
"Cervicogenic headache is a specific type of head pain that originates from structures in the neck. Understanding what defines this condition, how it differs from other headache types, and where upper cervical care fits into comprehensive treatment helps Sarasota patients find the right path to relief"
Many headache patients experience pain patterns that don't quite fit the typical migraine or tension headache descriptions. The pain often begins in the neck or at the base of the skull, spreads upward and forward into the head, frequently affects one side more than the other, and is often accompanied by neck pain, stiffness, or restricted movement. These patients have often tried migraine medications without success, used various pain relievers with limited benefit, and may have been told their headaches are 'just tension' without specific characterization or effective treatment.
Schedule Your Appointment
Schedule appointmentWhat many of these patients actually have is cervicogenic headache — a specific, recognized headache type that originates from structures in the cervical spine rather than from the primary headache mechanisms involved in migraine or tension-type headache. The International Classification of Headache Disorders (3rd edition) defines cervicogenic headache through specific diagnostic criteria, and substantial mainstream research has established the condition's underlying mechanisms and treatment frameworks. The 2009 paper by Bogduk and Govind in The Lancet Neurology provides the comprehensive clinical review (Bogduk & Govind, 2009), establishing cervicogenic headache as a distinct clinical entity with cervical structures as the demonstrable pain source.
For patients in Sarasota and surrounding communities dealing with persistent headaches that may have a cervical origin, understanding what cervicogenic headache actually involves clarifies both why standard headache treatments may have produced limited results and what comprehensive approaches can address the underlying cervical source of the pain. This guide walks through the specific diagnostic features of cervicogenic headache, how it differs from migraine and tension-type headache, the cervical anatomy that produces the pain, the standard treatment options, and where upper cervical chiropractic evaluation may fit into comprehensive care at Sarasota Upper Cervical.
What Cervicogenic Headache Actually Is
Cervicogenic headache has specific defining features that distinguish it from other headache types. Understanding these features helps patients recognize whether their headaches may have a cervical origin.
The clinical definition
The International Classification of Headache Disorders defines cervicogenic headache as pain perceived in the head from a source in the neck — specifically, headache caused by a disorder of the cervical spine and its component bony, disc, and/or soft tissue elements, usually but not invariably accompanied by neck pain. The condition is classified as a secondary headache, meaning the head pain is a symptom of an underlying cervical condition rather than a primary headache disorder like migraine. The diagnostic criteria require demonstration that the cervical structures are the source of the pain, typically through clinical features and response to appropriate diagnostic interventions.
The characteristic pain pattern
Cervicogenic headache typically follows a recognizable pain pattern. The pain often begins in the neck or at the base of the skull and spreads upward and forward into the head. The pain is typically unilateral (one-sided), though it can affect both sides. The pain spreads from the back of the head toward the forehead, temple, or behind the eye on the affected side. The pain quality is usually moderate to severe and described as deep, dull, or pressing rather than the throbbing pain of migraine or the band-like quality of tension-type headache. Episodes can last hours to days, and many patients have chronic continuous pain with periodic exacerbations.
The cervical features
Beyond the head pain itself, cervicogenic headache typically involves features pointing to cervical involvement. Patients often have neck pain alongside the headache. Cervical range of motion is typically reduced, particularly in rotation toward the affected side. Specific neck movements or sustained positions can trigger or worsen the headache. Tender points are often present in the suboccipital region or upper cervical area, and pressure on these points can reproduce or worsen the head pain. The cervical features are not just incidental findings — they are part of what establishes the cervicogenic origin of the headache.
The trigger patterns
Specific triggers commonly worsen cervicogenic headache. Sustained postures often worsen the pain — prolonged computer work, extended driving, reading for long periods, or any position that requires sustained cervical muscle activity. Specific head positions can trigger episodes, particularly head rotation or sustained head turning. Pressure on the affected cervical structures can reproduce the headache. External factors like stress, poor sleep, or fatigue can amplify cervicogenic headache patterns just as they amplify other headache types.
The Sjaastad criteria
Beyond the ICHD criteria, the 1998 criteria developed by Sjaastad and colleagues provide additional clinical features useful for diagnosis (Sjaastad et al., 1998). These features include unilateral pain without side-shift, pain triggered by neck movement or sustained positions, restricted cervical range of motion, ipsilateral neck or arm pain, and reduced pain with anesthetic blockade of the appropriate cervical structures. The Sjaastad criteria emphasize the cervical features that distinguish cervicogenic headache from migraine and tension-type headache.
The Cervical Anatomy That Produces the Pain
Cervicogenic headache produces pain in the head from structures in the neck through specific anatomical and neurological mechanisms. Understanding the anatomy clarifies why cervical structural problems can produce head pain.
Related article
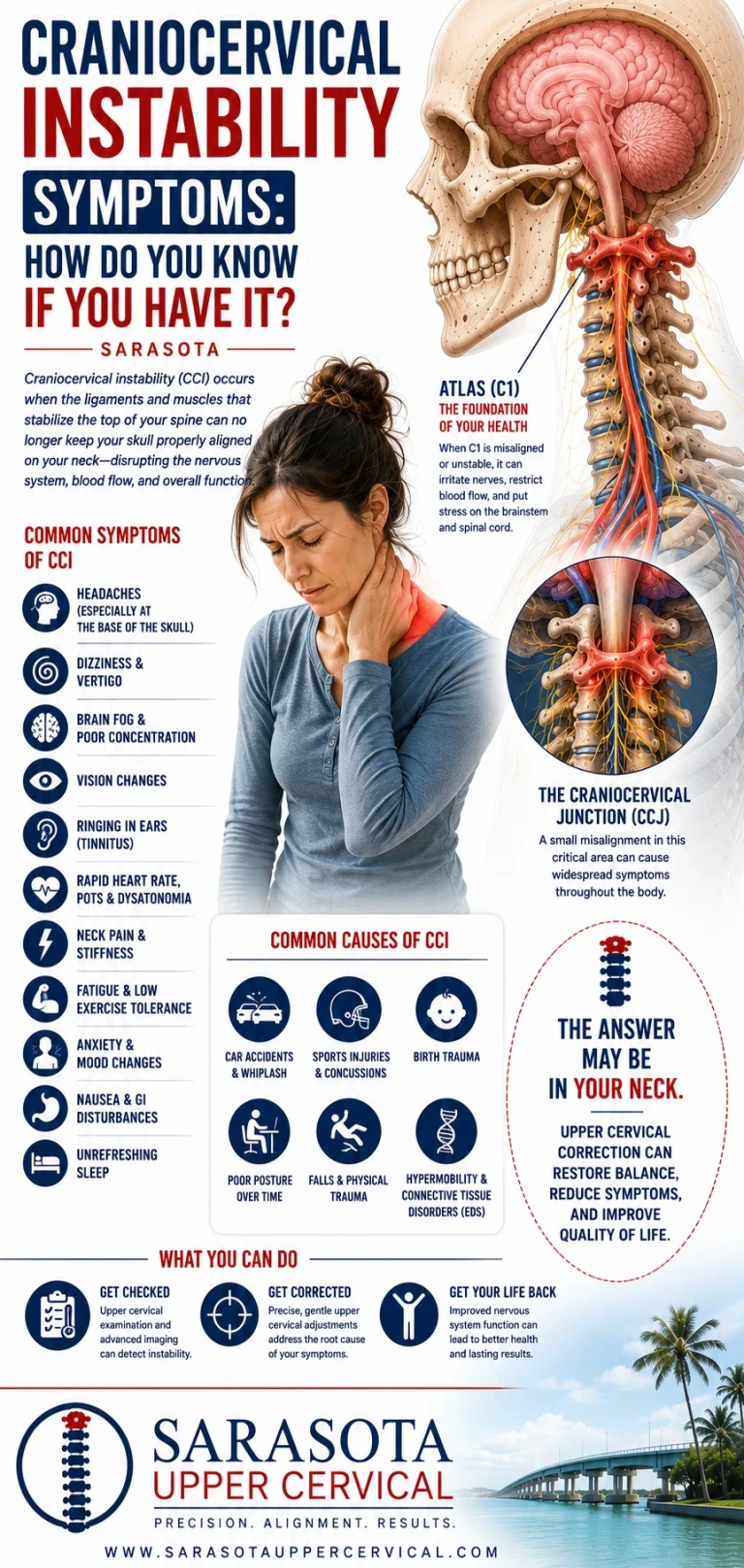
Craniocervical Instability Symptoms: How Do You Know If You Have It? | Sarasota
Jul 29, 2026The trigeminocervical complex
The fundamental anatomical basis for cervicogenic headache is the trigeminocervical complex — a region in the brainstem where sensory input from the trigeminal nerve and the upper cervical nerves converges. The 2003 paper by Bartsch and Goadsby in Current Pain and Headache Reports established this convergence as the anatomical link explaining how cervical structures can produce head pain (Bartsch & Goadsby, 2003). The trigeminal nerve provides sensation to the face and most of the head. The upper cervical nerves (C1-C3) provide sensation to the back of the head and neck. When sensory input from these two systems converges in the trigeminocervical complex, the brain can interpret signals from cervical structures as pain in the head — a phenomenon called referred pain.
Why the upper cervical region specifically
The upper cervical region — the area around the first three cervical vertebrae (C1, C2, C3) — is particularly relevant to cervicogenic headache because of its specific anatomical and neurological features. The upper cervical nerves are the ones that converge with trigeminal input in the trigeminocervical complex. The structures in this region — joints, muscles, ligaments, connective tissues — when affected by structural problems can produce pain that the brain interprets as head pain through this referred pathway. The 2022 narrative review by Peng and colleagues in the Journal of Clinical Medicine summarized the cervical contributions to head pain and dizziness (Peng et al., 2022).
The cervical structures that produce pain
Several specific cervical structures can produce cervicogenic headache. The C2-C3 facet joint, with its third occipital nerve innervation, is one of the most documented sources. The C1-C2 joint complex, with its substantial movement and ligamentous structures, can produce pain when affected. The suboccipital muscles, with their dense proprioceptive innervation and direct connections to the dura mater through the myodural bridge, can produce pain when chronically tense. The cervical discs, while less commonly implicated at upper levels, can occasionally contribute. Each of these structures has specific anatomical relationships and characteristic pain patterns.
The myodural bridge mechanism
One specific mechanism by which cervical muscle problems can produce headache involves the myodural bridge — the connective tissue continuity between the rectus capitis posterior minor muscle and the spinal dura mater documented by Hack and colleagues in 1995 in Spine (Hack et al., 1995). Chronic tension in this muscle, often related to upper cervical structural problems, transmits mechanical force directly to the dura through the bridge. The dura is one of the most pain-sensitive structures in the head, with extensive trigeminal innervation. Sustained dural tension can produce the chronic head pain pattern characteristic of certain cervicogenic and tension-type headaches.
The proprioceptive contribution
Beyond direct pain mechanisms, the upper cervical region's proprioceptive density contributes to cervicogenic headache patterns. The 2001 study by Kulkarni and colleagues in Neurology India documented exceptional muscle spindle density in the suboccipital muscles (Kulkarni et al., 2001), and the 1994 paper by McLain in Spine documented dense mechanoreceptor populations in cervical facet joints (McLain, 1994). When cervical structural problems distort the proprioceptive input from this region, the broader central processing can be affected, contributing to headache patterns and associated symptoms.
How Cervicogenic Headache Differs From Other Headaches
Cervicogenic headache differs in specific ways from migraine and tension-type headache. Understanding these differences helps patients identify whether their headaches may be cervicogenic.
Different from migraine
Migraine typically involves throbbing or pulsating pain, often with associated features like photophobia, phonophobia, nausea, or visual aura. Migraine episodes typically have well-defined onset and offset patterns. Cervicogenic headache differs in having a different pain quality (deep, dull, pressing rather than throbbing), typically lacking the associated migrainous features, having a clearer connection to neck movement or sustained positions, and often presenting with continuous baseline pain rather than discrete attacks. Some patients have both conditions, with cervicogenic headache triggering migraine attacks in susceptible individuals through the trigeminocervical complex.
Different from tension-type headache
Tension-type headache typically produces bilateral, band-like pressing pain without prominent neck features as the primary issue. Cervicogenic headache differs in being more typically unilateral, having clearer cervical features (neck pain, restricted range of motion, trigger patterns), being more responsive to interventions targeting cervical structures, and having a more clearly identifiable cervical source. The two conditions overlap substantially — many patients have features of both — and the myodural bridge mechanism may underlie substantial portions of what is diagnosed as tension-type headache.
Different from sinus headache
Many patients with cervicogenic headache are initially told they have sinus headaches because the referred pain pattern can include frontal, periorbital, or facial pain that suggests sinus origin. Cervicogenic headache differs from true sinus headache in lacking the specific sinus pathology, having clearer neck features, and not responding to sinus-targeted treatments. The 2004 study by Cady and Schreiber published in Headache documented that most patients self-diagnosing 'sinus headache' actually had migraine or other primary headache disorders (Cady & Schreiber, 2004), and a significant portion likely had cervicogenic contribution.
Different from occipital neuralgia
Occipital neuralgia involves sharp, shooting, electric-shock-like pain in the distribution of the occipital nerves. Cervicogenic headache differs in producing more diffuse, deep, pressing pain rather than the paroxysmal sharp pain of neuralgia. The two conditions can coexist — many patients have both — but they are distinct entities with somewhat different specific mechanisms and treatment approaches.
Why accurate diagnosis matters
Accurate diagnosis matters because the treatments differ substantially across headache types. Migraine responds to migraine-specific medications and trigger management. Tension-type headache responds to muscle relaxation, stress management, and addressing underlying muscle tension factors. Cervicogenic headache responds to interventions targeting the cervical source — physical therapy, manual therapy, anesthetic blocks, and structural approaches. Treating cervicogenic headache as if it were migraine often produces inadequate results because the underlying mechanism is different.
Standard Medical and Conservative Treatments
Cervicogenic headache has established treatment options that should form the foundation of comprehensive care. Understanding what standard care involves clarifies the framework within which upper cervical chiropractic operates.
Related article

Why Is My Face Drooping on One Side? | Natural Bell’s Palsy Treatment and Relief in Sarasota
Apr 26, 2026Why Standard Treatment Sometimes Falls Short
Despite the established treatment framework, many cervicogenic headache patients continue to experience headaches despite trying multiple standard approaches. Understanding why standard treatment sometimes falls short clarifies what comprehensive care may need to address.
The structural root cause problem
Many standard treatments address downstream effects of cervicogenic headache without addressing the underlying structural source. Pain medications can reduce pain temporarily but do not address the cervical structural problems producing the pain. Muscle relaxants can reduce tension but do not address why the tension keeps recurring. Posture correction helps but cannot fully resolve underlying structural misalignment. Manual therapy provides relief that often does not last because the structural source returns. When the underlying cervical structural problems persist, the downstream effects keep recurring.
Inadequate evaluation of upper cervical structures
Standard cervical evaluation often does not include the detailed assessment of upper cervical structures that may be most relevant to cervicogenic headache. Standard cervical X-rays may not visualize the upper cervical alignment with sufficient precision. Standard physical therapy evaluation focuses on cervical range of motion and muscle function but may not specifically assess upper cervical structural relationships. The factors that may be driving cervicogenic headache in specific patients may not be identified by standard evaluation approaches.
The chronicity problem
Many cervicogenic headache patients have had symptoms for months or years before seeking effective treatment. Over time, the patterns become chronic — muscle tension becomes entrenched, central sensitization develops, secondary anxiety about pain develops, and the patient's nervous system becomes adapted to chronic pain states. The longer cervicogenic headache persists without effective treatment, the more layered the clinical picture becomes and the more comprehensive treatment must be.
Missing the post-traumatic component
Many cervicogenic headache patients have post-traumatic onset — concussion, whiplash, sports injury, fall — that produced both the cervical structural injury and the headache pattern. The 2005 study by Kaale and colleagues in the Journal of Neurotrauma documented that whiplash mechanisms produce upper cervical ligamentous injuries at forces below those required for diagnosable concussion (Kaale et al., 2005). When trauma was sufficient to produce significant cervicogenic headache, the upper cervical structures essentially always experienced concurrent injury. Standard treatment that doesn't address the cervical structural component leaves a critical factor unaddressed.
The need for comprehensive care
Patients with persistent cervicogenic headache often need comprehensive care addressing multiple components: appropriate medical evaluation and management, physical therapy with cervical-specific protocols, structural evaluation of the upper cervical region, addressing lifestyle and ergonomic factors, managing associated conditions (anxiety, sleep disturbance), and appropriate medications when indicated. Single-modality treatment often produces incomplete results in patients with chronic cervicogenic headache patterns.
How Upper Cervical Evaluation Addresses Cervicogenic Headache
For patients with cervicogenic headache, particularly those with persistent symptoms despite standard treatment, upper cervical chiropractic evaluation can be one component of comprehensive care addressing the structural cervical source of the pain.
The structural focus
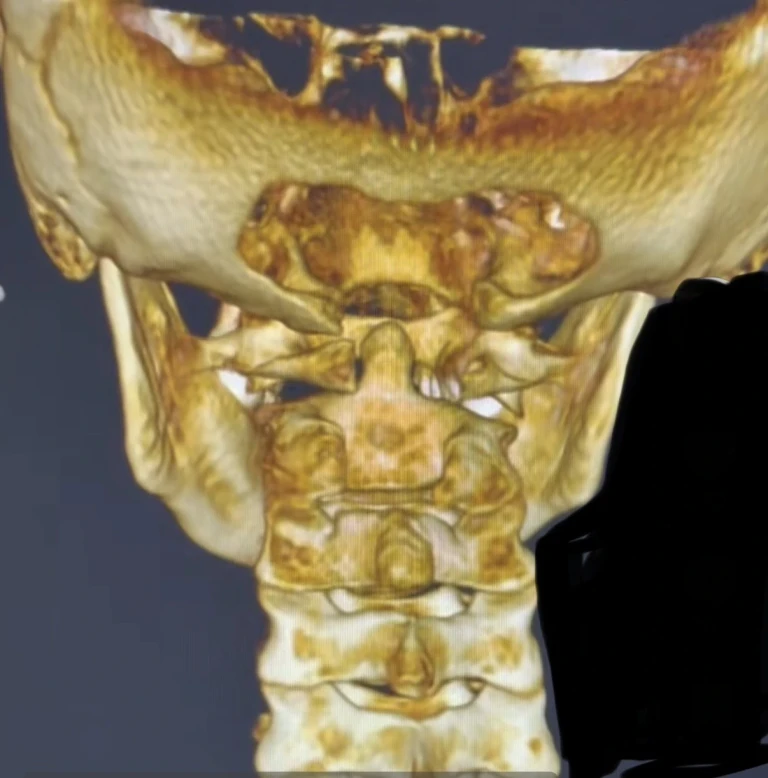
Upper cervical chiropractic focuses specifically on the precise structural relationship between the skull (occiput), atlas (C1), and axis (C2) — the region most relevant to cervicogenic headache. The approach uses three-dimensional cone beam CT imaging to measure alignment with precision to within fractions of a degree. This imaging identifies structural problems at the upper cervical level that may not be apparent on standard imaging. For cervicogenic headache patients with suspected upper cervical involvement, the imaging provides objective assessment of the structural picture.
Objective testing before any intervention
Beyond imaging, objective testing including leg length analysis and paraspinal infrared thermography is performed before any adjustment. Corrections are delivered only when objective findings indicate a structural shift. This principle of restraint guided by data is particularly important for headache patients whose nervous systems are often sensitized — interventions should be objective-finding-based rather than performed routinely. For patients without objective findings indicating need for correction, no intervention is performed.
Precision without manipulation
Upper cervical corrections are specific to the upper cervical segment and delivered along a calculated vector based on the imaging measurements. There is no twisting, no popping, no full-spine manipulation. The force is low. For cervicogenic headache patients — whose cervical structures may be sensitized — this precision is essential. Aggressive cervical manipulation can aggravate sensitized cervical structures and is not appropriate for this population. The precision-based approach is designed for the kind of careful structural correction that cervicogenic headache may benefit from.
What correction may accomplish
For appropriate cervicogenic headache patients, structural correction of the upper cervical region may address several factors. The restored structural alignment allows the compensatory muscle tension to begin resolving. As suboccipital muscle tension decreases, the mechanical effects on the dura through the myodural bridge may decrease. The distorted proprioceptive input may normalize. The mechanical effects on the upper cervical structures contributing to pain referral through the trigeminocervical complex may decrease. The cumulative effect, when correction is appropriate and effective, supports reduction of the headache pattern over weeks to months.
Realistic expectations
Patients pursuing upper cervical evaluation for cervicogenic headache should set realistic expectations. The evaluation identifies whether structural problems are present and addressable. When correction is appropriate and produces clinical benefit, the response is typically gradual over weeks to months rather than immediate. The chronic muscle patterns that developed over time take time to normalize. Multiple corrections may be needed over the course of care. Lack of improvement does not indicate the diagnosis was wrong; it indicates the cervical structural contribution to this specific patient's headaches was limited. Either outcome provides useful clinical information.
Address lifestyle and ergonomic factors
Many cervicogenic headache patients have lifestyle and ergonomic factors contributing to their condition. Workplace ergonomics often need adjustment — monitor height, chair setup, posture during prolonged work. Sleep position and pillow choice affect cervical mechanics. Stress management addresses factors that amplify cervical tension. These foundational components should be addressed alongside any specific treatments.
Related article
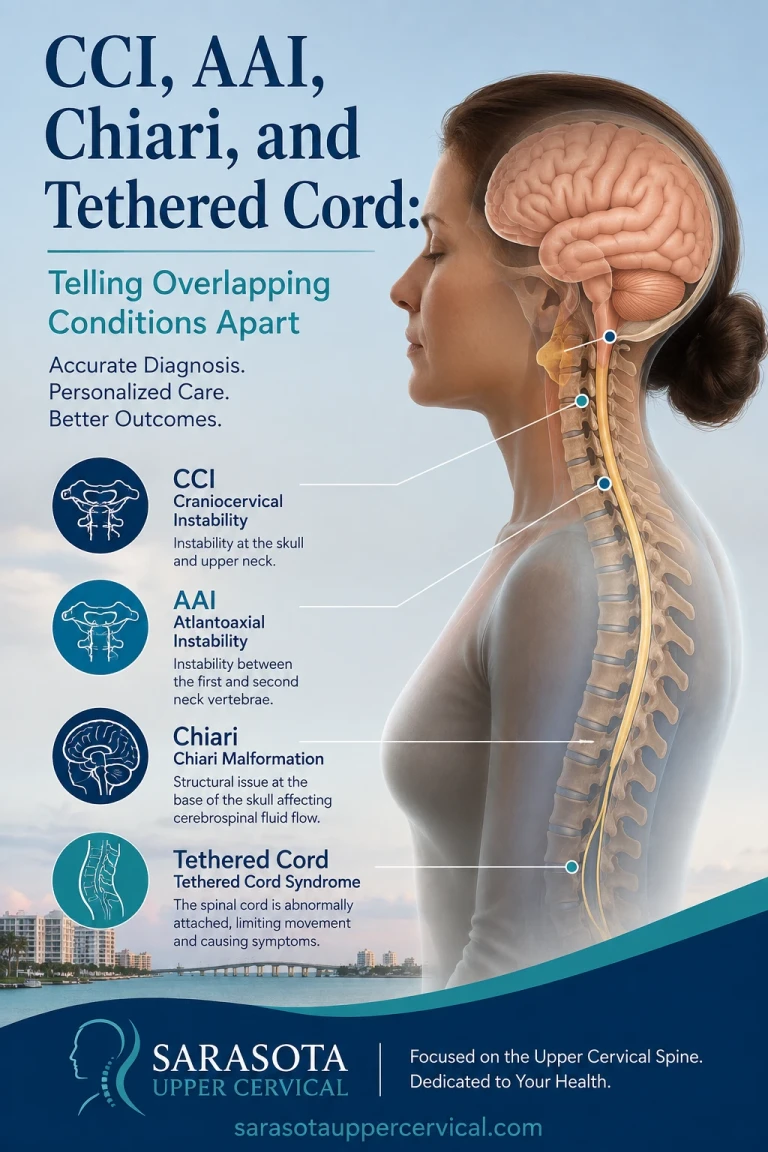
CCI, AAI, Chiari, and Tethered Cord: Telling Overlapping Conditions Apart | Sarasota
Aug 01, 2026Manage associated conditions
Cervicogenic headache patients often have associated conditions that affect overall function. Anxiety about persistent pain develops in many patients and may require specific attention. Sleep disturbance is common and worsens overall pain experience. Depression can develop with chronic pain conditions. Addressing these associated conditions is part of comprehensive care.
When to Consider an Upper Cervical Evaluation at Sarasota Upper Cervical
Upper cervical evaluation may be worth considering for cervicogenic headache patients when any of the following are true:
Your headaches start at the base of the skull or in the neck and spread upward into the head. You have associated neck symptoms — chronic neck pain, restricted cervical range of motion, suboccipital tension, tenderness at the base of the skull. Your headaches developed after head or neck trauma — concussion, whiplash, sports injury, fall. Your headaches worsen with sustained postures, computer work, or specific head positions. Your headaches have not responded adequately to standard headache treatments. You have been diagnosed with cervicogenic headache and are seeking comprehensive evaluation. You have prior concussions or significant neck trauma layered on top of your current presentation. Your trigger points are clearly located in the upper cervical region.
For patients with headaches responding well to standard treatment, headaches clearly attributable to other causes, headaches with red flag features requiring urgent medical evaluation, or acute severe new headache patterns, upper cervical chiropractic is not the appropriate first step. Standard medical evaluation should always be your first priority for any significant headache concern.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Important Safety Considerations
Several safety considerations apply to patients with headaches considering any care approach including upper cervical evaluation.
Sudden severe headache (the worst headache of your life), new neurological symptoms (vision changes, weakness, numbness, speech difficulties, confusion), severe headache with fever and neck stiffness (potential meningitis), or headaches with associated trauma require urgent medical evaluation rather than chiropractic care. These features can indicate serious underlying conditions requiring immediate medical management.
New onset headache patterns particularly in older adults, progressively worsening headaches over weeks to months, headaches that wake patients from sleep, headaches that are worse with cough or straining, or headaches with associated systemic symptoms (weight loss, fever, malaise) require medical evaluation for potential serious causes before assuming musculoskeletal origin.
Where to Go From Here
Cervicogenic headache is a specific, recognized headache type that originates from structures in the cervical spine. The condition has established diagnostic criteria, recognized clinical features distinguishing it from migraine and tension-type headache, well-characterized anatomical mechanisms involving the trigeminocervical complex and upper cervical structures, and established treatment frameworks including physical therapy, anesthetic interventions, medications, and for appropriate patients, structural cervical approaches. The condition affects substantial numbers of headache patients, many of whom continue to struggle with persistent symptoms despite trying multiple treatment approaches.
For patients in Sarasota and surrounding communities whose headaches have features suggesting cervical origin, comprehensive evaluation matters. Medical evaluation by appropriate providers establishes the diagnosis. Physical therapy addressing cervical mechanics provides foundational treatment. Upper cervical evaluation can be one component of comprehensive care addressing the structural cervical factors at the source of the headaches. The combination of appropriate medical management, conservative interventions, and when indicated, structural cervical evaluation provides the comprehensive approach that chronic cervicogenic headache often requires.
At Sarasota Upper Cervical, we focus on the precise structural relationship between the skull, atlas, and axis — the region most directly relevant to cervicogenic headache patterns. Our approach uses three-dimensional CBCT imaging and objective testing to evaluate whether structural problems may be contributing to your headache pattern, with precision-based corrections when appropriate. We work alongside your medical team rather than replacing standard care, providing a specific component of the comprehensive approach your situation may require.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Headache Classification Committee of the International Headache Society (IHS). (2018). The International Classification of Headache Disorders, 3rd edition. Cephalalgia, 38(1), 1–211.
Bogduk, N., & Govind, J. (2009). Cervicogenic headache: An assessment of the evidence on clinical diagnosis, invasive tests, and treatment. The Lancet Neurology, 8(10), 959–968.
Sjaastad, O., Fredriksen, T. A., & Pfaffenrath, V. (1998). Cervicogenic headache: Diagnostic criteria. The Cervicogenic Headache International Study Group. Headache, 38(6), 442–445.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Page, P. (2011). Cervicogenic headaches: An evidence-led approach to clinical management. International Journal of Sports Physical Therapy, 6(3), 254–266.
Bronfort, G., Haas, M., Evans, R., Leininger, B., & Triano, J. (2012). Effectiveness of manual therapies: The UK evidence report. Chiropractic & Manual Therapies, 18, 3.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Peng, B., Yang, L., Yang, C., Pang, X., Chen, X., & Wu, Y. (2022). Proprioceptive cervicogenic dizziness: A narrative review of pathogenesis, diagnosis, and treatment. Journal of Clinical Medicine, 11(21), 6293.
Cady, R. K., & Schreiber, C. P. (2004). Sinus headache: A clinical conundrum. Otolaryngologic Clinics of North America, 37(2), 267–288.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with persistent or significant headaches should pursue appropriate medical evaluation to establish accurate diagnosis and rule out serious underlying causes. Standard evidence-based headache treatments should form the foundation of care. Upper cervical evaluation should be considered a complementary approach for appropriate patient subsets rather than a primary treatment for headache disorders. Patients with sudden severe headache, new headache patterns, headaches with neurological symptoms, or other red flag features should seek urgent medical evaluation. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment