
"Patients with epilepsy frequently have multiple coexisting conditions including chronic headaches, neck pain, post-traumatic features, and sleep disturbance. Understanding the broader clinical picture helps Sarasota patients pursue comprehensive care alongside their essential neurological management"
Living with epilepsy involves more than managing seizures. Patients with epilepsy frequently experience a range of coexisting conditions that substantially affect their quality of life — chronic headaches and migraines occur at higher rates than in the general population, neck pain and musculoskeletal issues are common, post-traumatic features may persist when the epilepsy developed after head or neck trauma, sleep disturbance affects both seizure control and overall function, and the medications used to manage seizures can produce their own side effects. Comprehensive care for epilepsy patients addresses not just the seizure disorder itself but the broader clinical picture that affects daily life.
Schedule Your Appointment
Schedule appointmentAt Sarasota Upper Cervical, we see patients with epilepsy who come to us not seeking treatment for their seizure disorder — which appropriately remains under neurological management — but for the headaches, neck pain, and other coexisting conditions that upper cervical chiropractic can legitimately address. Many of these patients report that as their headaches improve, their neck pain resolves, their sleep quality improves, and their overall wellness increases, their general sense of wellbeing also improves. Some patients also report changes in their seizure patterns alongside these broader improvements, though attributing such changes specifically to upper cervical care requires careful interpretation given the multiple factors at play and the absence of randomized controlled trial evidence for chiropractic care as epilepsy treatment.
This article is for patients with epilepsy in Sarasota and surrounding communities who are dealing with multiple coexisting conditions and considering whether comprehensive care including upper cervical chiropractic evaluation may be appropriate for their situation. The article walks through the common coexisting conditions epilepsy patients face, why these conditions develop, what upper cervical care can and cannot address, the essential role of continued neurological management, important safety considerations specific to epilepsy patients, and how comprehensive care fits together. Throughout, the article maintains an honest framing — upper cervical chiropractic is not treatment for epilepsy itself, but addressing the multiple coexisting conditions epilepsy patients face can substantially improve quality of life.
An Important Framing Note
Before discussing what upper cervical care may offer epilepsy patients, we want to be explicit about what this article does and does not claim.
Upper cervical chiropractic is not a treatment for epilepsy. It is not an alternative to anti-epileptic medications. It is not a primary intervention for seizure disorders. No randomized controlled trials demonstrate that upper cervical chiropractic treats epilepsy, reduces seizure frequency as a specific intervention, or substitutes for neurological management. Patients with epilepsy must continue their anti-epileptic medications and neurological follow-up regardless of any complementary care they pursue. Reducing or discontinuing anti-epileptic medications without neurological supervision can produce breakthrough seizures with potentially severe consequences including injury, status epilepticus, or death.
What upper cervical chiropractic can legitimately address are the multiple coexisting conditions that epilepsy patients commonly have — chronic headaches, neck pain, post-traumatic features, and broader wellness factors. The clinical observations we make in our practice — that epilepsy patients often feel better overall with comprehensive care — reflect improvements in these coexisting conditions and overall wellness, not direct treatment of the seizure disorder itself. This honest framing protects patients and provides realistic expectations about what comprehensive care can offer.
The Coexisting Conditions Epilepsy Patients Commonly Have
Patients with epilepsy frequently have multiple coexisting conditions that affect their quality of life. Understanding these conditions clarifies what comprehensive care addresses.
Headaches and migraine
Headaches occur at substantially higher rates in patients with epilepsy than in the general population. The 2011 review by Bigal and colleagues in Current Opinion in Neurology documented the substantial comorbidity between epilepsy and migraine (Bigal et al., 2011). Migraine and epilepsy share underlying mechanisms involving cortical hyperexcitability, neurotransmitter dysregulation, and central sensitization. Many epilepsy patients have migraine alongside their seizure disorder. Many also have cervicogenic headache or tension-type headache contributing to their overall headache burden. The headaches can be disabling in their own right, and the medications used to treat both conditions can interact, complicating overall management.
Neck pain and musculoskeletal issues
Neck pain is common in epilepsy patients for several reasons. Falls during seizures can produce cervical injuries. Sustained postures during prolonged seizure activity can stress cervical structures. The chronic stress and tension of living with a seizure disorder produces musculoskeletal tension patterns. Some anti-epileptic medications affect bone density or muscle function. The cumulative result is that many epilepsy patients have chronic neck pain, suboccipital tension, and related musculoskeletal issues that affect daily comfort and function.
Post-traumatic features
Some forms of epilepsy develop after head or neck trauma. Post-traumatic epilepsy is a recognized entity following moderate to severe traumatic brain injury, with seizures developing in the weeks to years following the trauma. The 2004 paper by Annegers and Coan in Epilepsy Research documented post-traumatic epilepsy as a distinct entity with specific risk factors and patterns (Annegers & Coan, 2004). Patients with post-traumatic epilepsy typically have the seizure disorder plus the broader post-traumatic picture — concussion-related vestibular dysfunction, cervicogenic headache, post-concussion syndrome features, and the upper cervical structural injuries that accompany head trauma.
Sleep disturbance
Sleep problems are common in epilepsy and affect both quality of life and seizure control. Some seizures occur during sleep, disrupting sleep architecture. Anti-epileptic medications affect sleep quality. Anxiety about seizures can interfere with sleep. The relationship runs both ways — poor sleep can lower the seizure threshold, making seizures more likely. Improving sleep is an important component of comprehensive epilepsy management, both for quality of life and for supporting overall seizure control.
Related article

Post-Concussion Syndrome: Your Path to Recovery Through Upper Cervical Care
Jan 08, 2026Anxiety, depression, and stress
Psychological conditions occur at higher rates in epilepsy patients. The chronic nature of the condition, the unpredictability of seizures, the lifestyle restrictions (driving restrictions, employment limitations), and the biological factors related to the underlying brain function all contribute. Anxiety and depression substantially affect quality of life. Stress can lower seizure threshold, creating a cycle where worry about seizures may contribute to their occurrence. Addressing these psychological components is part of comprehensive care.
Medication side effects
Anti-epileptic medications, while essential for seizure control, can produce side effects affecting various body systems. Cognitive effects (sometimes called 'brain fog'), fatigue, mood changes, weight changes, and various physical effects are common. The side effects can substantially affect daily function and quality of life. Patients often must balance seizure control against side effect burden when working with their neurologists on medication optimization.
General health and wellness factors
Beyond specific conditions, general health and wellness factors substantially affect epilepsy patients. Physical fitness, nutrition, posture, ergonomics, stress management, and overall lifestyle factors all influence both quality of life and indirectly the underlying nervous system function that affects seizure threshold. Comprehensive wellness approaches address these foundational factors alongside specific medical management.
Why Upper Cervical Care May Help Epilepsy Patients Feel Better Overall
Upper cervical chiropractic addresses specific components of the broader clinical picture epilepsy patients face. Understanding what upper cervical care can legitimately address clarifies why some epilepsy patients report substantial improvements in quality of life with comprehensive care.
Addressing cervicogenic and tension-type headaches
Many epilepsy patients have cervicogenic headache or tension-type headache contributing to their overall headache burden alongside any migraine they may have. Upper cervical chiropractic specifically addresses the structural cervical factors that produce these headache types. When the underlying cervical structural problems are addressed, the headache patterns often improve substantially. For patients whose headache burden has been a major quality of life issue, this improvement can be transformative even without any direct effect on the seizure disorder itself.
Addressing neck pain and musculoskeletal tension
The neck pain and suboccipital tension that many epilepsy patients experience often responds to upper cervical structural correction. When cervical structural problems are addressed, the chronic muscle tension patterns can normalize, the postural challenges can improve, and the daily musculoskeletal burden can decrease. Patients who had been living with chronic neck pain alongside their epilepsy often experience meaningful relief from the musculoskeletal component.
Addressing post-traumatic features in post-traumatic epilepsy
For patients with post-traumatic epilepsy, the trauma that triggered the seizure disorder essentially always produced concurrent upper cervical structural injury. The 2005 study by Kaale and colleagues in the Journal of Neurotrauma documented that whiplash mechanisms produce upper cervical ligamentous injuries at forces below those required for diagnosable concussion (Kaale et al., 2005). When trauma was sufficient to trigger epilepsy, the upper cervical structures essentially always experienced concurrent injury. Addressing this cervical structural component may improve the broader post-traumatic picture — the headaches, neck pain, vestibular symptoms, and cognitive features that often accompany post-traumatic epilepsy — even though it does not treat the underlying epilepsy itself.
Supporting sleep quality
Improvements in pain levels, muscle tension, and overall comfort often translate into improved sleep quality. Patients who had been waking from pain, sleeping in awkward positions to avoid pain, or experiencing sleep disruption from neck problems often sleep better when these issues are addressed. Better sleep has multiple benefits including potential effects on seizure threshold given the established relationship between sleep deprivation and seizure susceptibility, though specific effects vary by patient.
Supporting overall wellness
The cumulative effect of addressing headaches, neck pain, sleep quality, and general musculoskeletal function is often broader improvement in overall wellness. Patients who feel physically better often feel mentally better, have more energy, engage more with daily activities, and report higher overall quality of life. These broader wellness improvements contribute to the general sense that patients have when they say they feel better with comprehensive care — improvements that reflect addressing multiple coexisting conditions rather than direct treatment of the seizure disorder itself.
What the broader improvement may mean for seizure threshold
Some epilepsy patients report changes in their seizure patterns alongside the broader improvements with comprehensive care. Several factors may contribute when this occurs. Improved sleep can affect seizure threshold. Reduced stress and pain can affect seizure threshold. Better overall wellness may support more stable neurological function. Better medication compliance — as patients feel better and engage more with their care — supports seizure control. These indirect mechanisms differ from a direct treatment effect on the seizure disorder. Patients experiencing such changes should discuss them with their neurologist and never adjust medications based on chiropractic care alone.
Neurological Management Remains Essential
The most important point about epilepsy care: anti-epileptic medications and neurological management remain the essential foundation of treatment that must continue regardless of any complementary care.
Anti-epileptic medications must continue
Patients with epilepsy must continue their anti-epileptic medications as prescribed by their neurologist. These medications are the evidence-based treatments that control seizures and prevent the serious consequences of uncontrolled epilepsy — injury during seizures, status epilepticus, sudden unexpected death in epilepsy (SUDEP), and other catastrophic outcomes. Anti-epileptic medications must never be reduced or stopped based on feeling better with chiropractic care or any other complementary approach. Medication changes must occur only under neurological supervision after appropriate evaluation, monitoring, and slow tapering when indicated.
Related article
Post-Viral POTS: Why Autonomic Symptoms Persist After Infection | Sarasota
Aug 02, 2026Neurological follow-up must continue
Regular neurological follow-up provides essential clinical oversight for epilepsy management. EEG monitoring, medication level monitoring, evaluation of seizure patterns, assessment of medication effectiveness and side effects, and adjustment of treatment based on the clinical course all occur through neurological care. Pursuing chiropractic care should never replace or interfere with neurological follow-up. Patients should inform their neurologist about any complementary care they pursue, and the neurologist should remain the primary manager of the epilepsy itself.
Why this matters specifically
Uncontrolled epilepsy carries serious risks. Breakthrough seizures can cause injuries from falls, motor vehicle accidents (epilepsy patients with seizures should not drive), drowning (showers, swimming, baths), burns (cooking, fires), and other consequences. Status epilepticus is a medical emergency that can be fatal. Sudden unexpected death in epilepsy (SUDEP) is a recognized cause of mortality in epilepsy patients. These risks make medication compliance and ongoing neurological care essential. Reducing medications because of perceived improvements with chiropractic care has produced tragic outcomes, and patients should be explicit with themselves and their families that anti-epileptic medications are non-negotiable regardless of how well they feel.
Coordinated care works best
Optimal care for epilepsy patients involves coordination between providers. The neurologist manages the epilepsy itself with appropriate medications and monitoring. Primary care addresses general health. Chiropractic care, when pursued, addresses specific musculoskeletal and structural components. Other providers (mental health, sleep medicine, physical therapy as appropriate) address other components. Communication between providers improves overall care. Patients should ensure their neurologist knows about any complementary care, and complementary care providers should be willing to work within the framework of the patient's overall medical management.
Important Safety Considerations for Epilepsy Patients
Several safety considerations apply specifically to epilepsy patients considering upper cervical or any other chiropractic care.
Medical clearance before beginning care
Patients with epilepsy should discuss any planned chiropractic care with their neurologist before beginning. The discussion ensures the neurologist knows about the planned complementary care, allows for any specific considerations to be addressed, and supports coordinated care. Some specific situations may warrant additional caution or specific precautions.
Avoiding aggressive manipulation
Aggressive cervical manipulation involving sudden high-velocity movements may not be appropriate for all epilepsy patients. Upper cervical chiropractic uses precision-based low-force corrections rather than aggressive manipulation — there is no twisting, no popping, no full-spine manipulation. This precision-based approach is particularly appropriate for patients with neurological conditions where sudden cervical manipulation could be problematic. Patients should ensure any chiropractic care they pursue uses appropriate gentle techniques rather than aggressive manipulation.
Active seizure considerations
Patients in active phases of poorly controlled epilepsy, those who have recently had seizures, or those in post-ictal states should not receive chiropractic adjustments until they are stable. Care should be timed for periods when the patient is medically stable and has had appropriate neurological evaluation. Acute medical situations should be managed through medical channels rather than through chiropractic care.
Hypermobility considerations
Some epilepsy patients also have connective tissue conditions like Ehlers-Danlos syndrome. Patients with hypermobility conditions require specialized evaluation, and the combination of hypermobility with potential craniocervical instability may require neurosurgical evaluation rather than standard chiropractic care.
Never reduce medications
The most important safety point bears repeating: patients with epilepsy must never reduce or discontinue their anti-epileptic medications based on feeling better with chiropractic care. Medication changes occur only through neurological management with appropriate monitoring. The risks of uncontrolled seizures are serious and potentially life-threatening.
What an Upper Cervical Evaluation at Sarasota Upper Cervical Involves
For epilepsy patients pursuing upper cervical evaluation as part of comprehensive care addressing coexisting conditions, our evaluation process is designed for precision and safety.
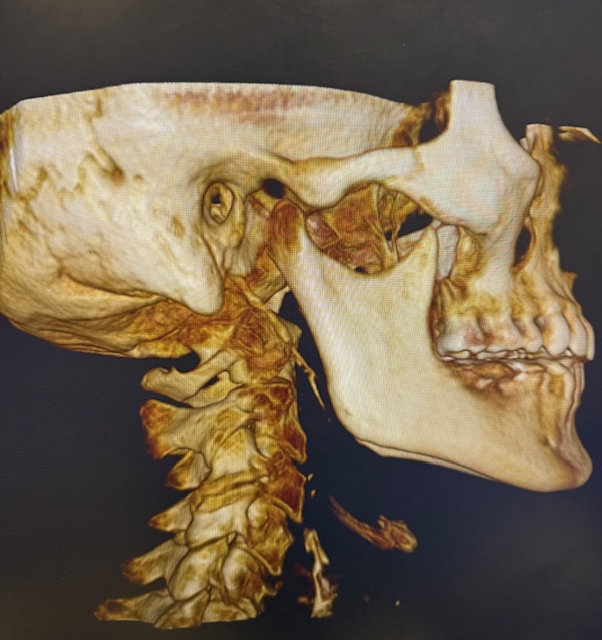
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree. The imaging identifies whether structural problems are present at the craniocervical level that may be contributing to the coexisting conditions epilepsy patients face — headaches, neck pain, post-traumatic features. The imaging provides objective measurement rather than assumption that structural problems are necessarily present.
Objective testing before any intervention
Leg length analysis and paraspinal infrared thermography are performed before any adjustment, and corrections are delivered only when objective findings indicate a structural shift. This principle of restraint guided by data is particularly important for patients with neurological conditions — interventions are objective-finding-based rather than performed routinely on assumption.
Related article

Tinnitus Relief: Understanding the Upper Cervical Connection to Ear Ringing
Jan 26, 2026Precision without manipulation
Corrections, when delivered, are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. For epilepsy patients — whose neurological systems require careful consideration — this precision is essential. The approach is fundamentally different from aggressive cervical manipulation that may not be appropriate in neurological patients.
Care coordination
Care for epilepsy patients should occur in coordination with their neurological management. We encourage patients to inform their neurologist about chiropractic care, and we work within the framework of the patient's overall medical management. Our care addresses specific structural components; the neurologist manages the epilepsy itself.
Realistic expectations
Epilepsy patients considering upper cervical care should have realistic expectations. The care may help with headaches, neck pain, and broader wellness factors. It is not treatment for the seizure disorder itself. Improvements develop gradually over weeks to months when they occur. Continued neurological management remains the foundation of epilepsy care. Either outcome — substantial improvement in coexisting conditions or limited improvement — provides useful information about what the cervical structural component was contributing to the broader picture.
When Upper Cervical Evaluation May Be Worth Considering
Upper cervical evaluation may be worth considering for epilepsy patients in specific situations:
You have chronic headaches alongside your epilepsy that have not responded fully to standard headache treatment. You have chronic neck pain, suboccipital tension, or restricted cervical range of motion that affects your quality of life. Your epilepsy developed after head or neck trauma, and you continue to have post-traumatic features (post-concussion vestibular symptoms, cervicogenic headache, broader post-traumatic picture). You experienced falls during seizures that produced cervical injuries you have not specifically addressed. You have prior concussions or significant neck trauma layered on top of your current presentation. You are pursuing comprehensive wellness care alongside your essential neurological management.
For patients without significant coexisting headache or neck pain issues, without trauma-related involvement, and without other clear cervical features, upper cervical evaluation may have less to offer. The intervention is most relevant for the coexisting conditions epilepsy patients commonly have, not as general epilepsy care for patients without these specific features.
Important prerequisites before pursuing care: discuss with your neurologist, ensure your epilepsy is appropriately managed, never plan to reduce anti-epileptic medications based on chiropractic care, ensure any provider you see uses precision-based low-force techniques rather than aggressive manipulation, and maintain your essential neurological follow-up.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Where to Go From Here
Patients with epilepsy face complex clinical pictures that involve more than just seizure management. The coexisting conditions — chronic headaches, neck pain, post-traumatic features, sleep disturbance, and broader wellness factors — substantially affect quality of life. Comprehensive care addressing these multiple components, alongside continued essential neurological management of the epilepsy itself, can meaningfully improve overall function and wellbeing for many patients.
Upper cervical chiropractic, properly understood and properly framed, can be one component of comprehensive care for epilepsy patients with relevant coexisting conditions. The care addresses structural cervical factors contributing to headaches, neck pain, and post-traumatic features. It is not treatment for epilepsy itself. Anti-epileptic medications and neurological follow-up remain essential and must continue regardless of any complementary care. The clinical improvements many epilepsy patients report with comprehensive care reflect improvements in multiple coexisting conditions and overall wellness, supporting better quality of life alongside continued seizure management.
For patients in Sarasota and surrounding communities with epilepsy and coexisting conditions affecting your quality of life, Sarasota Upper Cervical provides structural evaluation focused on the C1 and C2 region using three-dimensional CBCT imaging and objective testing protocols. We work alongside your medical team, providing one specific component of comprehensive care while your neurologist continues to manage the essential epilepsy treatment. Our approach uses precision-based low-force corrections rather than aggressive manipulation, appropriate for patients with neurological conditions.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Bigal, M. E., Lipton, R. B., Cohen, J., & Silberstein, S. D. (2003). Epilepsy and migraine. Epilepsy & Behavior, 4(Suppl 2), S13–S24.
Velioglu, S. K., Boz, C., & Ozmenoglu, M. (2005). The impact of migraine on epilepsy: A prospective prognosis study. Cephalalgia, 25(7), 528–535.
Annegers, J. F., & Coan, S. P. (2000). The risks of epilepsy after traumatic brain injury. Seizure, 9(7), 453–457.
Christensen, J., Pedersen, M. G., Pedersen, C. B., Sidenius, P., Olsen, J., & Vestergaard, M. (2009). Long-term risk of epilepsy after traumatic brain injury in children and young adults: A population-based cohort study. The Lancet, 373(9669), 1105–1110.
Tellez-Zenteno, J. F., Patten, S. B., Jetté, N., Williams, J., & Wiebe, S. (2007). Psychiatric comorbidity in epilepsy: A population-based analysis. Epilepsia, 48(12), 2336–2344.
Manni, R., & Terzaghi, M. (2010). Comorbidity between epilepsy and sleep disorders. Epilepsy Research, 90(3), 171–177.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Chiropractic care focuses on the structure and function of the spine and nervous system. Upper cervical chiropractic is not a treatment for epilepsy and is not a substitute for anti-epileptic medications or neurological management. Patients with epilepsy must continue their anti-epileptic medications as prescribed by their neurologist and maintain regular neurological follow-up. Medication changes must occur only under neurological supervision. Any chiropractic care should be coordinated with the patient's neurologist. Patients with epilepsy considering complementary care should discuss it with their neurologist beforehand. The clinical observations described in this article reflect improvements in coexisting conditions and overall wellness rather than direct treatment of seizure disorders. No claim is made or implied that upper cervical chiropractic cures or treats epilepsy or any other specific disease. Individual results vary.



Leave a comment