
"Flying produces some of the most challenging pressure conditions the Eustachian tube must manage. For patients with underlying ETD susceptibility, ascent and descent reveal a problem that may operate more subtly in daily life. Understanding why flying triggers symptoms clarifies what may be affecting your ears year-round"
Many patients in Sarasota know the experience well. The descent into Sarasota-Bradenton International or Tampa International begins, and somewhere over the Gulf of Mexico the ears start to feel pressure. Swallowing helps a little. Yawning helps a little. By the time the plane is on final approach, one ear or both ears feel completely blocked. The ears do not pop. The hearing is muffled for the rest of the day. Sometimes there is sharp pain that develops in the last few minutes of descent and persists for hours afterward. Sometimes there is dizziness during landing or in the hours after the flight. Some patients have had episodes severe enough that they avoid flying entirely — a substantial limitation for Florida residents, snowbird families, and anyone whose work or family life requires travel. In this article we will discuss why this occurs and how the upper cervical spine can be a constributing factor to this occurence and how it can help resolve the condition.
Schedule Your Appointment
Schedule appointmentTo schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
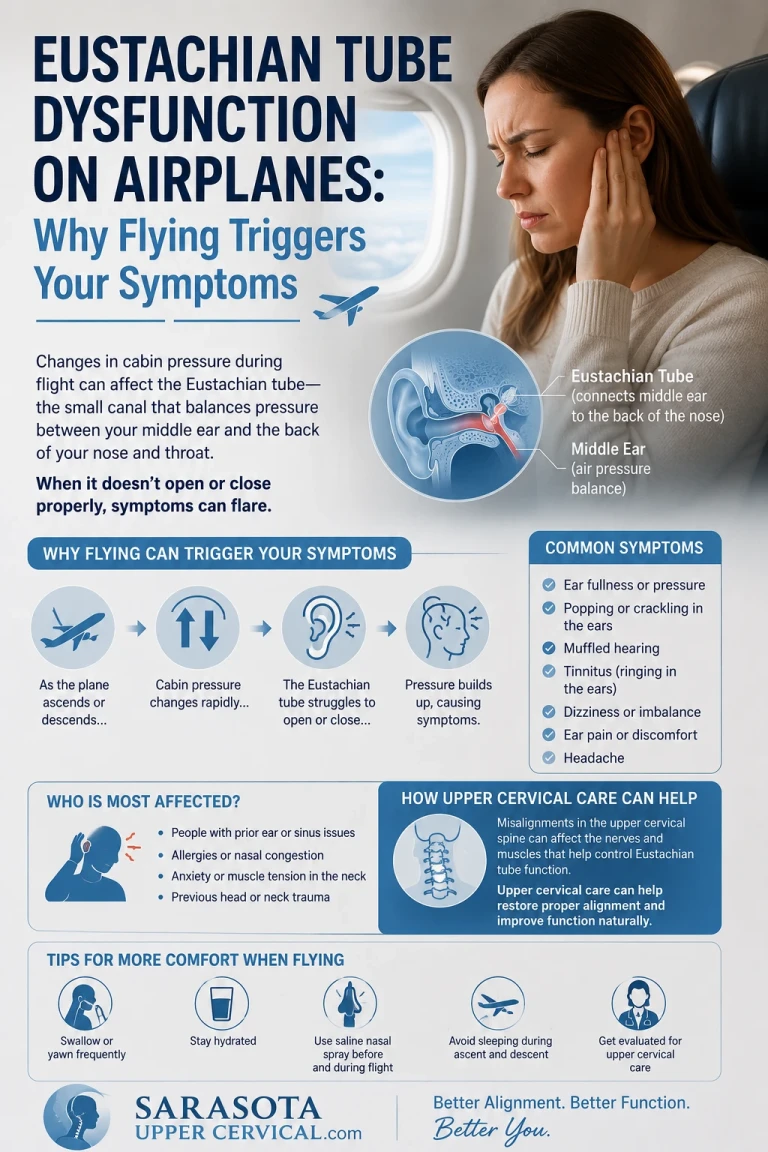
This pattern — symptoms predictably worse with flying, sometimes severe, often persisting after landing — reflects underlying Eustachian tube dysfunction (ETD) being revealed by the pressure challenges that flying presents. The Eustachian tube must equalize pressure between the middle ear and the surrounding atmosphere whenever ambient pressure changes. During flight, pressure changes are rapid and substantial — different from the slower barometric pressure changes from weather. The tube must open repeatedly and adequately to keep up. For a patient with healthy ETD function, this happens automatically and produces only the brief pressure sensation of normal flight. For a patient with underlying ETD susceptibility, the system cannot keep up with the demand, and symptoms develop.
What patients often miss is that ETD on airplanes is rarely just about the plane. Flying acts as a stress test for the Eustachian tube system. Patients who reliably struggle with flying typically have underlying ETD problems that operate more subtly in daily life — occasional ear pressure with weather changes, fullness with sinus issues, muffled hearing that comes and goes, or symptoms patients have come to consider normal. The flight produces an acute version of what the system is already struggling with at baseline. Understanding what flying reveals about your Eustachian tube function clarifies whether comprehensive evaluation may be warranted to address the underlying picture.
This article walks through what actually happens to the Eustachian tube during flight, the specific mechanism of ETD on airplanes, why some patients have severe problems while others fly without issue, the connection to underlying chronic ETD susceptibility, how upper cervical structural factors may contribute to the underlying picture, and where comprehensive evaluation at Sarasota Upper Cervical may have relevance for patients whose flying problems point to deeper ETD issues affecting their daily life.
What Happens to the Eustachian Tube During Flight
Understanding why flying produces ETD symptoms requires understanding the pressure changes the Eustachian tube must manage during a normal flight.
Cabin pressure changes during flight
Commercial aircraft pressurize their cabins to simulate altitudes between 6,000 and 8,000 feet, even when flying at 35,000 feet or higher. This means that during a typical flight, cabin pressure decreases from ground-level pressure to the equivalent of 6,000-8,000 feet during climb, then increases back to ground-level pressure during descent. The pressure change happens over minutes — substantial pressure changes occurring in compressed time. For comparison, the barometric pressure changes from weather systems typically occur over hours or days, allowing the body more time to adapt. The flight pressure changes are rapid, large, and bidirectional within a few hours.
What the middle ear must do
The middle ear is an enclosed air-filled space behind the eardrum. When ambient pressure changes, the middle ear pressure must change to match — otherwise pressure differentials across the eardrum produce symptoms. The Eustachian tube is the only pathway for air to move between the middle ear and the atmosphere. When functioning normally, the Eustachian tube opens periodically (typically with swallowing, yawning, or jaw movement) to allow brief air exchange that equalizes middle ear pressure with current ambient pressure.
Ascent: passive pressure relief
During ascent, cabin pressure decreases. This means middle ear pressure becomes higher than ambient pressure. The pressure differential pushes the eardrum slightly outward and creates a passive pressure that helps force the Eustachian tube open. Air can escape from the middle ear through the tube relatively easily because the pressure is pushing in the direction of tube opening. Most patients experience ascent as relatively easy from an ear perspective — the ears may pop or feel briefly full, but resolution happens automatically.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Related article
Descent: active opening required
Descent is the more challenging phase. As cabin pressure increases during descent, ambient pressure becomes higher than middle ear pressure. The pressure differential now pushes the eardrum inward and pushes the Eustachian tube closed. To equalize pressure, the tube must be actively opened by the muscles that control it — the tensor veli palatini and the levator veli palatini. Passive equalization is essentially impossible during descent; the muscles must open the tube against the closing pressure. This is why ETD problems primarily occur during descent rather than ascent. Patients who experience symptoms typically describe them developing in the last 20-30 minutes of flight as the aircraft descends through the lower atmosphere where pressure changes are most rapid.
The repeated demand
Beyond the overall pressure change of ascent and descent, the Eustachian tube must open and close many times during these phases to keep up with the continuous pressure changes. The tube cannot open once and stay open — it opens briefly and closes between openings to maintain its normal function. During descent, the tube may need to open dozens or hundreds of times to keep up with the pressure demands. A system that opens adequately some of the time but not consistently cannot keep up with the cumulative demand. The result is pressure trapped in the middle ear that progressively worsens through descent.
The Specific Mechanism of ETD on Flights
When the Eustachian tube cannot keep up with the pressure demands of descent, specific events unfold that produce the symptoms patients experience.
Pressure differential develops
When the Eustachian tube fails to open adequately during descent, ambient pressure becomes progressively higher than middle ear pressure. The pressure differential across the eardrum increases. Initial small differentials produce only mild fullness sensation. As the differential grows, the eardrum is pushed progressively inward, producing increasing pressure sensation, then discomfort, then pain. The fluid normally present in middle ear tissues can be drawn into the middle ear space, producing the fluid-filled middle ear pattern.
The barotrauma spectrum
Failure of pressure equalization produces what is called otitic barotrauma — pressure-induced injury to the middle ear. The 2017 review by Stangerup and colleagues classified barotrauma severity from mild (transient symptoms resolving quickly) through moderate (persistent symptoms with eardrum changes) to severe (hemorrhage into the middle ear, eardrum rupture). The 2005 paper by Mirza and Richardson in Clinical Otolaryngology documented otic barotrauma patterns in patients with ETD susceptibility (Mirza & Richardson, 2005). Most patients have mild to moderate barotrauma with resolution over hours to days; severe barotrauma is rare but possible in patients with substantial ETD problems.
Why symptoms can persist after landing
When middle ear pressure equalization has not occurred during flight, the pressure differential does not magically resolve when the plane lands. The Eustachian tube must still equalize the pressure, and if its function is impaired, equalization may take hours or days. Patients describe ears that remain blocked for the rest of the day, hearing changes that persist into the next day, sometimes pain that lingers, and fullness that takes days to fully resolve. The lingering symptoms reflect the pressure differential still being resolved gradually rather than acute new pathology developing after landing.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Why some flights are worse than others
Several factors affect how challenging a given flight will be. Steep descents produce more rapid pressure changes than gradual descents. Smaller aircraft typically descend more rapidly than larger aircraft. Bad weather requiring rapid altitude changes adds challenge. Flying with active congestion (cold, allergies, sinus issues) makes the Eustachian tube less responsive. Long flights at altitude may allow more middle ear adaptation than short flights with rapid up-and-down patterns. Same patient, different flights, can produce different severity of symptoms based on these variables.
Why Some Patients Struggle While Others Fly Without Issue
Most people fly without significant ETD symptoms. The patients who struggle have underlying factors that compromise their Eustachian tube function. Understanding these factors clarifies what's actually being revealed by problematic flights.
Underlying chronic ETD susceptibility
Patients who consistently struggle with flying typically have underlying chronic ETD susceptibility. The susceptibility may be subtle in daily life — occasional ear pressure, mild symptoms with weather changes, fullness that comes and goes — but it becomes apparent under the acute stress test of flight. The flight does not cause the ETD; it reveals the ETD that was already present. This is why patients with frequent flying problems benefit from comprehensive evaluation of their baseline Eustachian tube function rather than just management strategies for the flight itself.
Muscular dysfunction of the Eustachian tube
The Eustachian tube is opened by two main muscles. The tensor veli palatini is the primary opener — its contraction during swallowing pulls the cartilaginous portion of the tube open. The levator veli palatini provides additional support. Both muscles can be affected by various factors that impair their function. When these muscles do not contract effectively or do not coordinate their action well, the tube does not open adequately on demand. The flight situation requires repeated rapid effective opening; impaired muscular function makes this demand impossible to meet.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Related article
trigeminal neuralgia and the neck connection | Trigeminal neuralgia treatment and relief sarasota
Jun 22, 2026The trigeminal nerve and tensor veli palatini control
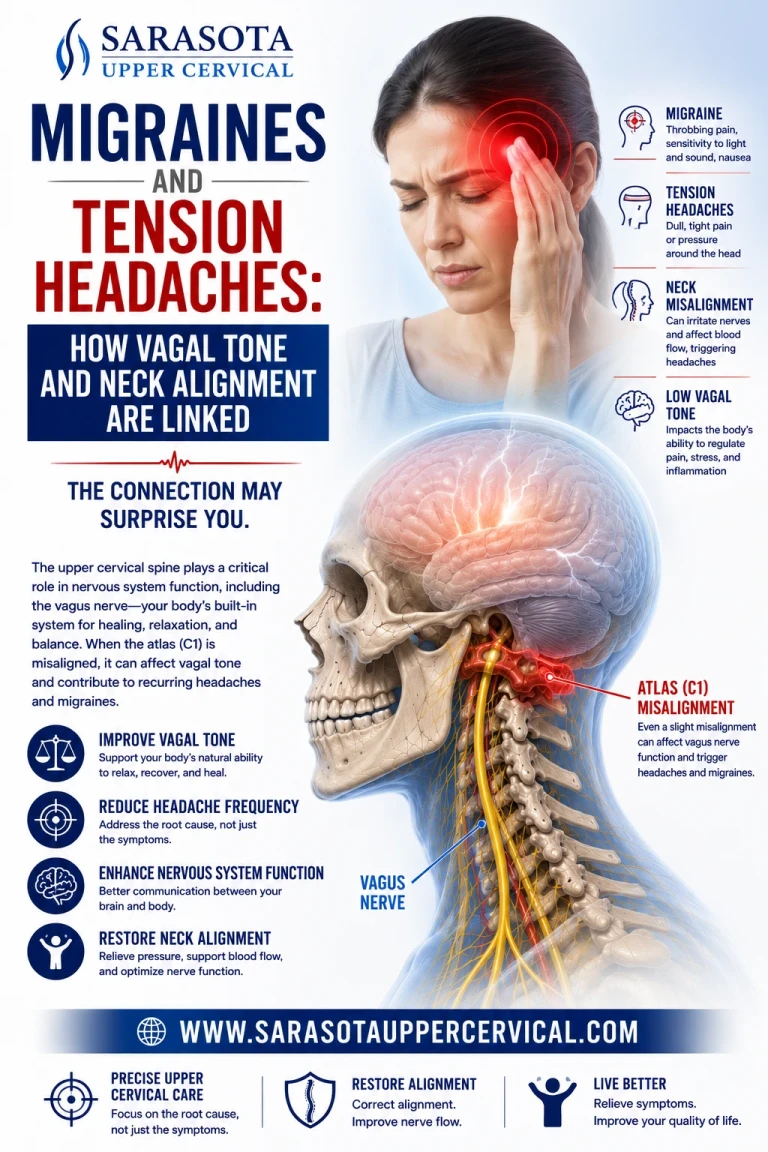
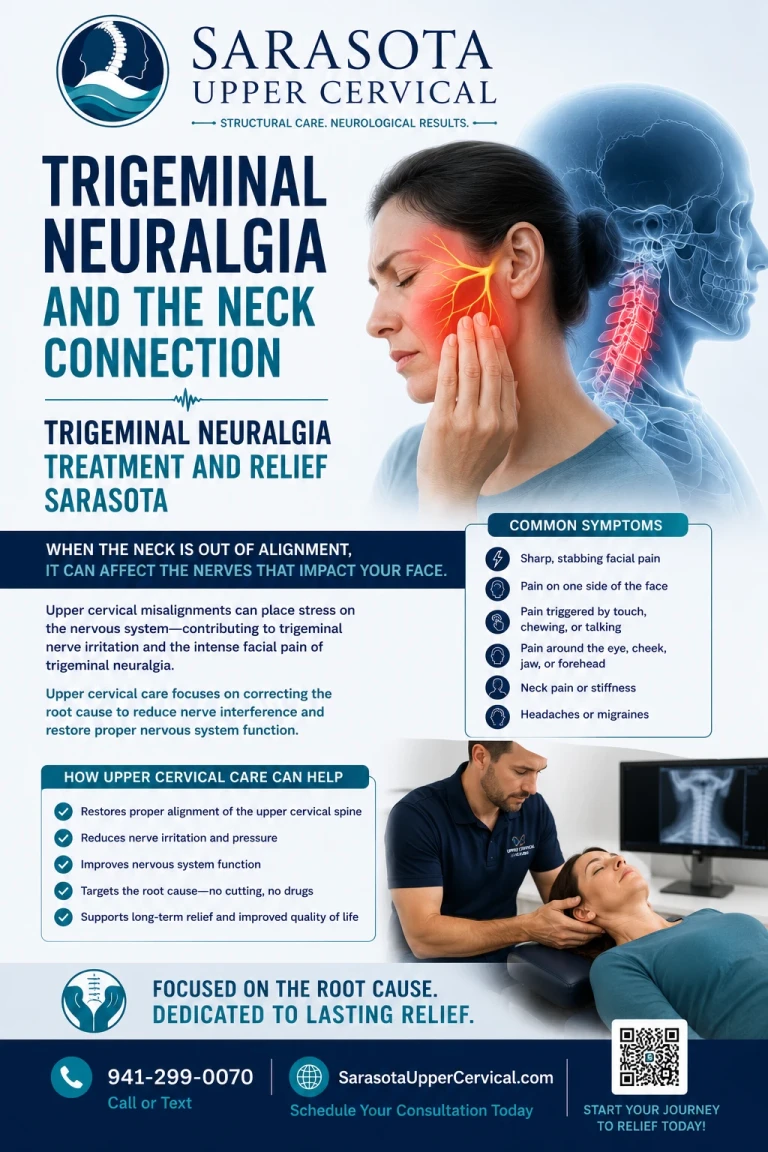
The tensor veli palatini is innervated by the mandibular branch (V3) of the trigeminal nerve. The trigeminal nuclei are located in the brainstem, with the trigeminal system having extensive connections to upper cervical structures through the trigeminocervical complex. The 2003 paper by Bartsch and Goadsby in Current Pain and Headache Reports established this anatomical convergence (Bartsch & Goadsby, 2003). Problems affecting trigeminal function or its central connections can affect tensor veli palatini function and therefore Eustachian tube opening. This neural pathway connection means that structural problems affecting the trigeminocervical region may indirectly affect Eustachian tube muscular control.
Anatomical narrowing or variation
Some patients have anatomically narrower Eustachian tubes that are more susceptible to dysfunction. Congenital variations in tube length, angle, or width affect baseline susceptibility. Anatomical features that work adequately under normal conditions may become inadequate under the acute pressure demands of flight. Most patients don't know their specific anatomical features — they only know they have problems flying. Imaging and evaluation can identify some of these factors.
Inflammation and mucosal factors
Inflammation in the upper airway affects Eustachian tube function. Active allergies, chronic sinus inflammation, recent upper respiratory infections, and various other inflammatory conditions can affect the tube's mucosal lining and the surrounding tissues. The inflammation may produce minimal daily symptoms but compromises the tube's ability to function under acute stress. Flying when actively congested is much harder than flying when clear. Chronic low-grade inflammation creates ongoing susceptibility.
Postural and structural factors
The Eustachian tube anatomy is affected by the position and structural relationships of surrounding tissues. Postural problems affecting the head and neck position may affect tube function. Craniocervical structural problems may affect the anatomy of structures that surround and influence the Eustachian tube. These postural and structural factors may compromise baseline tube function in ways that become apparent only under acute demand.
The Upper Cervical Connection to Underlying ETD Susceptibility
For patients whose flying problems point to underlying chronic ETD susceptibility, the upper cervical structural picture may be one of multiple factors contributing to the susceptibility. Understanding the cervical contribution clarifies where comprehensive evaluation may have relevance.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The neural control pathway
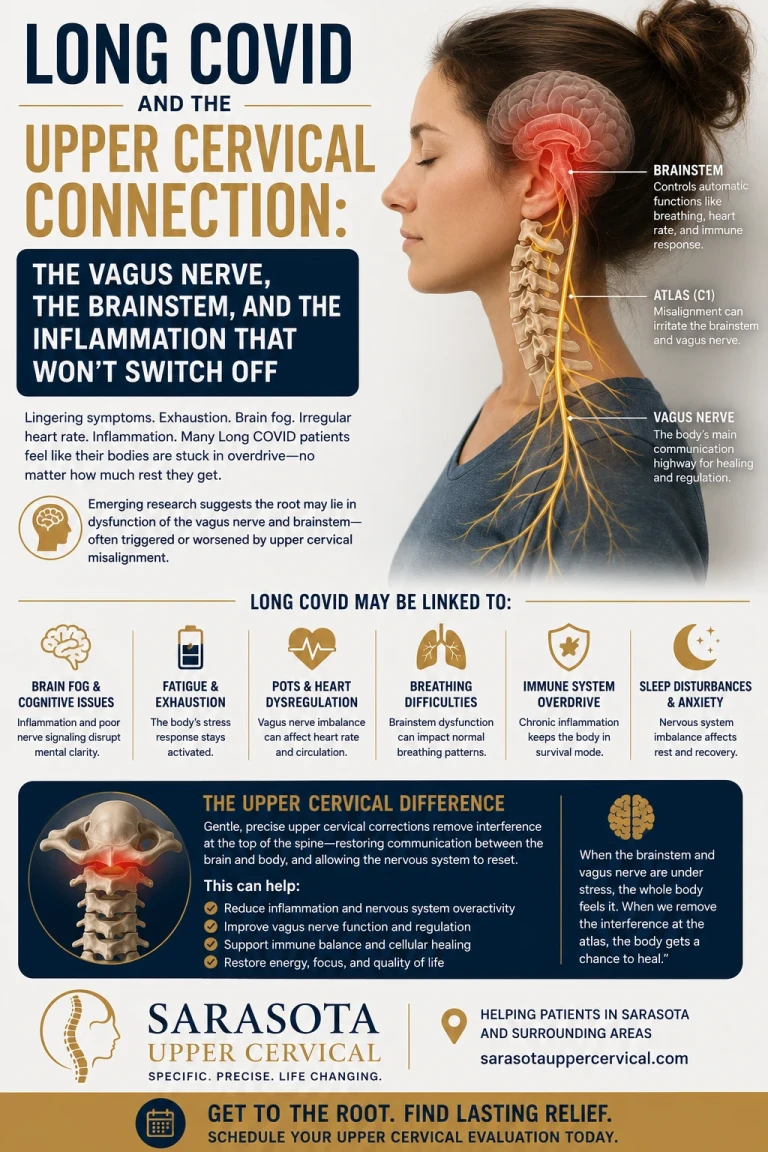
The muscles that open the Eustachian tube are controlled by neural pathways that include the trigeminal nerve (tensor veli palatini via V3) and the pharyngeal plexus (levator veli palatini). The brainstem nuclei controlling these pathways are anatomically close to the upper cervical structures and integrate input from cervical proprioceptive sources. The 2000 study by Gdowski and McCrea documented direct cervical proprioceptive input to brainstem neurons in vestibular regions (Gdowski & McCrea, 2000). Similar cervical input affects other brainstem nuclei. Upper cervical structural problems producing distorted proprioceptive input may affect the broader brainstem environment in which Eustachian tube control occurs.
The fascial and muscular continuity
The Eustachian tube does not exist in isolation. It runs through anatomical regions that are connected to upper cervical structures through fascial and muscular continuities. Tensor veli palatini, palatine muscles, pharyngeal muscles, and surrounding deep neck musculature have fascial relationships with structures of the cervical region. Craniocervical structural problems producing compensatory tension in deep cervical and suboccipital muscles may have effects through these continuities that affect the broader anatomical environment of the Eustachian tube.
The cervical sympathetic chain and vascular regulation
The cervical sympathetic chain along the cervical spine, with the superior cervical ganglion located near the upper cervical region, controls sympathetic innervation to various structures in the head and neck. The mucosa lining the Eustachian tube receives sympathetic innervation that affects its tone, mucus production, and inflammatory response. Cervical sympathetic chain function affected by upper cervical structural problems may contribute to the chronic low-grade inflammation and mucosal factors that compromise Eustachian tube function.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The dural environment and broader head function
The 1995 paper by Hack and colleagues in Spine documented direct connective tissue continuity between the rectus capitis posterior minor muscle and the spinal dura mater (Hack et al., 1995). Chronic compensatory tension in suboccipital muscles transmits mechanical force directly to the dura. The dural environment around the brainstem and the broader mechanical environment of the head can be affected by these chronic structural problems. While the specific effect on Eustachian tube function is theoretical rather than established, the broader principle that craniocervical structural problems affect adjacent anatomical regions provides a framework for understanding potential cervical contributions to ETD.
Why this matters for flying
If upper cervical structural factors are contributing to chronic baseline ETD susceptibility, they are part of what flying reveals as a problem. The flight does not cause cervical issues; it stresses a system that may already be compromised by them. Addressing the cervical contribution to baseline ETD susceptibility may improve the system's ability to handle the acute demands that flying presents. The flying problems become the visible expression of an underlying picture that improvement in baseline function may help.
When to Consider Comprehensive Evaluation at Sarasota Upper Cervical
For patients whose flying problems point to underlying chronic ETD, comprehensive evaluation including upper cervical assessment may be worth considering when:
Your flying problems have worsened over time or have not resolved with standard management strategies. You have other ETD symptoms in daily life — pressure that comes and goes, fullness with weather changes, muffled hearing, occasional dizziness. You have associated cervical features — chronic neck pain, suboccipital tension, restricted range of motion, cervicogenic headache. Your ETD developed or worsened after head or neck trauma — concussion, whiplash, sports injury. You have other conditions that may share cervical structural contributions — tinnitus, vestibular symptoms, TMJ dysfunction, chronic sinus issues. You have tried standard ETD management without adequate improvement.
For patients with isolated flying problems without other ETD features, without cervical symptoms, and without other suggestive features, the case for comprehensive cervical evaluation is weaker. Standard ETD management and ENT follow-up may be sufficient. The cervical evaluation framework applies most clearly to patients whose flying problems are part of a broader ETD picture suggesting underlying chronic susceptibility.
Sarasota Upper Cervical provides three-dimensional CBCT imaging and objective testing to evaluate the upper cervical structural picture. The evaluation identifies whether structural factors may be contributing to chronic ETD susceptibility. Precision-based corrections, when appropriate, address the structural component as part of comprehensive care. To schedule an evaluation, call 941-259-1891.
Important Safety Considerations
Several safety considerations apply to patients with ETD problems on flights.
Severe ear pain during flight that does not resolve, hearing loss that persists more than a few days after landing, vertigo with sudden onset, or any new neurological symptoms warrant medical evaluation. While most flying-related ETD resolves over days, occasional cases involve more significant barotrauma requiring evaluation. ENT evaluation is appropriate for any concerning persistence.
Patients with active ear infections, recent ear surgery, or specific middle ear conditions should consult their physicians before flying. Some conditions are contraindications to flight or require specific precautions.
Patients with significant ETD problems who must fly should consider their options including pre-flight medical consultation, optimal medication timing, equalization techniques, pressure-regulating earplugs, and flight selection (avoiding short flights with rapid altitude changes when possible).
Where to Go From Here
At Sarasota Upper Cervical, we evaluate the craniocervical structural component that may be contributing to chronic ETD susceptibility in appropriate patient subsets. Our approach uses three-dimensional CBCT imaging and objective testing to identify whether structural factors are present, with precision-based corrections when indicated. We work alongside ENT care and other medical management rather than replacing them, addressing one specific component of the broader picture. For patients whose flying problems are part of a larger ETD picture affecting their daily life, comprehensive evaluation may provide a path to better baseline function.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Bluestone, C. D. (2005). Eustachian Tube: Structure, Function, Role in Otitis Media. PMPH-USA.
Stangerup, S. E., Klokker, M., Vesterhauge, S., Jayaraj, S., Rea, P., & Harcourt, J. (2017). Point prevalence of barotitis and its prevention and treatment with nasal balloon inflation: A prospective, controlled study. Otology & Neurotology, 38(1), 33–38.
Mirza, S., & Richardson, H. (2005). Otic barotrauma from air travel. Journal of Laryngology & Otology, 119(5), 366–370.
Norris, R. L. (2013). Travel medicine: Diving, flying, and otitis. Emergency Medicine Clinics of North America, 31(1), 169–186.
Wright, T. (2015). Eustachian tube dysfunction. BMJ Clinical Evidence, 2015, 0510.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Gdowski, G. T., & McCrea, R. A. (2000). Neck proprioceptive inputs to primate vestibular nucleus neurons. Experimental Brain Research, 135(4), 511–526.
Schilder, A. G., Bhutta, M. F., Butler, C. C., Holy, C., Levine, L. H., Kvaerner, K. J., Norman, G., Pennings, R. J., Poe, D., Silvola, J. T., Sudhoff, H., & Lund, V. J. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with persistent ETD or significant flying-related symptoms should pursue appropriate medical evaluation by ENT or otolaryngology specialists. Standard evidence-based ETD management should form the foundation of care. Upper cervical evaluation should be considered as a complementary approach for appropriate patient subsets rather than a primary treatment. Patients with severe ear pain, persistent hearing loss, sudden vertigo, or other concerning symptoms should seek prompt medical evaluation. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment