
"Why the upper cervical spine is one of the most overlooked sources of vertigo — and what precision imaging and a gentle correction can do about it"
Vertigo is exhausting. The room spins, your stomach turns, you don’t trust your own head to stay still. Most people who walk into our Sarasota office have already been through it — the urgent care visit, the ENT workup, the Epley maneuver, the medications. Sometimes they get relief. Often they get a label, a prescription, and the quiet sense that no one really knows where their vertigo is coming from.
Schedule Your Appointment
Schedule appointmentWhat gets missed in most of those workups is the upper cervical spine. Not because it doesn’t matter — it matters a great deal — but because it sits in the gap between specialties. ENTs look at the inner ear. Neurologists look at the brain. Very few clinicians look at the small joints at the top of the neck where the brainstem, the inner ear, and the spinal cord all meet. And those joints, when they are misaligned, can drive vertigo through several mechanisms at once.
The Vestibular Nucleus Listens to Three Inputs — and One of Them Is Your Neck
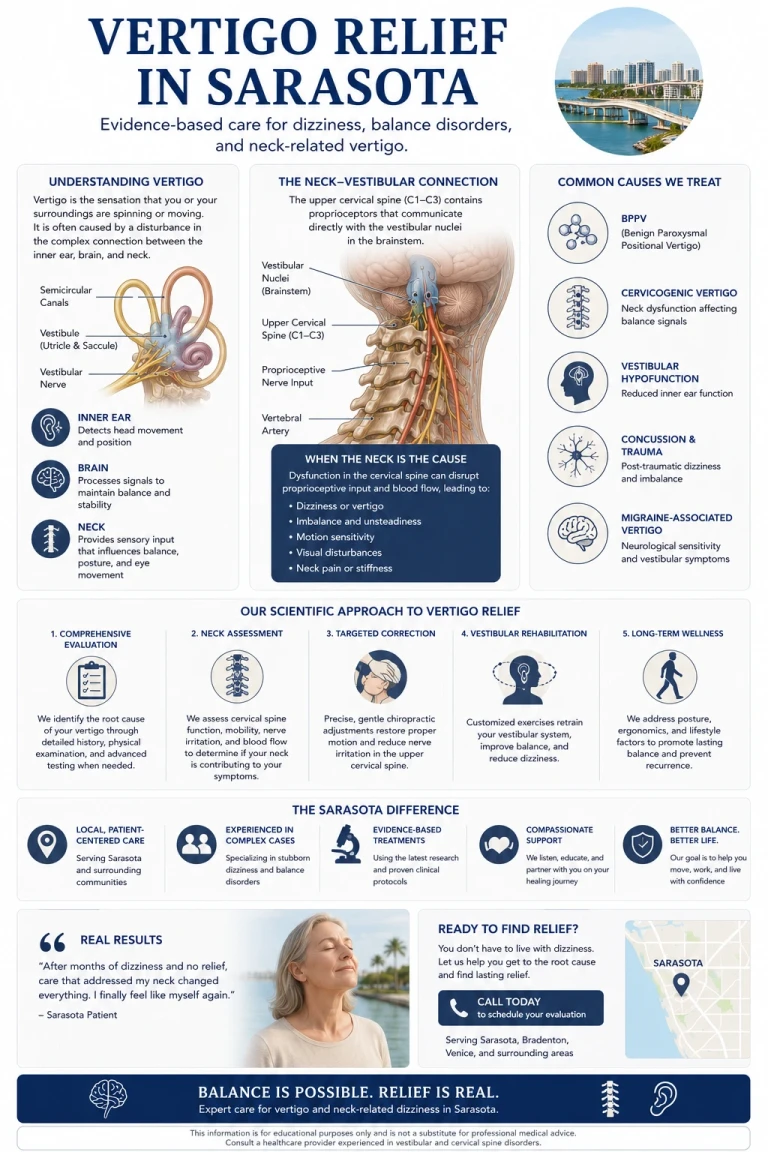
Balance is not produced in the inner ear alone. It is produced in the brainstem, in a structure called the vestibular nuclei, where three different streams of information come together: the inner ear, the eyes, and the proprioceptive sensors in the upper cervical spine. The brain compares all three. When they agree, you feel steady. When they disagree, you feel dizzy.
The upper cervical spine — the atlas (C1) and axis (C2) — contains the highest density of mechanoreceptors anywhere in the spinal column. These joint sensors continuously feed the vestibular nuclei information about where your head is, how it is moving, and how it relates to your body. When the joints are aligned and moving well, the input is accurate. When they are misaligned or restricted, the input becomes distorted — and the vestibular nuclei receive a signal that conflicts with what the inner ear and eyes are reporting.
That mismatch is what the brain experiences as vertigo, unsteadiness, or disequilibrium. The inner ear may be perfectly healthy. The crystals may be exactly where they belong. But if the input from the upper cervical joints is wrong, the brain still gets confused. This is one reason canalith repositioning maneuvers sometimes fail — the inner ear was never the actual driver.
The Craniocervical Junction: A Choke Point for Brain Fluid Dynamics
The craniocervical junction (CCJ) is where the skull meets the atlas. Almost everything the brain depends on physically passes through this region — the brainstem, the vertebral arteries, the internal jugular veins, the cerebrospinal fluid (CSF) channels, and several cranial nerves. When the CCJ is aligned, these structures move freely. When it is misaligned, fluid dynamics can be disrupted in several ways at once, and the inner ear is one of the most sensitive structures to those disruptions.
Related article
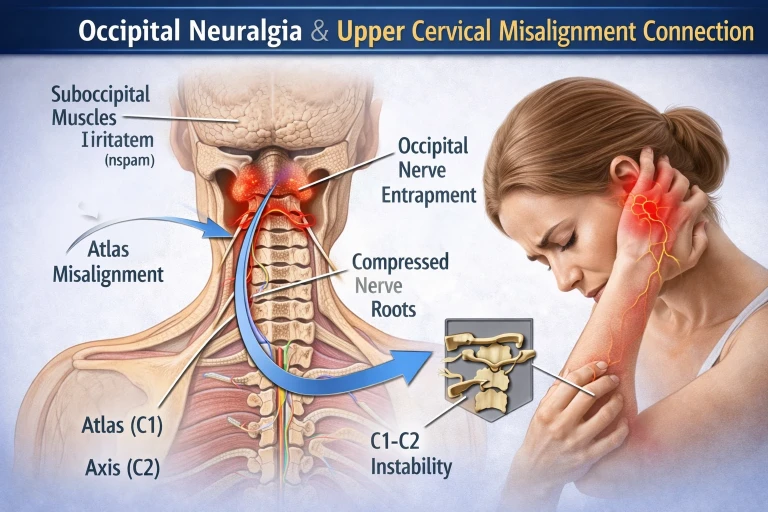
Sharp Pain at the Base of the Skull? | Lakewood Ranch Upper Cervical Care |Occipital Neuralgia
Mar 05, 2026First, CSF drainage can be impaired. CSF moves between the brain and the spinal cord through a narrow channel at the craniocervical junction. When that channel is mechanically distorted, CSF flow becomes turbulent or restricted. The result is rising intracranial pressure — not always to a dangerous degree, but often enough to subtly change the pressure environment inside the skull.
Second, jugular venous drainage can be reduced. The internal jugular vein passes directly in front of the atlas. When the atlas is rotated or shifted, the vein can be partially compressed, slowing the rate at which blood drains out of the skull. Blood that doesn’t drain backs up, and that pressure has to go somewhere.
The inner ear is exquisitely pressure-sensitive. The semicircular canals and the cochlea are filled with fluid — endolymph and perilymph — whose pressure relationships have to stay precisely balanced for normal hearing and balance. When intracranial pressure rises, when venous drainage slows, when fluid dynamics shift, the inner ear feels it. Patients can experience this as vertigo, fullness in the ear, tinnitus, muffled hearing, or all of the above — often without any abnormality showing up on an ENT workup.
The Vestibulocochlear Nerve and Denticulate Cord Tension
The vestibulocochlear nerve (cranial nerve VIII) is the wiring that carries signals from the inner ear to the brainstem. It exits the brainstem in the immediate vicinity of the craniocervical junction. Anything that mechanically stresses this region can potentially interfere with the function of this nerve.
This is where the denticulate (dentate) ligament theory becomes relevant. The denticulate ligaments are thin sheets of connective tissue that anchor the spinal cord laterally to the dura mater at every spinal level. They are strongest in the cervical region. Dr. John Grostic first proposed in 1988 that misalignments of the upper cervical vertebrae can create torsional and tensile stress that travels through the denticulate ligaments to the spinal cord and brainstem. The hypothesis has since gained meaningful support in mainstream neurosurgical literature — a peer-reviewed analysis of cervical spondylotic myelopathy concluded that the pattern of neuropathology in the disease more closely matches the predicted stress pattern of dentate ligament tension than direct compression.
In practical terms, this means that what happens mechanically at the top of the neck doesn’t stay at the top of the neck. Tension transmits up through the dura into the brainstem, where the vestibulocochlear nerve and the vestibular nuclei live. It is an indirect mechanism, but a real one, and it is one of the more plausible explanations for why upper cervical misalignment can produce hearing and balance symptoms that look identical to inner ear disease.
Loss of Cervical Curve: When the Whole Neck Pulls on the Brainstem

A healthy neck has a forward curve — a cervical lordosis — of roughly 30 to 40 degrees. That curve isn’t cosmetic. It allows the spinal cord to sit at its natural length inside the spinal canal, without being stretched. When the curve is lost, straightened, or reversed, the spinal canal effectively becomes longer than the cord was designed for. The cord doesn’t shorten to match. It gets pulled.
Because the cord is anchored to the spinal canal by the denticulate ligaments, that pull is transmitted through those attachments. Neurosurgical literature has described this phenomenon directly: loss of cervical lordosis can create traction on the spinal cord and a downward caudal pull on the brainstem and cerebellar tonsils. In some patients this contributes to or worsens a Chiari-like picture. In many more, it simply means the brainstem is operating under a low-grade, constant mechanical tension it was never designed to handle.
The vestibular nuclei, the vestibulocochlear nerve, and the postural control centers all sit in the brainstem. A brainstem under tension is a brainstem that processes balance information less efficiently. Patients with significant loss of cervical curve frequently describe a chronic, low-grade unsteadiness that is worse at the end of the day, worse with screen time, and worse when they are tired — a pattern that fits a brainstem doing extra work to maintain function under mechanical load.
CBCT Imaging: Seeing the Picture Clearly
Before any care begins in our Sarasota office, we use Cone Beam Computed Tomography (CBCT) imaging of the upper cervical spine. CBCT is a precision imaging tool that produces three-dimensional views of the skull base, atlas, axis, and surrounding structures — detail that flat two-dimensional X-rays cannot provide.
Every craniocervical junction is built differently. The angles, the orientations, and the relationships between the skull, C1, and C2 are unique to each person. Without precision measurements, an upper cervical correction is a guess. With them, the correction can be specific, gentle, and matched to your exact anatomy. For a patient who has been told their vertigo is unexplained, this is often the first time the structure most likely to be driving it is being looked at directly.
No Twisting. No Cracking. No Pulling of the Neck
Most people picture a chiropractic adjustment as a fast head-turn and a popping sound. That is not what we do. The correction we deliver is specific, low-force, and based directly on the measurements taken from your CBCT scan. There is no twisting, cranking, or pulling. No cavitation noise. You lie on your side with your head supported. The correction takes seconds.
For someone whose vertigo has been triggered by neck movement for months or years, this matters a great deal. The last thing a sensitized vestibular system needs is a forceful head rotation. Our approach is designed specifically to avoid that — to give the brainstem cleaner input from the upper cervical joints without adding stress to a system that is already under load.

Gentle does not mean ineffective. Gentle means we are working with the nervous system, not against it. The goal is to restore mechanical and neurological balance to the craniocervical junction so the brainstem, the vestibular nuclei, and the inner ear can do their jobs without conflicting input.
Who This Tends to Help
The patient we see most often in this category has a story that sounds familiar. Vertigo that started after a fall, a car accident, a concussion, a dental procedure, or sometimes nothing identifiable at all. A workup that came back “unremarkable.” Maybe a diagnosis of BPPV. Maybe vestibular therapy. Maybe medication. Some improvement, then relapse. A growing suspicion that the inner ear isn’t really the answer.
Common features include vertigo that worsens with certain head positions, neck stiffness or pain that the patient may not have connected to the dizziness, symptoms that get worse with stress, fatigue, or prolonged screen time, and a sense of unsteadiness that doesn’t fit any clean diagnostic box. None of those features are diagnostic on their own — but together, they raise the question of whether the upper cervical spine deserves a closer look.
A Realistic First Visit, and a Real Path Forward
A first visit in our Sarasota office includes a thorough consultation, a focused examination, and CBCT imaging of the upper cervical spine. We pay particular attention to your full history — including any head or neck trauma, even decades old, because those events are often where this story starts. After we review the imaging with you, we will tell you honestly whether upper cervical care looks like a good fit. If it is, we build a plan. If it is not, we say so and point you toward what is more likely to help.
Vertigo doesn’t have to be a permanent condition you manage around. For many patients, the answer is not in the inner ear — it is in the structure at the top of the neck that quietly influences everything the inner ear and the brainstem are trying to do. Upper cervical chiropractic care, delivered with precision imaging and a gentle, non-twisting correction, addresses that structure directly.
Ready to find out if your vertigo is coming from your neck? Schedule a consultation at our Sarasota office to start with a complete upper cervical evaluation and CBCT imaging.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Persistent or severe vertigo should be evaluated by a qualified healthcare provider to rule out serious causes including stroke, central nervous system disease, and other medical conditions. Upper cervical chiropractic care does not diagnose, treat, or cure any specific vestibular



Leave a comment