissue damage — middle ear barotrauma, with bleeding into the middle ear, tympanic membrane rupture, or inner ear barotrauma producing permanent hearing loss or vestibular dysfunction. Severe barotrauma is uncommon but represents the worst-case outcome of baro-challenge-induced ETD.
What Causes Baro-Challenge-Induced ETD
Several factors can produce the tube dysfunction that becomes apparent under baro-challenge conditions. Most patients have one or more identifiable contributing factors.
Subclinical inflammation
Low-grade inflammation in the Eustachian tube or surrounding tissues — from chronic allergic rhinitis, low-grade upper respiratory issues, chronic sinusitis, or other inflammatory conditions — can subclinically narrow the tube. The narrowing is insufficient to produce symptoms during routine activities but becomes functionally significant under baro-challenge demands. Patients with seasonal allergies, chronic nasal congestion, or sinus issues are over-represented among baro-challenge-induced ETD patients.
Anatomical factors
Some patients have anatomical variations in the Eustachian tube — narrower than average diameter, more horizontal orientation, or other structural features — that make pressure equalization more difficult. These features are often present from birth and may explain why some patients have had pressure-change problems throughout their lives.
Functional muscle dysfunction
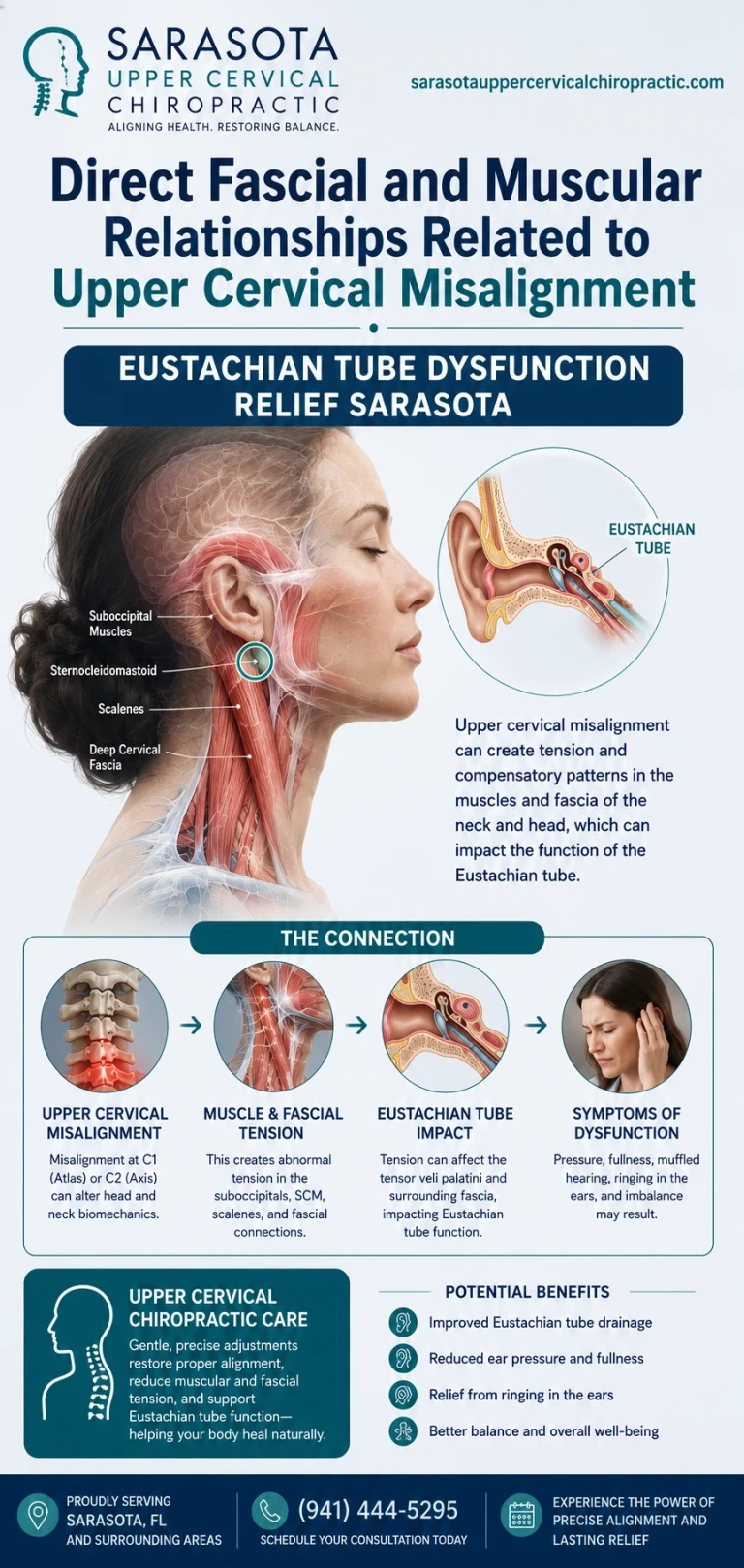
The Eustachian tube is actively opened by the tensor veli palatini and levator veli palatini muscles. Dysfunction in these muscles — through neural control problems, coordination issues, or muscular weakness — can produce inadequate tube opening during baro-challenge. The neural control of these muscles involves cranial nerve V (tensor veli palatini) and the pharyngeal plexus (levator veli palatini), both with brainstem connections.
Prior surgery or scarring
Patients with prior ear surgery, prior nasopharyngeal surgery, or scarring from prior infections can develop baro-challenge-induced ETD even when their routine ear function appears normal. The structural changes from prior interventions affect tube function under stress.
Chronic inflammatory or allergic conditions
Chronic rhinitis, chronic sinusitis, gastroesophageal reflux disease (GERD), and other conditions affecting the upper airways can produce ongoing low-grade inflammation that affects Eustachian tube function. Identifying and treating these underlying conditions is often part of comprehensive baro-challenge-induced ETD management.
Reduced mucociliary function
The Eustachian tube depends on functional mucociliary clearance to maintain its normal environment. Conditions affecting cilia function — including some chronic respiratory conditions, smoking, and various inflammatory states — can compromise tube function under baro-challenge demands.
Post-traumatic onset
Some patients develop baro-challenge-induced ETD after head or neck trauma — whiplash, concussion, sports head injury, or significant falls. For these patients, the trauma may have produced effects on the autonomic regulation of mucosal tissues, on the neural control of tube musculature, or on the broader craniocervical environment in which the upper airway functions. The post-traumatic subset is the population most likely to have a meaningful structural cervical contribution to their condition.
How Baro-Challenge-Induced ETD Is Diagnosed
Baro-challenge-induced ETD is a clinical diagnosis established by history, examination during and between baro-challenge episodes, and exclusion of other causes.
History
The clinical history is typically diagnostic. Symptoms appearing reliably during baro-challenge — flying, diving, altitude change — with relatively normal ear function between exposures suggests the diagnosis. Frequency of exposure, severity of symptoms, ability to clear with various equalization maneuvers, and presence of contributing factors (allergies, sinus issues, GERD, recent illness) are all relevant.
Otoscopic examination
Examination between episodes is often normal or shows only subtle findings. Examination during or shortly after a symptomatic episode may show middle ear effusion, retraction of the tympanic membrane, or in severe cases evidence of barotrauma — bleeding into the middle ear or tympanic membrane perforation.
Tympanometry
Tympanometry between episodes is typically normal. Tympanometry during or after symptomatic episodes may show abnormalities reflecting middle ear effusion or pressure differential.
Eustachian tube function testing
Specialized tests of Eustachian tube function — including the Valsalva test, Toynbee test, and tubomanometry — assess the tube's ability to equalize pressure on demand. Patients with baro-challenge-induced ETD may have normal or only mildly abnormal results on these tests despite their clear clinical history, which is part of why the diagnosis often relies heavily on the symptom pattern.

Evaluation for contributing conditions
Evaluation for the conditions that commonly contribute to baro-challenge-induced ETD — allergic rhinitis, chronic sinusitis, GERD, anatomical variations — is part of comprehensive workup. Identifying and addressing these contributing factors is often the most useful element of treatment.
Imaging
CT or MRI imaging is sometimes obtained to evaluate for structural abnormalities, particularly in patients with severe or treatment-resistant symptoms. Specialized imaging of the Eustachian tube anatomy is occasionally used in academic centers.
Standard Treatment Approaches
Treatment of baro-challenge-induced ETD follows a stepwise approach focused on addressing identifiable contributing factors and improving tube function during baro-challenge situations.
Treatment of underlying conditions
Identifying and treating contributing conditions is the foundation of management. Allergic rhinitis treatment, chronic sinusitis treatment, GERD management, and similar interventions targeting the underlying contributors often produce meaningful improvement in baro-challenge tolerance.
Pre-exposure preparation
Decongestants taken before known baro-challenge events (flights, dives) can temporarily improve tube function. Both oral decongestants (such as pseudoephedrine) and topical decongestant sprays (such as oxymetazoline) have been used. Timing matters — these are typically taken 30 to 60 minutes before anticipated descent or pressure change.
Equalization technique training
For divers and frequent flyers, learning multiple equalization techniques and practicing them in low-stakes situations improves the patient's ability to clear during demanding situations. Techniques including the Valsalva maneuver, Toynbee maneuver, Frenzel maneuver, and various hands-free techniques can be taught and practiced.
Nasal saline irrigation
Regular nasal saline irrigation can reduce inflammation and improve mucociliary function, potentially improving baseline tube function and baro-challenge tolerance.
Topical steroid sprays
Nasal steroid sprays can reduce inflammation in the nasopharynx and around the Eustachian tube opening, improving function in patients with inflammatory contributors. These typically require sustained use to produce meaningful improvement.
Balloon dilation
Eustachian tube balloon dilation is a relatively newer intervention in which a small balloon is inflated within the tube to address chronic narrowing. The procedure has shown benefit for some patients with chronic ETD and has been investigated for baro-challenge-induced ETD specifically. Balloon dilation is typically reserved for patients who have not responded to conservative management.
Activity modification
For some patients, avoiding the specific baro-challenge that produces symptoms — limiting flying, ceasing diving, avoiding altitude exposure — may be necessary, particularly for those whose work or recreational activities depend on tolerance of these conditions. This is a significant decision with career and quality-of-life implications, and pursuing comprehensive evaluation before accepting activity restriction is appropriate.
Where the Craniocervical Junction Fits Into the Picture
The connection between upper cervical structural problems and baro-challenge-induced ETD is less direct than for some other ear-related conditions. The primary causes of baro-challenge-induced ETD — inflammation, anatomical factors, allergies, prior surgery — are not typically cervical in origin. The cervical contribution becomes relevant for specific patient subsets in which structural factors are plausibly affecting the broader picture.
Neural control of tube musculature
The Eustachian tube is opened by two muscles — the tensor veli palatini and the levator veli palatini. The tensor veli palatini is innervated by the mandibular branch of the trigeminal nerve (cranial nerve V), and the levator veli palatini is innervated by the pharyngeal plexus, which receives contributions from cranial nerve X (vagus) and the cervical sympathetic chain. These cranial nerves emerge from the brainstem, which sits within the bony corridor formed by the skull, atlas (C1), and axis (C2). The cervical sympathetic chain runs along the front of the upper cervical spine.
When the upper cervical structure is significantly misaligned, the mechanical environment of the brainstem and surrounding cranial nerves can be affected. Chronic low-grade irritation and altered autonomic balance can plausibly influence the neural control of the Eustachian tube musculature, contributing to functional dysfunction under stress.
Autonomic regulation of mucosal function
Mucosal tone, secretion, and inflammatory regulation throughout the upper airway depend heavily on autonomic balance. Sympathetic and parasympathetic input regulate blood flow, glandular secretion, and inflammatory responses in nasal, sinus, and Eustachian tube tissues. Chronic autonomic dysregulation — including dysregulation produced by craniocervical structural problems — can contribute to the chronic low-grade inflammation that underlies baro-challenge-induced ETD in many patients.
The post-traumatic subset
Patients whose baro-challenge-induced ETD began after head or neck trauma represent the subset for whom the cervical connection is most plausible. The trauma that triggered the ear symptoms also produced upper cervical structural injury, and the broader picture often includes other symptoms — neck pain, suboccipital tension, possible vestibular involvement, autonomic dysregulation — suggesting the cervical contribution extends beyond just the ear symptoms.
Honest framing of the evidence
Direct research connecting upper cervical chiropractic to baro-challenge-induced ETD outcomes is limited. The framework rests on anatomical relationships and clinical observation rather than on randomized controlled trial evidence. Patients considering upper cervical evaluation for baro-challenge-induced ETD should understand that this represents a hypothesis-driven consideration for specific patient subsets, not an established treatment supported by formal clinical research. For most patients, addressing identified contributing factors — inflammation, allergies, sinus issues, GERD — and standard pre-exposure preparation should be the primary approach. Structural cervical evaluation is appropriate for the subset with trauma history, associated cervical symptoms, or incomplete response to standard management.
How Upper Cervical Care Addresses the Structural Component
Upper cervical chiropractic is a specialty within the broader chiropractic profession that focuses specifically on the precise structural relationship between the skull, atlas, and axis. For patients with baro-challenge-induced ETD in whom a structural cervical contribution is suspected, the evaluation can identify whether meaningful misalignment is present.
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree — precision that standard X-rays cannot match. The imaging allows the practitioner to determine whether a meaningful structural component is present and exactly what its direction and magnitude are.
Objective testing before any intervention
Two objective tests are performed at every visit. Leg length analysis measures functional postural asymmetry that reflects upper cervical misalignment. Paraspinal infrared thermography measures asymmetric autonomic activity along the cervical spine. If both tests indicate the spine is in alignment, no adjustment is delivered. If they indicate a shift, a precise correction is delivered along the vector calculated from the CBCT analysis.
Precision without manipulation
When corrections are indicated, they are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. For patients with ear and pressure-related symptoms — whose systems may be sensitized — this precision matters.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation is worth considering for patients with baro-challenge-induced ETD when any of the following are true:
Your symptoms began after head or neck trauma — whiplash, concussion, sports head injury, significant fall — and have persisted since. You have associated cervical symptoms — chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache pattern — alongside the ear symptoms. Your symptoms include features beyond baro-challenge-induced ETD alone — vestibular symptoms, autonomic dysregulation, chronic upper airway issues — suggesting broader involvement. Standard treatments — addressing inflammatory contributors, pre-exposure preparation, equalization techniques — have not adequately improved your baro-challenge tolerance. You have a history of multiple concussions or significant neck injuries layered on top of the current symptoms. You are pursuing comprehensive evaluation, particularly if your activities (professional flying, diving, or similar) make baro-challenge tolerance career-critical.
For baro-challenge-induced ETD patients without these features — particularly those with clear allergic, inflammatory, or anatomical contributors that respond to standard management — the case for upper cervical evaluation is weaker, and standard approaches addressing the identified causes should remain the focus.
To schedule an upper cervical evaluation at Sarasota Upper Cervical Chiropractic, call 941-259-1891.
Where to Go From Here
Baro-challenge-induced ETD is a recognized form of Eustachian tube dysfunction that becomes apparent only when the ear is challenged with significant pressure change. For most patients, standard care addressing identifiable contributing factors — inflammation, allergies, sinus issues, GERD — combined with pre-exposure preparation and equalization technique training produces meaningful improvement. For the subset of patients whose condition began after trauma, who have associated cervical symptoms, or whose symptoms have not responded adequately to standard management, the upper cervical spine deserves consideration as part of a more complete evaluation.
Sarasota Upper Cervical Chiropractic uses three-dimensional CBCT imaging and precision-based correction to address structural problems in the upper cervical region when present. To schedule an evaluation, call 941-259-1891.
References
Schilder, A. G. M., Bhutta, M. F., Butler, C. C., et al. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Bluestone, C. D. (2008). Eustachian tube: Structure, function, role in otitis media. PMPH-USA.
Smith, M. E., & Tysome, J. R. (2015). Tests of Eustachian tube function: A review. Clinical Otolaryngology, 40(4), 300–311.
Mitchell-Innes, A., Williams, J., Pothier, D., et al. (2018). Balloon Eustachian tuboplasty for chronic Eustachian tube dysfunction: Systematic review and meta-analysis. Otology & Neurotology, 39(6), 651–659.
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Tracey, K. J. (2002). The inflammatory reflex. Nature, 420(6917), 853–859.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with suspected baro-challenge-induced Eustachian tube dysfunction should pursue appropriate medical evaluation by an otolaryngologist, particularly when symptoms are severe or affect activities critical to work or recreation. Patients whose activities involve diving, professional flying, or significant altitude exposure should have appropriate medical clearance before continuing these activities if ETD is suspected. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment