
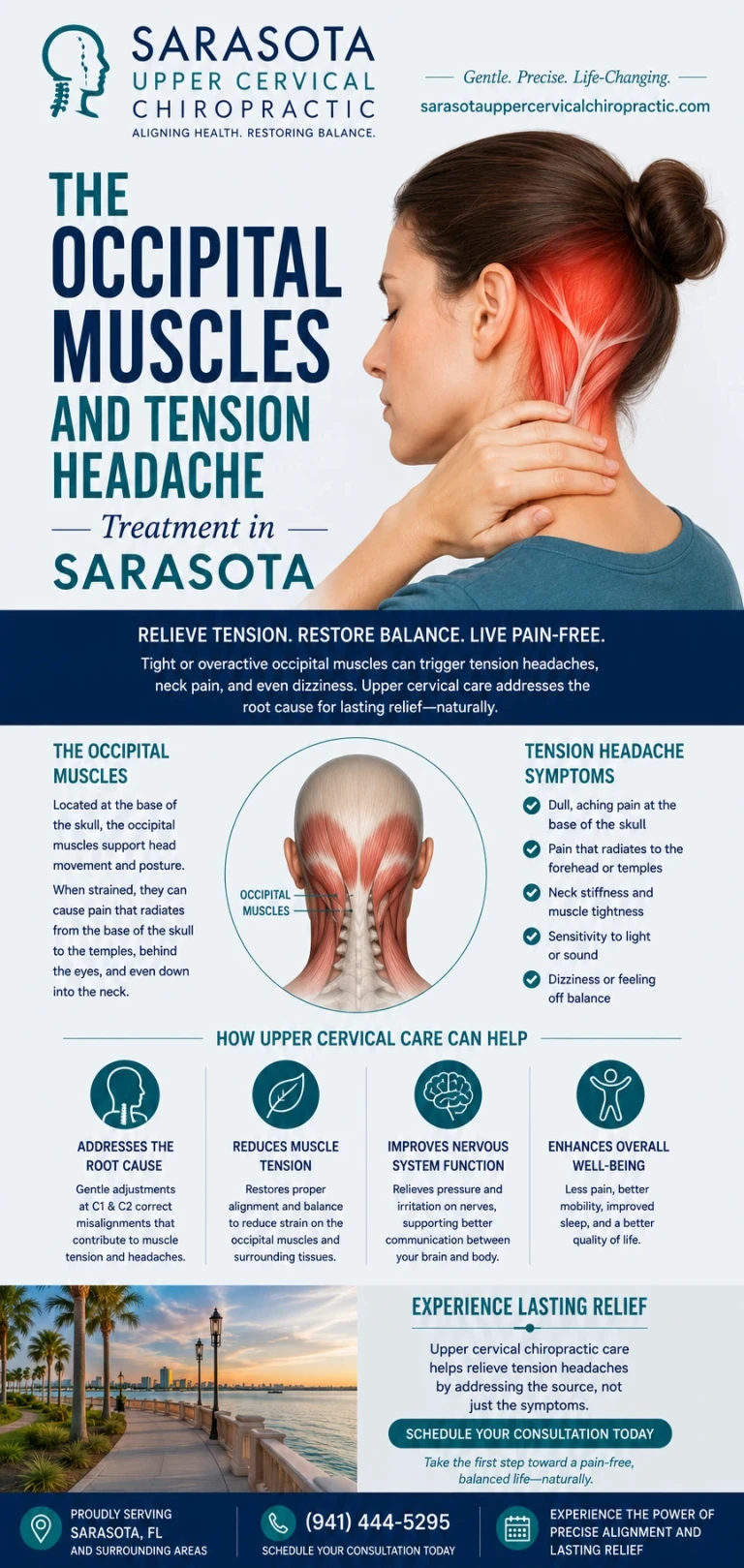
"Tension-type and cervicogenic headaches often originate at the base of the skull where small deep muscles connect directly to the dura mater through an anatomical structure called the myodural bridge. Understanding this mechanism clarifies why upper cervical structural problems can be a root cause of chronic head pain"
Many patients with chronic tension-type or cervicogenic headaches describe a specific pattern: the pain begins at the base of the skull, spreads upward over the back of the head, and often extends to the temples, forehead, or behind the eyes. The pain is usually a dull, pressing, or band-like quality rather than the throbbing pain of vascular headache. It is often worse with sustained postures, after prolonged computer work, with stress, or after sleeping in awkward positions. Patients frequently describe tight muscles at the base of the skull alongside the headache, and many have learned that pressing on these tight areas temporarily reduces the pain. This pattern is not coincidental — it reflects a specific anatomical relationship between the deep occipital muscles and the dura mater that has been documented in mainstream anatomy research.
Schedule Your Appointment
Schedule appointmentThe structure that creates this anatomical relationship is called the myodural bridge — a direct connective tissue connection between specific small muscles at the base of the skull and the dura mater that surrounds the spinal cord and brain. When the 1995 paper by Hack and colleagues in Spine first documented this connection in detail (Hack et al., 1995), it provided an anatomical explanation for clinical observations that practitioners had been making for decades: that tension in the deep occipital muscles can produce headache through mechanical effects on the dura. Subsequent research has confirmed and expanded the original findings, establishing the myodural bridge as established anatomy rather than speculation.
For patients in Sarasota and surrounding communities dealing with chronic tension-type or cervicogenic headaches, understanding the myodural bridge clarifies why structural problems at the upper cervical junction can be a root cause of head pain. Standard headache management — addressing trigger factors, stress reduction, postural improvements, and medications when appropriate — forms the foundation of care. Within that framework, structural evaluation of the upper cervical junction can be a relevant consideration for patients whose headaches persist despite standard management, particularly when the headache pattern matches the cervicogenic and tension-type features that suggest cervical involvement.
To book a FREE evaluation call 941 259-1891.
This article walks through the anatomy of the deep occipital muscles, the discovery and structure of the myodural bridge, how the bridge produces dural tension when the muscles are chronically tight, why dural tension produces headache, how upper cervical misalignment causes the occipital muscle tension that drives this mechanism, and where upper cervical evaluation fits into comprehensive care for appropriate headache patients.
The Deep Occipital Muscles: Small Muscles With Outsized Importance
The muscles at the base of the skull are among the smallest in the body but have anatomical and functional importance well beyond their size. Understanding these muscles is essential for understanding how they contribute to headaches through the myodural bridge mechanism.
The suboccipital muscle group
The suboccipital muscles form a small but critical group at the base of the skull. Four muscles make up the group: the rectus capitis posterior major, the rectus capitis posterior minor, the obliquus capitis superior, and the obliquus capitis inferior. These muscles connect the skull (occiput) to the first two cervical vertebrae (atlas and axis), allowing fine control of head position relative to the upper neck. The muscles are deep — covered by the larger trapezius, semispinalis capitis, and other superficial muscles that patients can feel from the surface. The suboccipital muscles themselves are not directly palpable in most patients but their effects are felt as the deep tension or tightness at the base of the skull that headache patients commonly describe.
The rectus capitis posterior minor specifically
Of the four suboccipital muscles, the rectus capitis posterior minor (RCPM) is the most important for the myodural bridge mechanism. The RCPM is a small muscle that runs from the posterior tubercle of the atlas (the back surface of the first cervical vertebra) upward to attach to the inferior aspect of the occipital bone, just below the inferior nuchal line. It is the smallest of the suboccipital muscles, but its anatomical position and its connection to the dura mater through the myodural bridge give it disproportionate clinical importance for headache mechanisms.
Why these muscles are proprioceptively dense
Beyond their mechanical role, the suboccipital muscles are extraordinarily rich in proprioceptive receptors. The 2001 study by Kulkarni and colleagues in Neurology India documented exceptionally high muscle spindle density in the suboccipital muscles — substantially higher than in most other muscles in the body (Kulkarni et al., 2001). This proprioceptive density reflects the muscles' role in providing precise information about head position to the brainstem. The receptors send continuous signals about muscle length and tension, contributing to balance processing and providing input that the brain uses for spatial orientation. When these muscles are chronically tight or in abnormal positions, the proprioceptive signals they send are distorted, with consequences extending beyond just the local musculoskeletal effects.
Common tension patterns
The suboccipital muscles are prone to chronic tension in patients with various conditions and lifestyle factors. Forward head posture from prolonged computer or device use places sustained demand on these muscles. Stress and anxiety produce protective muscle tightening throughout the cervical region, including the suboccipital area. Sleep posture problems can produce overnight tension that persists into the day. Trauma — concussion, whiplash, sports injuries — can produce sustained altered patterns in these muscles. Upper cervical structural misalignment can produce compensatory tension as the muscles work to maintain head position despite structural compromise. Each of these factors contributes to the chronic suboccipital tension that drives the myodural bridge mechanism for headache.
Why patients feel them as tight
Patients with chronic suboccipital tension often describe a sense of tightness, pressure, or knotted muscles at the base of the skull. While the suboccipital muscles themselves are too deep to palpate directly, their tension affects the overlying muscles (trapezius, semispinalis capitis) and produces detectable tender points in the surface anatomy. The 'knots' that patients feel at the base of the skull often reflect the broader tension pattern that includes the deep suboccipital involvement. Pressing on these tender areas often produces both local relief and reduction in headache symptoms, reflecting the connection between the muscles and the head pain.
The Myodural Bridge: A Direct Connection Between Muscle and Dura Mater
The myodural bridge is the specific anatomical structure that creates the direct mechanical relationship between the rectus capitis posterior minor and the dura mater. Understanding this structure clarifies why occipital muscle tension can produce headaches through mechanical effects on intracranial structures.
What the myodural bridge is
The myodural bridge is a band of dense connective tissue — specifically, a continuation of the RCPM tendon and surrounding fascial tissue — that extends from the deep surface of the RCPM through the posterior atlanto-occipital interspace to attach directly to the spinal dura mater. The bridge is not a passive ligament that holds two structures in their normal positions; it is a continuous connective tissue continuum that allows mechanical force to transmit directly from the muscle to the dural tissue. When the muscle contracts or remains chronically tight, the resulting tension propagates along the bridge to the dura.

The Hack 1995 discovery and subsequent research
While clinicians had long suspected a connection between deep occipital muscles and headache, the specific anatomical structure was first documented in detail in the 1995 paper by Hack and colleagues published in Spine (Hack et al., 1995). The researchers performed careful cadaveric dissection and microscopic examination, documenting the continuity of connective tissue from the RCPM muscle through the posterior atlanto-occipital membrane to the dura mater. The finding was significant because it provided a specific anatomical mechanism for how cervical muscle tension could affect intracranial structures. Subsequent research by Mitchell and colleagues (1998 Clinical Anatomy) and others has confirmed and expanded the findings, establishing the myodural bridge as a consistent anatomical feature rather than a rare variant.
The structure of the bridge
Detailed anatomical study has revealed the bridge as more complex than a simple band of tissue. The connective tissue continuum involves several components: fibers from the RCPM tendon itself, connections through the posterior atlanto-occipital membrane (a ligamentous structure between the skull and atlas), and direct attachments to the dura mater. The arrangement creates a continuous mechanical pathway from the muscle to the dural tissue, with the various components functioning together to transmit force. The bridge is present consistently across populations, with anatomical variations in detail but with the fundamental structure consistently identified.
The dura mater that the bridge attaches to
The dura mater is the tough, fibrous outer covering of the central nervous system. It surrounds the brain (the cranial dura) and the spinal cord (the spinal dura), with continuous communication between the two. The dura is not a passive covering but a structurally important and physiologically active tissue. It contains substantial blood supply, has its own innervation, and serves multiple roles including mechanical protection, structural support, and contribution to cerebrospinal fluid dynamics. Critically for headache mechanisms, the dura is one of the most pain-sensitive structures in the head, with extensive innervation by branches of the trigeminal nerve that mediate the headache response to dural stimulation.
Why the dural attachment matters
When the RCPM is chronically tight, the tension transmitted through the myodural bridge produces sustained mechanical loading of the dura mater. The dura responds to this mechanical loading through its sensory innervation, producing pain signals that the brain interprets as headache. The pain pattern matches what patients with cervicogenic and tension-type headaches commonly describe — beginning at the base of the skull (where the bridge originates), spreading through the head (following the dural sensory distribution), and often involving the trigeminal-innervated regions of the face and head.
Why Dural Tension Produces Headache
Understanding how dural tension translates into headache symptoms requires understanding the dural pain mechanism. The dura is one of the most studied pain-producing structures in the head, and the mechanisms by which it produces pain are well-characterized.
The dural sensory innervation
The dura mater receives extensive sensory innervation primarily from branches of the trigeminal nerve. The ophthalmic division of the trigeminal nerve (V1) provides the most extensive dural innervation, particularly to the supratentorial dura (the dura covering the upper part of the brain). The maxillary division (V2) and mandibular division (V3) provide additional innervation. The upper cervical nerves (C1, C2, C3) also contribute to dural innervation, particularly the cervical dura around the upper spinal cord. This innervation pattern creates the sensory framework through which dural stimulation produces headache.
The trigeminovascular system
The trigeminal innervation of the dura is part of the broader trigeminovascular system that is central to many headache mechanisms including migraine. The trigeminovascular system involves the trigeminal nerve, its connections to dural and cranial blood vessels, the brainstem regions where trigeminal signals are processed (including the trigeminal nucleus caudalis), and the broader connections that produce headache pain. The 2017 framework by Goadsby and colleagues described migraine as fundamentally a disorder of sensory processing involving this system (Goadsby et al., 2017). For the myodural bridge mechanism, the relevant aspect is that mechanical stimulation of the dura activates the trigeminovascular pain pathway.
The trigeminocervical complex
The connection between cervical structures and trigeminal-based headache mechanisms operates partly through the trigeminocervical complex — a brainstem region where input from the trigeminal nerve and the upper cervical nerves converge. The 2003 paper by Bartsch and Goadsby in Current Pain and Headache Reports established this convergence as the anatomical link between cervical involvement and headache mechanisms (Bartsch & Goadsby, 2003). When the dura is mechanically stressed by the myodural bridge mechanism, the resulting signals interact with cervical afferent input in the trigeminocervical complex, contributing to the headache pattern that has both cervical and trigeminal features.
Why mechanical dural tension matters
Mechanical stimulation of the dura can activate the same pain pathways that other dural insults activate. The dura's sensitivity to mechanical stimulation has been documented in clinical contexts including post-lumbar puncture headache, where altered dural mechanics from CSF leakage produces characteristic positional headache. In the myodural bridge context, sustained mechanical loading from chronically tight RCPM can produce the dural pain signaling that manifests as the chronic tension-type or cervicogenic headache pattern. The mechanical mechanism is similar in principle to other documented dural pain mechanisms; the source of the mechanical loading is what differs.
The pattern of pain produced
Headaches produced through the myodural bridge mechanism typically follow specific patterns. Pain often begins at the base of the skull where the RCPM and the bridge are located. The pain spreads upward and forward, following the dural sensory distribution. Many patients describe a 'cap' or 'band' of pain across the back of the head, sometimes extending to the temples, forehead, or behind the eyes. The pain quality is typically dull, pressing, or band-like rather than throbbing or pulsating. The pattern is consistent with what is described clinically as cervicogenic headache and tension-type headache — categories that may share substantial underlying mechanism through the myodural bridge pathway.
How Upper Cervical Misalignment Causes Occipital Muscle Tension
The chain of mechanisms reaching from the myodural bridge to headache requires sustained tension in the RCPM and other occipital muscles. Understanding how upper cervical structural problems produce that sustained tension clarifies why structural correction may address the root cause of the headache pattern.
The structural challenge of the upper cervical junction
The upper cervical junction — where the skull articulates with the atlas (C1), and the atlas articulates with the axis (C2) — is the most mobile and most mechanically demanding region of the spine. The atlas does not have a vertebral body like other vertebrae; it is essentially a ring of bone that supports the weight of the skull and allows for substantial movement. The arrangement is mechanically efficient when alignment is correct but problematic when alignment is disrupted. Even small structural misalignments at this level produce disproportionate mechanical consequences.
Compensatory muscle patterns
When the upper cervical structures are misaligned, the surrounding muscles must work continuously to maintain functional head position. The deep suboccipital muscles, including the RCPM, are particularly affected because they are the muscles specifically designed to control fine head position relative to the atlas and axis. With structural misalignment present, these muscles cannot achieve their normal resting length and tension patterns. They must remain partially contracted to compensate for the structural problem, producing the chronic tension that drives the myodural bridge mechanism.
Why this compensation is unsustainable
Muscles are designed for cyclical activity — periods of contraction during use alternating with periods of relaxation during rest. The compensatory tension required to maintain function with structural misalignment violates this design principle. The muscles remain partially contracted continuously, leading to multiple consequences. Chronic muscle ischemia (reduced blood flow) develops in the persistently contracted tissue. Metabolic byproducts accumulate as the muscles cannot clear them through normal contraction-relaxation cycles. Trigger points form in the chronically tense tissue. The proprioceptive signaling from the muscles becomes distorted as the receptors send signals reflecting the abnormal state. And critically for the headache mechanism, the sustained tension transmits through the myodural bridge to the dura, producing the chronic headache pattern.
Related article
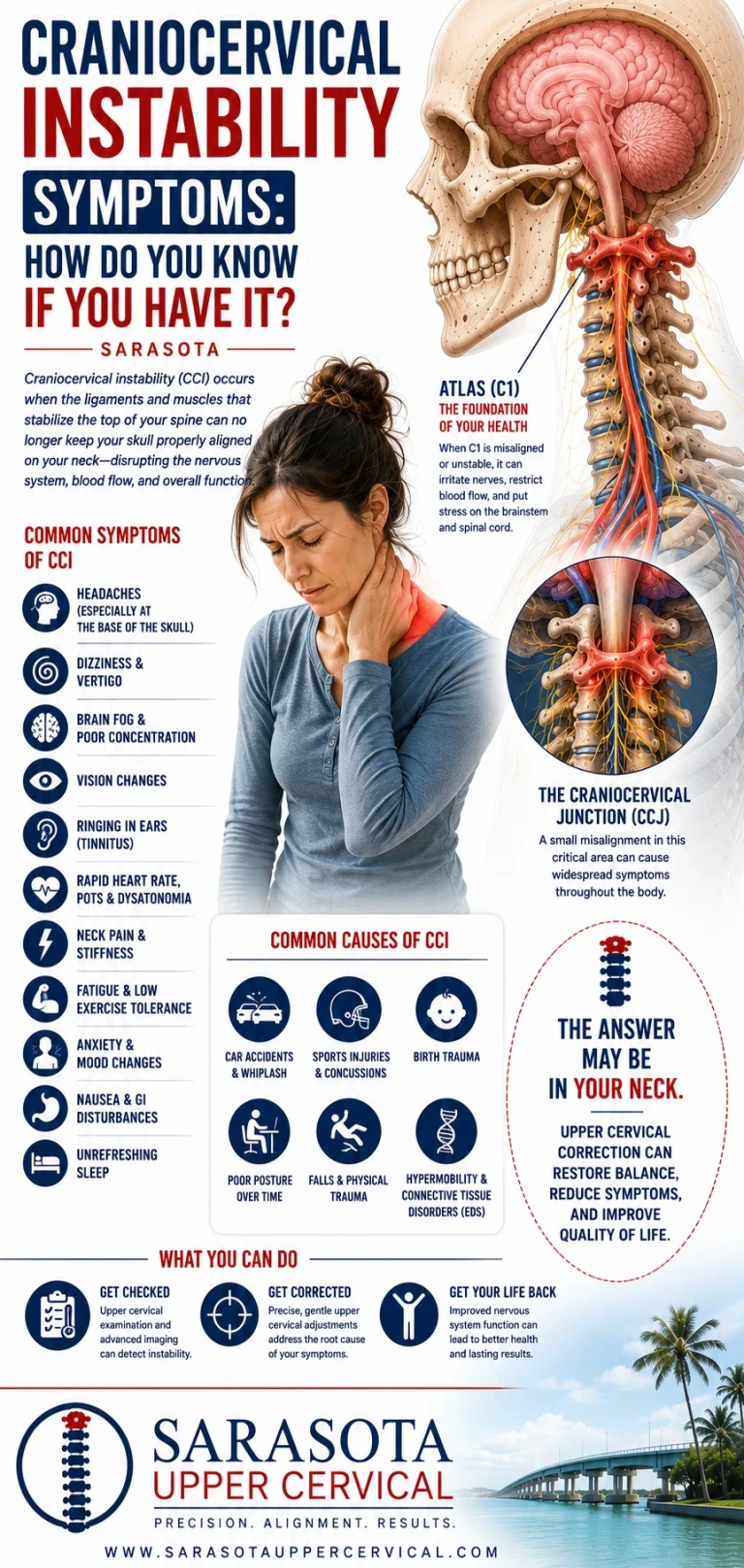
Craniocervical Instability Symptoms: How Do You Know If You Have It? | Sarasota
Jul 29, 2026The pain-tension cycle
Once the chronic tension-headache pattern is established, the system can become self-perpetuating. The headache pain produces protective muscle guarding that increases the tension. The increased tension amplifies the myodural bridge effect and worsens the headache. The patient becomes anxious about the persistent pain, which produces additional muscle tension through stress mechanisms. Sleep is disrupted, reducing the recovery that would normally allow some resolution of the tension. The cycle perpetuates the condition, with the underlying structural cause continuing to drive the entire pattern.
Why standard treatments often produce limited results
Standard headache treatments often produce only partial relief in patients with this underlying mechanism. Pain medications can reduce the headache pain temporarily but do not address the underlying tension or its structural cause. Muscle relaxants can reduce tension temporarily but do not address why the tension keeps recurring. Massage and superficial muscle work can produce temporary relief but cannot reach the deep suboccipital muscles effectively. Postural correction helps but cannot resolve the underlying structural problem if structural misalignment is the root cause. The treatments address downstream effects without addressing the root cause.
Which Headaches the Myodural Bridge Mechanism Relates To
The myodural bridge mechanism is most relevant to specific headache types and patterns. Understanding which headaches relate to this mechanism — and which do not — helps clarify when upper cervical evaluation may be appropriate.
Cervicogenic headache
Cervicogenic headache is the headache type most directly related to the myodural bridge mechanism. Cervicogenic headache is defined as headache arising from cervical structures, with specific clinical features including unilateral or dominantly one-sided pain, pain that begins in the neck and spreads to the head, exacerbation by neck movement or sustained posture, restricted cervical range of motion, and reduced pain with appropriate cervical interventions. The myodural bridge mechanism is one of the proposed mechanisms by which cervical structures produce cervicogenic headache, particularly the pain pattern that begins at the base of the skull and spreads forward and upward.
Tension-type headache
Tension-type headache is the most common headache disorder, characterized by bilateral, pressing or tightening, mild-to-moderate pain that is not aggravated by routine physical activity and does not have prominent migrainous features. The myodural bridge mechanism likely contributes substantially to many cases of tension-type headache, given the role of cervical muscle tension in producing the dural mechanical loading. Many patients diagnosed with tension-type headache may have underlying cervical contribution through the myodural bridge mechanism that has not been specifically identified. The overlap between cervicogenic and tension-type headache categories reflects this shared underlying mechanism.
Migraine through cervical interaction
Migraine is fundamentally a disorder of central sensory processing rather than primarily a peripheral mechanism. However, cervical input through the trigeminocervical complex can activate the migraine system in susceptible individuals. Patients with migraine plus persistent cervical involvement may have the myodural bridge mechanism contributing to migraine attack frequency or maintenance, particularly in patients with post-traumatic onset, prominent cervical features, or treatment-resistant patterns. The relationship is more indirect than with cervicogenic or tension-type headache but can still be relevant for appropriate patients.
Post-traumatic headache
Post-traumatic headaches develop after head or neck trauma and often involve mixed mechanisms. The trauma typically produces both upper cervical structural injury (with subsequent occipital muscle tension and myodural bridge effects) and broader effects on the central nervous system. The myodural bridge mechanism contributes to the cervicogenic component of post-traumatic headache, while the central mechanisms contribute to other features. For these patients, addressing the cervical structural component can be a meaningful part of comprehensive post-traumatic headache management.
Headaches the myodural bridge mechanism does not explain
Some headache types are not particularly related to the myodural bridge mechanism. Primary headaches like cluster headache and trigeminal autonomic cephalalgias involve different specific mechanisms. Headaches from intracranial pathology — brain tumors, aneurysms, infections, increased intracranial pressure — require medical evaluation and treatment of the underlying condition. Headaches associated with serious systemic illness require appropriate medical workup. Patients with sudden severe headache (the worst headache of their life), new headache patterns particularly in older adults, headaches with neurological symptoms, or other red flag features need urgent medical evaluation rather than assumption of cervical mechanisms.
Honest Framing of the Evidence
Patients considering upper cervical evaluation for chronic tension-type or cervicogenic headaches should understand the evidence landscape clearly.
What is well-established
The anatomical existence of the myodural bridge is well-established. The Hack 1995 finding has been replicated and expanded by multiple subsequent studies, with the structure consistently identified across populations. The dural sensitivity to mechanical stimulation is well-established mainstream neuroscience. The trigeminocervical complex and its role in headache mechanisms is well-established. The biomechanical reality that upper cervical structural problems produce occipital muscle tension is consistent with broader principles of musculoskeletal compensation. These foundational elements are not controversial.
What this means for patient decisions
Patients with chronic tension-type or cervicogenic headaches considering upper cervical evaluation should understand that the evaluation represents an anatomically-grounded approach to addressing one potential root cause of their headaches. The evaluation may identify structural problems that, when corrected, may reduce the chronic occipital muscle tension that drives the myodural bridge mechanism. Improvement, when it occurs, typically develops gradually over weeks to months. Lack of improvement does not indicate the diagnosis was wrong; it indicates that the cervical structural contribution to this specific patient's headaches was limited.
Multidisciplinary care often helps
Many patients with chronic headaches benefit from multidisciplinary care involving multiple providers addressing different components. Neurology or headache specialist evaluation establishes the diagnosis and oversees overall management. Physical therapy provides structural rehabilitation and exercise components. Stress management and behavioral approaches address psychological factors. Lifestyle and ergonomic modifications address daily contributing factors. Upper cervical evaluation can be one component of this multidisciplinary approach for appropriate patients, addressing the specific structural component that other providers do not target.
How an Upper Cervical Evaluation Works
For appropriate patients with chronic tension-type or cervicogenic headaches, upper cervical chiropractic focuses specifically on the precise structural relationship between the skull, atlas, and axis — the region where the myodural bridge originates.
Three-dimensional CBCT imaging
Cone beam computed tomography produces a true 3D reconstruction of the upper cervical anatomy and measures alignment to within fractions of a degree. The imaging identifies the specific structural problems that may be present, providing objective measurement rather than subjective assessment. For patients with chronic headaches and suspected cervical involvement, the imaging clarifies whether structural problems exist that could be contributing to the symptom pattern.

Objective testing before any intervention
Leg length analysis and paraspinal infrared thermography are performed before any adjustment, and corrections are only delivered when objective findings indicate a structural shift. The principle of restraint guided by data is particularly important for chronic headache patients whose nervous systems are often sensitized from prolonged pain. Interventions are objective-finding-based, not symptom-based alone.
Precision without manipulation
Corrections are specific to the upper cervical segment and delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. For chronic headache patients — whose cervical and central systems are often sensitized — this precision matters. Aggressive cervical manipulation can aggravate sensitized systems and is not appropriate for this population.
Expected response pattern
When upper cervical correction produces benefit for chronic tension-type or cervicogenic headache, the response typically develops gradually. The chronic muscle tension does not resolve immediately after correction — the muscles have adapted to the abnormal pattern over time and require weeks to months to return to normal resting length and tension patterns. As the muscle tension gradually normalizes, the myodural bridge effect reduces, and the dural mechanical loading decreases. The headache pattern often improves correspondingly, with reduced frequency, reduced severity, or both. Individual response patterns vary.
When to Consider an Upper Cervical Evaluation
An upper cervical evaluation may be worth considering for chronic headache patients when any of the following are true:
Your headaches begin at the base of the skull and spread upward and forward. You have chronic tightness or tension at the base of the skull alongside your headaches. You have a clinical diagnosis of cervicogenic headache or tension-type headache that has not responded fully to standard treatment. Your headaches developed after head or neck trauma — concussion, whiplash, sports injury, or fall. You have associated symptoms suggesting cervical involvement — neck pain, restricted cervical range of motion, cervicogenic dizziness, or other features. Your headaches worsen with sustained postures, prolonged computer work, or specific head positions. You have prior concussions or significant neck trauma layered on top of the current presentation. You have migraine alongside prominent cervical features that suggest cervical contribution to the migraine pattern.
Upper cervical evaluation is appropriately complementary to standard headache care, not a replacement for it. Standard treatments including appropriate medications when indicated, stress management, ergonomic improvements, physical therapy, and other components should continue. For patients with headaches responding well to standard treatment, patients with headache patterns clearly explained by other causes, and patients with red flag features requiring urgent medical evaluation, upper cervical chiropractic is not the appropriate first step.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Important Safety Considerations
Several safety considerations apply to patients with chronic headaches considering any care approach including upper cervical evaluation.
Sudden severe headache (the worst headache of your life), new neurological symptoms (vision changes, weakness, numbness, speech difficulties, confusion), severe headache with fever and neck stiffness (potential meningitis), or headaches with associated trauma require urgent medical evaluation rather than chiropractic care. These features can indicate serious underlying conditions requiring immediate medical management.
New headache patterns particularly in older adults, headaches that progressively worsen over weeks to months, headaches that wake patients from sleep, headaches that are worse with cough or straining, or headaches with associated systemic symptoms (weight loss, fever, malaise) require medical evaluation for potential serious causes.
Where to Go From Here
The myodural bridge provides a specific anatomical mechanism by which tension in the deep occipital muscles produces headache through mechanical effects on the dura mater. The structure has been established as consistent anatomy through the 1995 Hack research and subsequent replication studies. The mechanism connects the rectus capitis posterior minor to the spinal dura through continuous connective tissue, with muscle tension transmitting directly to dural tissue and producing pain through the well-established dural sensory innervation. Upper cervical structural problems are one of the most common causes of the chronic occipital muscle tension that drives this mechanism, making structural correction a potential approach to addressing the root cause of certain chronic headache patterns.
For patients with chronic tension-type or cervicogenic headaches who have not responded fully to standard treatment, who have headache patterns matching the myodural bridge mechanism, who have associated cervical features, or who have post-traumatic onset, upper cervical evaluation can be worth considering as a complementary component of comprehensive headache care. The evaluation should be approached alongside continued standard headache management, with realistic expectations about gradual response when improvement occurs. For patients with headaches responding to standard treatment or with red flag features requiring medical evaluation, standard medical care should remain primary.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Mitchell, B. S., Humphreys, B. K., & O'Sullivan, E. (1998). Attachments of the ligamentum nuchae to cervical posterior spinal dura and the lateral part of the occipital bone. Journal of Manipulative and Physiological Therapeutics, 21(3), 145–148.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Goadsby, P. J., Holland, P. R., Martins-Oliveira, M., et al. (2017). Pathophysiology of migraine: A disorder of sensory processing. Physiological Reviews, 97(2), 553–622.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with chronic headaches should pursue appropriate medical evaluation to establish the specific headache diagnosis and rule out serious causes. Standard evidence-based headache treatments should form the foundation of care. Upper cervical evaluation should be considered a complementary approach for appropriate patient subsets rather than a primary treatment for headache disorders. Patients with sudden severe headache, new headache patterns, headaches with neurological symptoms, or other red flag features should seek urgent medical evaluation. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment