
"Why sound sensitivity is rarely just an ear problem — and how the upper cervical spine influences the brainstem that decides how loud everything feels"
Hyperacusis is one of the most isolating conditions a person can live with. Normal everyday sounds — dishes clattering, a car door closing, your own children laughing — become physically painful or overwhelming. Quiet environments become essential. Social events become exhausting. Restaurants, grocery stores, and movie theaters become things you plan around or avoid entirely. And the ENT workup, more often than not, comes back largely unremarkable, which is its own kind of frustrating answer.
Schedule Your Appointment
Schedule appointmentWhat is rarely communicated to patients is that hyperacusis is fundamentally a central nervous system condition, not an ear condition. The mechanism has been clearly described in peer-reviewed auditory neuroscience for more than a decade. And once you understand where the problem actually lives — in the auditory brainstem, at the same anatomical level as the top of your neck — the connection to the upper cervical spine becomes a serious clinical question rather than a far-fetched theory.
This article explains what hyperacusis actually is in neurological terms, why the brainstem and the upper cervical spine are so closely connected when it comes to sound processing, and how a precision-based, gentle upper cervical correction may offer a path forward for patients who feel they have run out of options.
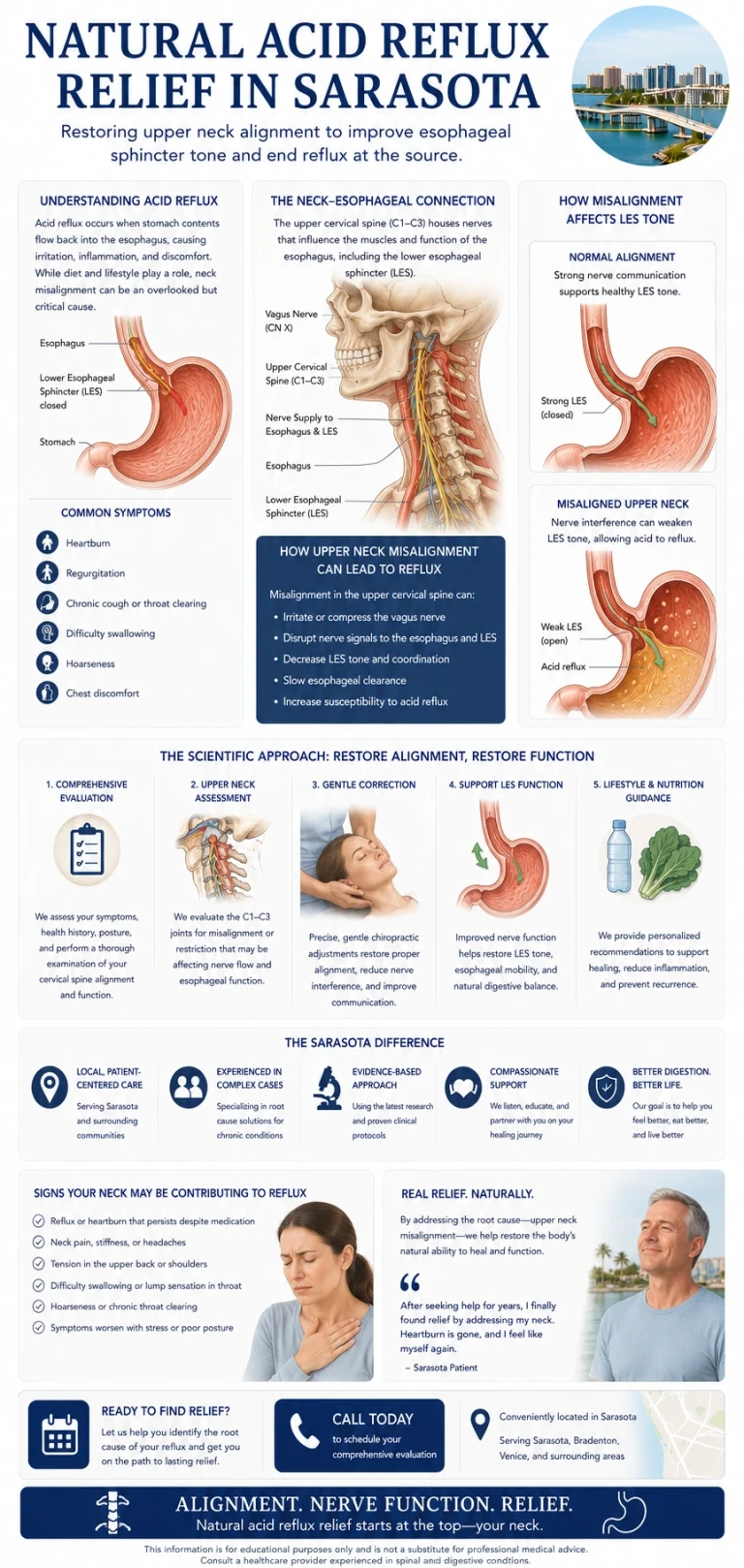
Hyperacusis Is a Brainstem Disorder, Not an Ear Disorder
The starting point for understanding hyperacusis is a concept called central gain enhancement. Auditory neuroscience research has shown that when the brain receives reduced or unstable input from the cochlea — from noise exposure, an injury, illness, or simply chronic stress on the nervous system — it does not just sit there with quieter signals. It compensates. It turns up the volume centrally, by amplifying the neural activity in the brainstem and higher auditory centers.
This compensation is a survival feature. It is the same mechanism that lets you hear a soft conversation in a quiet room. But when the compensation gets stuck in the up position, the result is that ordinary sounds are amplified to the point where they feel uncomfortable, intrusive, or painful. The ears themselves are fine. The volume control in the brainstem is not.
The structures most directly implicated are in the brainstem itself — the cochlear nucleus, the inferior colliculus, and the medial geniculate body, all of which sit at or near the level where the skull meets the upper cervical spine. The dorsal cochlear nucleus in particular has been described in peer-reviewed literature as a critical hub: it is the first synaptic relay in the auditory pathway, it integrates input from the inner ear with input from elsewhere in the body, and it is mandatory for the generation of certain forms of tinnitus and sound intolerance. When this region is hyperactive, the brain experiences ordinary sound as too loud, too sharp, or simply too much.
The Direct Neurological Link Between Your Neck and Your Hearing
Related article
Seeing the Whole Picture: CBCT, the Blair Analysis, and Why Precision Changes Outcomes
Jun 20, 2026
Here is where things get particularly interesting, and where the science directly supports a connection between the upper cervical spine and sound hypersensitivity.
The dorsal cochlear nucleus does not only receive input from the inner ear. It also receives somatosensory input — input from the face, the head, and the neck. This has been documented anatomically through neural tracing studies. Researchers have injected tracers into the cochlear nucleus and retrogradely labeled nerve cells in the dorsal root ganglion at the second cervical level, C2. They have done the reverse experiment, injecting C2 and anterogradely labeling fibers terminating in the cochlear nucleus. The conclusion in the peer-reviewed literature is direct: somatosensory input from the upper cervical spine reaches the auditory brainstem and converges with auditory signals there.
The practical implication is significant. When the upper cervical joints are misaligned or chronically irritated, the somatosensory signal they send into the brainstem is abnormal. That abnormal signal lands in the same anatomical region that is processing every sound you hear. It can excite the auditory brainstem in ways it should not be excited, and in a system that is already running with elevated central gain, this is exactly the kind of input that can sustain or worsen hyperacusis.
This is not theoretical. Auditory neuroscience literature has demonstrated that electrical stimulation of cervical nerves or voluntary head and neck movements can alter dorsal cochlear nucleus activity — and that up to roughly 80 percent of people with certain forms of tinnitus or sound intolerance can modulate their symptoms by changing the position or activity of their neck. The same input pathway that can worsen symptoms can, in principle, also normalize them when the source of irritation is removed.
Why a Misaligned Upper Cervical Spine Can Irritate the Brainstem
The brainstem sits at the level of the craniocervical junction, the area where the skull meets the atlas (C1) and axis (C2). Almost everything the brain depends on physically passes through this region — the brainstem itself, the vertebral arteries supplying it with blood, the internal jugular veins draining blood out of the skull, the cerebrospinal fluid channels, and several cranial nerves including the vestibulocochlear nerve that carries hearing information from the inner ear.
When the upper cervical spine is misaligned, several things can happen at once. The mechanoreceptor input from the joints becomes distorted. The local environment around the brainstem and surrounding nerves can be placed under mechanical stress. Cerebrospinal fluid flow and venous drainage can be subtly impaired, affecting the pressure environment around the brainstem. And the dense connective tissue that anchors the spinal cord to the dura mater — the denticulate ligaments — can transmit tensile stress directly up into the brainstem itself.
Any one of these factors can contribute to brainstem irritation. Taken together, they describe a chronically over-stimulated, under-resourced brainstem trying to do all of its many jobs — including the careful regulation of auditory gain — in a less than optimal mechanical environment. For a patient with hyperacusis, this is not an academic concern. It is the difference between living comfortably in the world and avoiding it.
The Pattern Many Hyperacusis Patients Share
Related article
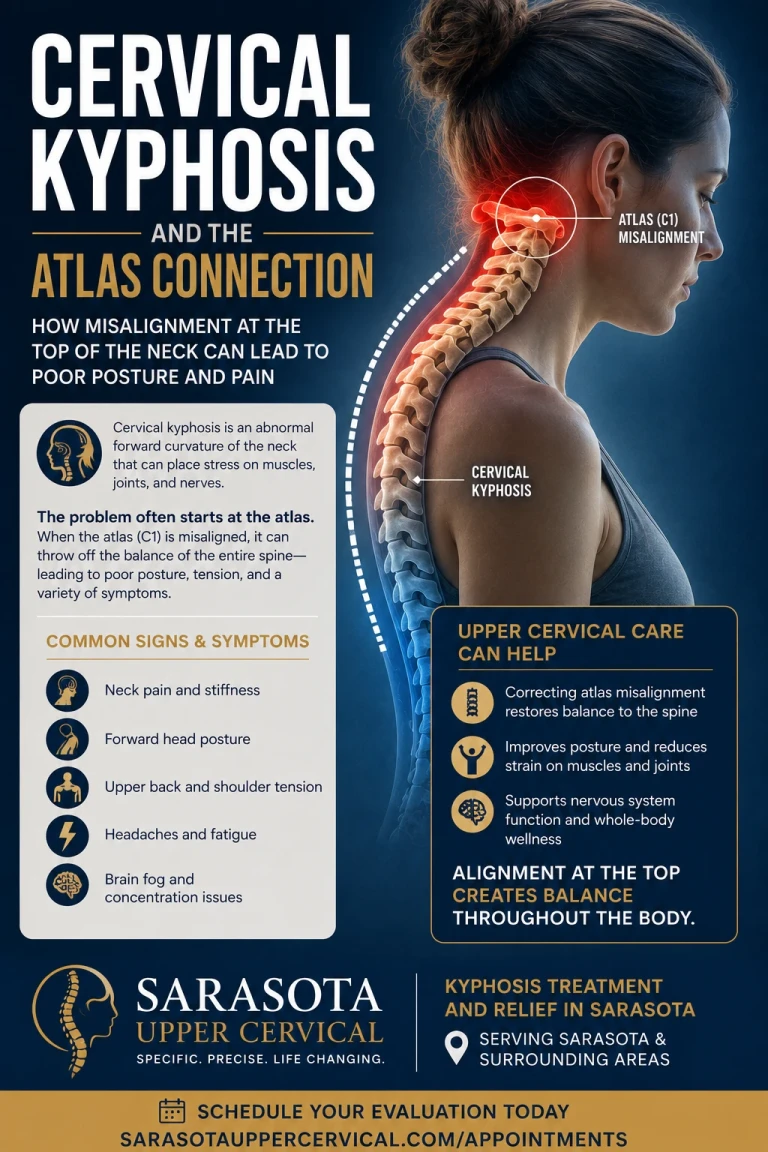
Cervical kyphosis and the atlas connection | Kyphosis treatment and relief sarasota
Jun 28, 2026
The patient we see most often in this category has a story that sounds familiar. Sound sensitivity that began or significantly worsened after a specific event — a concussion, a car accident, a fall, a viral illness, a particularly loud noise exposure, or sometimes a period of intense stress. An ENT workup that ruled out the obvious causes but did not resolve the symptoms. Sometimes a course of sound therapy. Sometimes a recommendation to simply avoid triggering environments.
Common features include sound sensitivity that worsens with neck strain or specific head positions, neck stiffness or pain that the patient may not have connected to the auditory symptoms, a history of head or neck trauma, frequent co-occurring symptoms like tinnitus, fullness in the ears, dizziness, or migraine, and a sense that the sensitivity is worse on bad days — when sleep, stress, or fatigue are working against you. None of these features are diagnostic on their own, but together they raise the question of whether the upper cervical spine is part of what is driving the central gain that is making everyday sound unbearable.
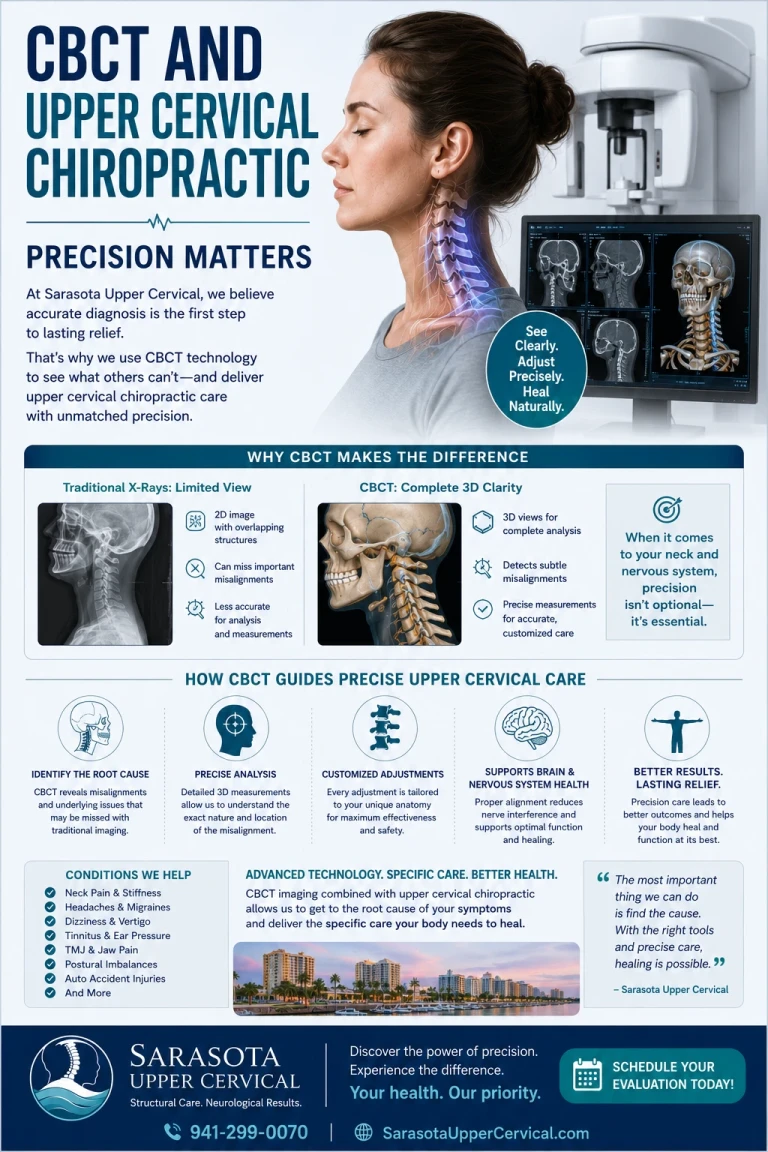
CBCT Imaging: Precision Before Anything Else
Before any care begins in our Sarasota office, we use Cone Beam Computed Tomography (CBCT) imaging of the upper cervical spine. CBCT is a precision imaging tool that produces three-dimensional views of the skull base, atlas, axis, and surrounding structures — detail that flat two-dimensional X-rays cannot provide.
Every craniocervical junction is built differently. The angles, the orientations, and the relationships between the skull, C1, and C2 are unique to each person. Without precision measurements, an upper cervical correction is a guess. With them, the correction can be specific, gentle, and matched to your exact anatomy. For a patient whose ENT workup has ruled out the inner ear but who is still searching for an explanation, this is often the first time the structure most likely to be influencing the auditory brainstem is being looked at directly.
No Twisting. No Cracking. No Pulling of the Neck
Most people picture a chiropractic adjustment as a fast head-turn and a popping sound. That is not what we do. The correction we deliver is specific, low-force, and based directly on the measurements taken from your CBCT scan. There is no twisting, cranking, or pulling. No cavitation noise. You lie on your side with your head supported. The correction takes seconds.
For a patient with hyperacusis, this matters a great deal. A nervous system that is amplifying everyday sound is a nervous system already running hot. The last thing it needs is a forceful manipulation that adds more stimulus to a system already overwhelmed. Our approach is built specifically to avoid that — to give the brainstem cleaner input from the upper cervical joints without adding stress to a system that is already in a heightened state of alert.
Gentle does not mean ineffective. Gentle means we are working with the nervous system, not against it. The goal is to restore mechanical and neurological balance at the craniocervical junction so the auditory brainstem can return to a more normal level of gain — and so ordinary sound can stop feeling like an attack.

A Realistic First Visit, and a Realistic Conversation
A first visit in our Sarasota office includes a thorough consultation, a focused examination, and CBCT imaging of the upper cervical spine. We pay particular attention to your full history — including any head or neck trauma, even decades old, because those events are often where the auditory hypersensitivity story actually begins. After we review the imaging with you, we will tell you honestly whether upper cervical care looks like a good fit. If it is, we build a plan. If it is not, we say so and point you toward what is more likely to help.
Hyperacusis is a complex condition, and a single approach is rarely the whole answer. Upper cervical chiropractic does not replace appropriate audiological care, sound therapy, or psychological support where those are needed. What it can offer is a piece that often goes missing — a serious look at the structural and neurological foundation underneath the auditory system that is producing the symptoms.
If You’re Living With Hyperacusis in Sarasota
Sound hypersensitivity does not have to be a permanent condition you arrange your life around. The neurology of hyperacusis is increasingly well understood, the connection between the upper cervical spine and the auditory brainstem is anatomically documented, and the approach to addressing it can be specific, precise, and gentle. None of that is a cure. All of it represents a real, structural piece of the puzzle that most workups simply do not include.
If you are searching for hyperacusis treatment and relief in Sarasota and you want to understand whether the upper cervical spine might be part of your picture, the next step is a conversation. We will go through your history, image your craniocervical junction, and give you a straight answer about whether this approach makes sense for you.
Ready to take the next step? Schedule a consultation at our Sarasota office to start with a complete upper cervical evaluation and CBCT imaging.
References:
Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol. 2014;5:206. • Zhan X, Pongstaporn T, Ryugo DK. Projections of the second cervical dorsal root ganglion to the cochlear nucleus in rats. J Comp Neurol. 2006;496(3):335-348. • Shore SE. Multisensory integration in the dorsal cochlear nucleus: unit responses to acoustic and trigeminal ganglion stimulation. Eur J Neurosci. 2005;21(12):3334-3348. • Pfaller K, Arvidsson J. Central distribution of trigeminal and upper cervical primary afferents in the rat studied by anterograde transport of horseradish peroxidase conjugated to wheat germ agglutinin. J Comp Neurol. 1988;268(1):91-108. • Manohar S, et al. Dorsal cochlear nucleus responses to somatosensory stimulation are enhanced after noise-induced hearing loss. Eur J Neurosci. 2008.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Hyperacusis and other auditory disorders should be evaluated by a qualified audiologist or ENT specialist to rule out serious causes. Upper cervical chiropractic care does not diagnose, treat, or cure hyperacusis, tinnitus, or any other auditory disorder. Individual results vary.



Leave a comment