
A Chiari malformation diagnosis rests almost entirely on one tool: MRI. There's no blood test, no simple office exam finding that confirms it on its own, and, importantly, imaging position and technique can significantly change what's actually found. This guide walks through exactly what doctors look for on a Chiari MRI, the measurements and terminology you're likely to see on a radiology report, and where an upper cervical evaluation, including imaging most standard workups never order, fits into building a complete picture.
The Core Measurement: Tonsillar Descent Below the Foramen Magnum
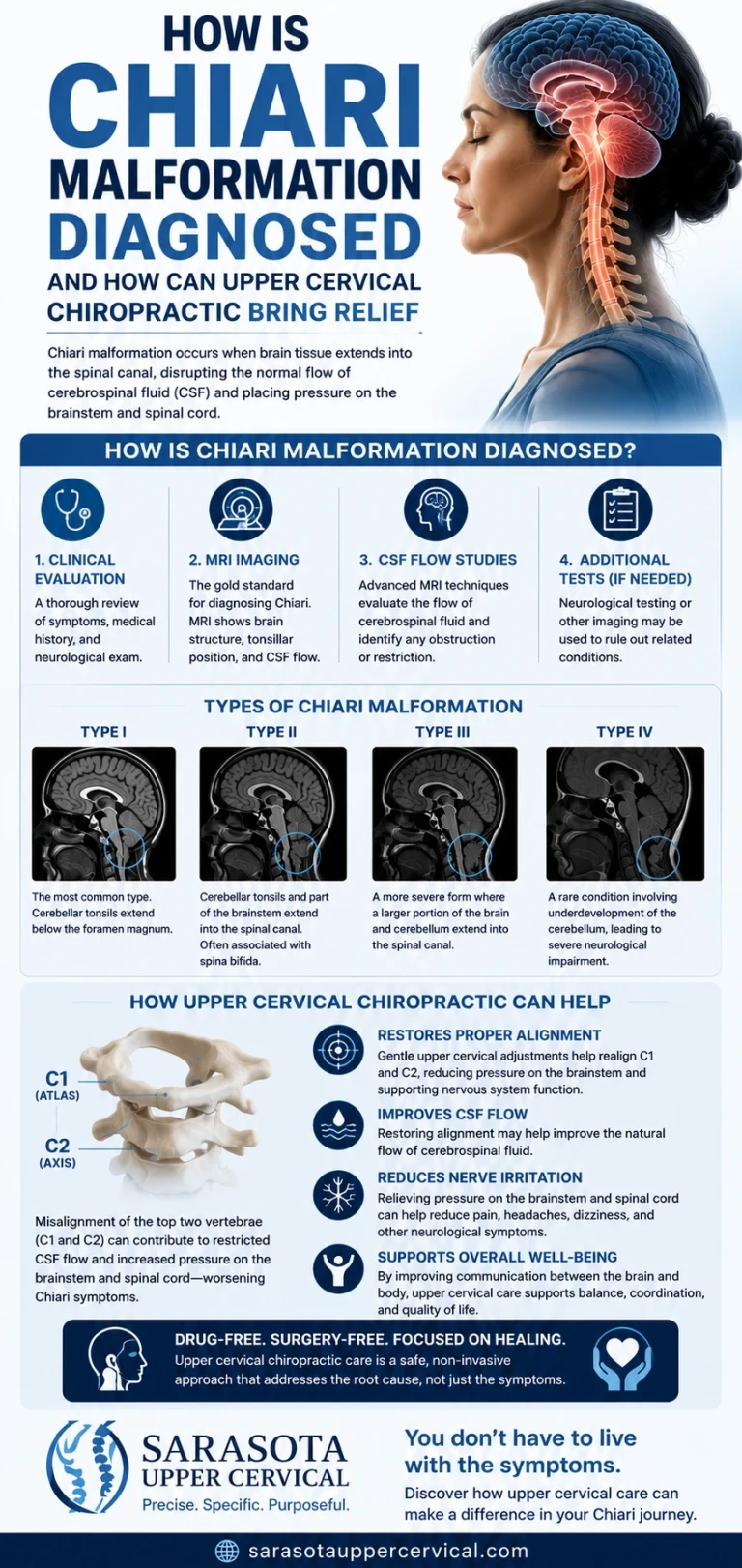
The foramen magnum is the large opening at the base of the skull where the brainstem transitions into the spinal cord. On a midsagittal MRI (a side-view slice through the middle of the brain and upper spine), radiologists measure how far the cerebellar tonsils extend below this opening, typically using a reference line called the McRae line, drawn from the basion to the opisthion, two bony landmarks that define the plane of the foramen magnum.
Schedule Your Appointment
Schedule appointmentThe generally accepted thresholds are:
1. Up to 3 mm below the foramen magnum: considered a normal variant
2. 3 to 5 mm: considered borderline
3.Greater than 5 mm: the standard cutoff for a Chiari type I diagnosis
These thresholds are guidelines, not absolute rules. Radiologists also look for supporting findings that can make a borderline measurement more clinically meaningful, including "peg-like" or pointed tonsils (as opposed to their normal rounded shape), which can appear in both symptomatic and asymptomatic individuals, and a cervicomedullary "kink," a buckling of the brainstem-spinal cord junction seen in a majority of symptomatic patients in some series.
Looking Beyond the Tonsils: CSF Flow and Cine MRI
Measuring tonsillar position alone doesn't tell the whole story, because much of what makes Chiari symptomatic relates to how it disrupts the normal pulsing flow of cerebrospinal fluid (CSF) between the skull and spinal canal. A specialized technique called cine MRI captures this flow in motion, synced to the cardiac cycle, and can reveal obstruction or abnormal flow patterns at the foramen magnum even when tonsillar descent is borderline. This is part of why some patients with a "mild" measurement on a standard MRI report still have significant, demonstrable CSF flow disruption, and why cine MRI is a standard part of a thorough surgical workup when decompression is being considered.

Checking for a Syrinx
Because disrupted CSF flow at the level of the malformation can lead to fluid accumulating inside the spinal cord itself, a full MRI evaluation includes imaging of the entire spinal cord, not just the brain, to check for a syrinx (syringomyelia). A syrinx is a significant finding: it's present in a substantial share of Chiari type I cases, is associated with sensory loss, weakness, and, in children, can contribute to the development of scoliosis, sometimes before any other Chiari symptom appears.
Why Position Matters: The Case for Upright, Weight-Bearing Imaging
Here's a detail that's frequently left out of a standard diagnostic conversation, and it's directly relevant to why some symptomatic patients get told their imaging is "unremarkable." Standard MRI is performed lying down. But the cerebellar tonsils and CSF flow dynamics behave differently once the head is fully weight-bearing, the position your craniocervical junction is actually in most of your waking life.
Research using upright, weight-bearing MRI, work closely associated with imaging researcher Dr. Scott Rosa's studies of the craniocervical junction, has shown that fully visualizing tonsillar ectopia and flow-impeding misalignment often requires imaging in this upright, loaded position, something a standard recumbent scan cannot capture. In practical terms: a Chiari that measures as mild or borderline lying down can look meaningfully different standing up, which may help explain why some patients with significant symptoms are initially told their scan looks unremarkable.
Where the Upper Cervical Spine Enters the Diagnostic Picture
A standard neurological workup for Chiari focuses almost entirely on the posterior fossa, the tonsils, and CSF flow. A thorough upper cervical evaluation adds a distinct, complementary layer: assessing the mechanical state of the craniocervical junction itself.
Cone beam CT (CBCT) and precise atlas positioning
Because the atlas (C1) and axis (C2) sit directly at the junction where Chiari-related crowding occurs, an upper cervical evaluation often includes advanced imaging such as cone beam CT to build a precise three-dimensional picture of how these two vertebrae are actually positioned, information a standard brain MRI is not designed to capture in the same level of biomechanical detail.

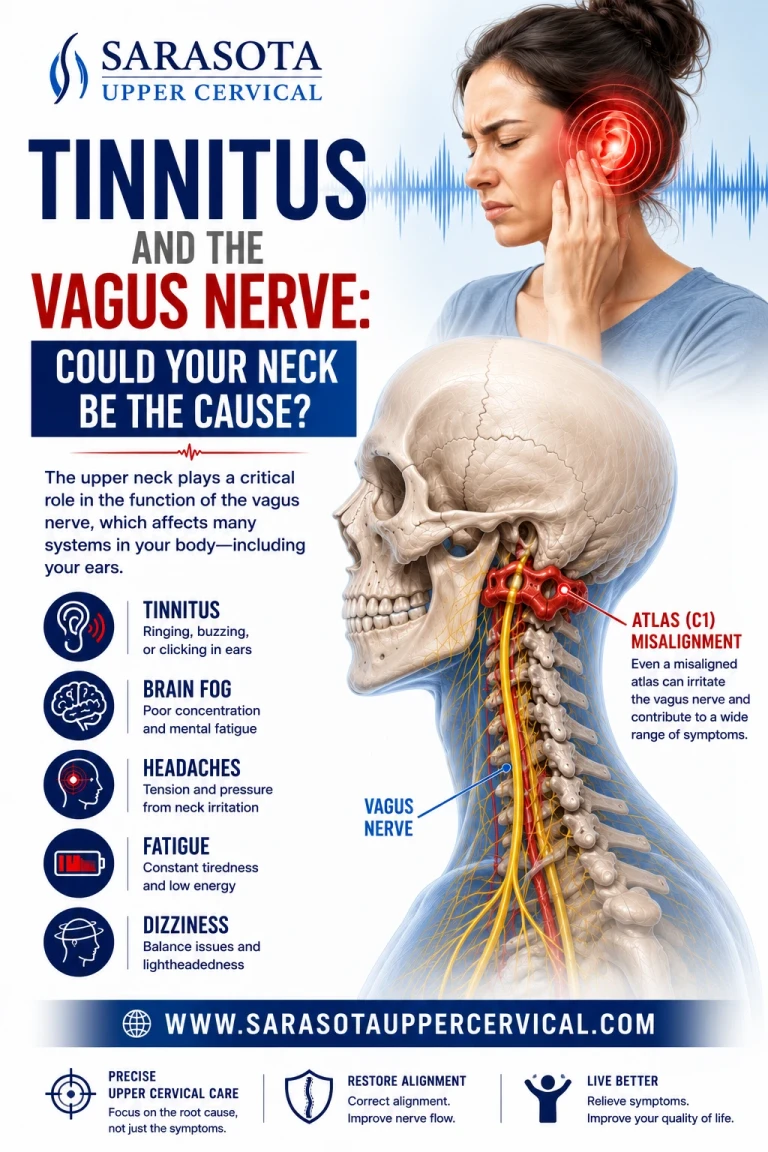
Assessing brainstem irritation from atlas misalignment
Because the atlas surrounds the brainstem and upper spinal cord so closely, its position directly affects the mechanical environment of the entire craniocervical junction. Evaluating this alignment is not a substitute for neurological diagnosis of Chiari itself, but it identifies a separate, addressable variable: whether the mechanical state of the upper neck may be adding irritation on top of the anatomical crowding already present.
The myodural bridge as a diagnostic and mechanistic clue
The rectus capitis posterior minor and its neighboring suboccipital muscles connect directly to the dura mater via the myodural bridge, right at the craniocervical junction. Research has documented degeneration of this muscle specifically in Chiari patients, and whiplash-related damage to it has been associated with a significantly increased likelihood of Chiari-related findings. A history of whiplash or neck trauma, combined with imaging or palpation findings suggesting suboccipital muscle dysfunction, is a meaningful piece of clinical information that a brain-only MRI protocol will not surface on its own.
Cervical curve assessment
Because a flattened or reversed cervical curve (sometimes called straight neck syndrome) lengthens the spinal canal and places the cord under increased longitudinal tension, a lateral cervical spine view assessing the curve is a simple, informative addition to a Chiari workup, particularly for patients whose symptoms began or worsened after a neck injury. This measurement is not part of a standard brain MRI protocol and is easy to miss unless specifically ordered.
Functional and proprioceptive assessment
Because the suboccipital muscles carry an unusually high density of proprioceptive receptors feeding the brainstem's balance centers, a functional evaluation, checking for muscle imbalance, restricted motion, and asymmetric tone around the upper cervical spine, adds information about the sensorimotor side of the picture that structural imaging alone doesn't capture.
Putting a Complete Workup Together
A comprehensive Chiari diagnostic process reasonably includes: standard brain MRI with attention to tonsillar position and the McRae line, cine MRI to assess CSF flow dynamics, full-spine imaging to rule out a syrinx, and, for patients with a relevant trauma history or a discrepancy between symptom severity and standard imaging findings, upright weight-bearing MRI alongside a focused upper cervical evaluation including cervical curve assessment and precise atlas/axis imaging such as CBCT. The first three are standard neurological practice. The last is where many workups stop short, not for lack of supporting research, but because it simply isn't part of the default template most patients are routed through.
What Diagnosis Does Not Mean
To be direct: neither an upper cervical evaluation nor any correction of atlas alignment diagnoses, replaces the diagnosis of, or treats a Chiari malformation. Diagnosis and any decision about surgical management rest with neurology and neurosurgery. What a thorough upper cervical workup contributes is a clearer picture of a separate, genuinely relevant mechanical variable, useful information for understanding symptom severity and, for some patients, for guiding conservative care alongside ongoing medical management.
Questions and Answers
What size of tonsillar descent counts as a Chiari malformation?
Descent greater than 5 millimeters below the foramen magnum on midsagittal MRI is the generally accepted threshold for a Chiari type I diagnosis, with 3 to 5 millimeters considered borderline and up to 3 millimeters considered a normal variant.
Why would a doctor order cine MRI in addition to a standard MRI?
Cine MRI captures the motion of cerebrospinal fluid flow at the foramen magnum, which can reveal significant obstruction even when tonsillar descent measures as mild or borderline on a standard image, making it an important part of a thorough surgical workup.
Why does body position during an MRI matter?
Standard MRI is performed lying down, but the tonsils and CSF flow behave differently under the full weight-bearing load of an upright position. Research using upright, weight-bearing MRI has found that some tonsillar descent and flow obstruction is only fully visible in this loaded position, which may explain why some symptomatic patients are told their recumbent scan looks unremarkable.
Does an upper cervical evaluation replace an MRI or neurological workup?
No. An upper cervical evaluation, including imaging like cone beam CT, adds information about the mechanical state of the atlas, axis, and cervical curve. It does not diagnose Chiari malformation itself and should always be pursued alongside, not instead of, standard neurological evaluation and MRI.
Why would a cervical curve X-ray be relevant to a Chiari workup?
A flattened or reversed cervical curve lengthens the spinal canal and increases longitudinal tension on the spinal cord, a mechanical factor the tethering research suggests can relate to tonsillar position and symptom severity. This measurement isn't part of a standard brain MRI protocol, so it's easy to overlook unless specifically evaluated.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Chiari malformation is a structural neurological condition that must be diagnosed and managed by qualified medical professionals using appropriate neurological imaging and evaluation. Upper cervical chiropractic does not diagnose, treat, correct, or cure Chiari malformation and is intended only to evaluate and address the biomechanics of the craniocervical junction as a complement to medical care. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization is made or implied. The imaging approaches and research described, including upright MRI and craniocervical junction imaging research, represent emerging and in some cases debated areas of science, and are presented for education rather than as proof of diagnostic or treatment outcomes. Always consult your physician, neurologist, or neurosurgeon regarding diagnosis and treatment of Chiari malformation or any neurological symptom



Leave a comment