
"Both are one-sided. Both can be constant. But one starts in your neck — and that difference changes everything about what you should do next"
Sarasota Upper Cervical · Serving Sarasota - Bradenton-Lakewood Ranch - Venice - Parrish -Englewood - Osprey
Schedule Your Appointment
Schedule appointmentIf you've lived with a one-sided headache that never fully goes away, you've probably been handed more than one label for it. These headaches are easy to confuse because they share a surface description: continuous, on one side, sometimes flaring worse than others. But underneath that description sit very different problems with very different solutions.
Two that get mixed up are cervicogenic headache — a headache driven by the upper neck — and hemicrania continua, a primary headache disorder. Telling them apart matters, because the path forward for one has nothing to do with the path forward for the other. This article focuses mostly on the cervicogenic side, because it's the one most often missed — and the one where the source can frequently be found in a place no one thought to look: the top of the neck.
Start with the most overlooked suspect: your upper neck
The single biggest reason one-sided headaches go unsolved is that the neck is rarely examined as the source. People with a headache get their head looked at. They get their eyes checked, their sinuses checked, their stress and sleep questioned. The two vertebrae at the very top of the neck — the ones sitting directly beneath the skull — are almost never part of the conversation. And those two vertebrae are exactly where a cervicogenic headache begins.
Request a FREE Consultation- 941 259-1891
A cervicogenic headache is, by definition, a headache referred from the neck. The pain is felt in the head, but the generator is in the upper cervical spine. That's not a theory unique to us — it's the established meaning of the term. What's less widely appreciated is just how directly the top of the neck is wired into the parts of the head where pain shows up.
Related article
vertebrobasilar insufficiency syndrome and the neck - treatment and relief in Sarasota
Jun 23, 2026Why a neck problem is felt in your head
At the base of your skull, the sensory nerves from your upper neck (the C1, C2, and C3 levels) feed into the same brainstem junction as the trigeminal nerve, which carries sensation from your face, forehead, and the area around your eye. This junction is called the trigeminocervical complex, and the upper neck and the head region don't just sit near each other there — their signals can converge onto the very same nerve cells.
The practical consequence is simple and important: when the top of the neck is a source of ongoing irritation, your brain can interpret that signal as head pain — one-sided, behind or around the eye, at the temple, or wrapping from the base of the skull forward. The neck is the source; the head is the screen it gets projected onto.
Request a FREE Consultation- 941 259-1891
The choke point
The upper neck is a narrow, high-traffic junction where the spine meets the skull — a place where nerves, blood flow, and the very top of the spinal cord all pass through a tight space. When the alignment of the top two vertebrae is disturbed, this junction becomes a source of irritation that the rest of the head feels. We call it the choke point because so much depends on it staying clear and balanced.
What makes a headache look cervicogenic
Certain features point toward the neck as the driver. None of these is a self-diagnosis — they're the clues that make a proper upper cervical evaluation worthwhile:
It stays on one side and tends to start at the back of the head or base of the skull before spreading forward toward the temple or eye.
Neck movement or sustained positions change it — long hours at a screen, sleeping wrong, or holding your head in one posture makes it worse.
There's a history of neck trauma — a car accident, a fall, a sports injury, even years earlier. Old upper-neck injuries are a recurring thread.
Pressing certain spots at the top of the neck reproduces or worsens the familiar head pain.
Reduced or stiff neck movement on the painful side.
When this is the pattern, the headache isn't really a "head" problem at all. It's a neck problem that happens to be felt in the head — and that's a problem with a structural source you can actually evaluate.
Related article

Tinnitus Relief: Understanding the Upper Cervical Connection to Ear Ringing
Jan 26, 2026So where does hemicrania continua come in?
Here's the short, honest version, because you deserve to know what else a one-sided constant headache can be.
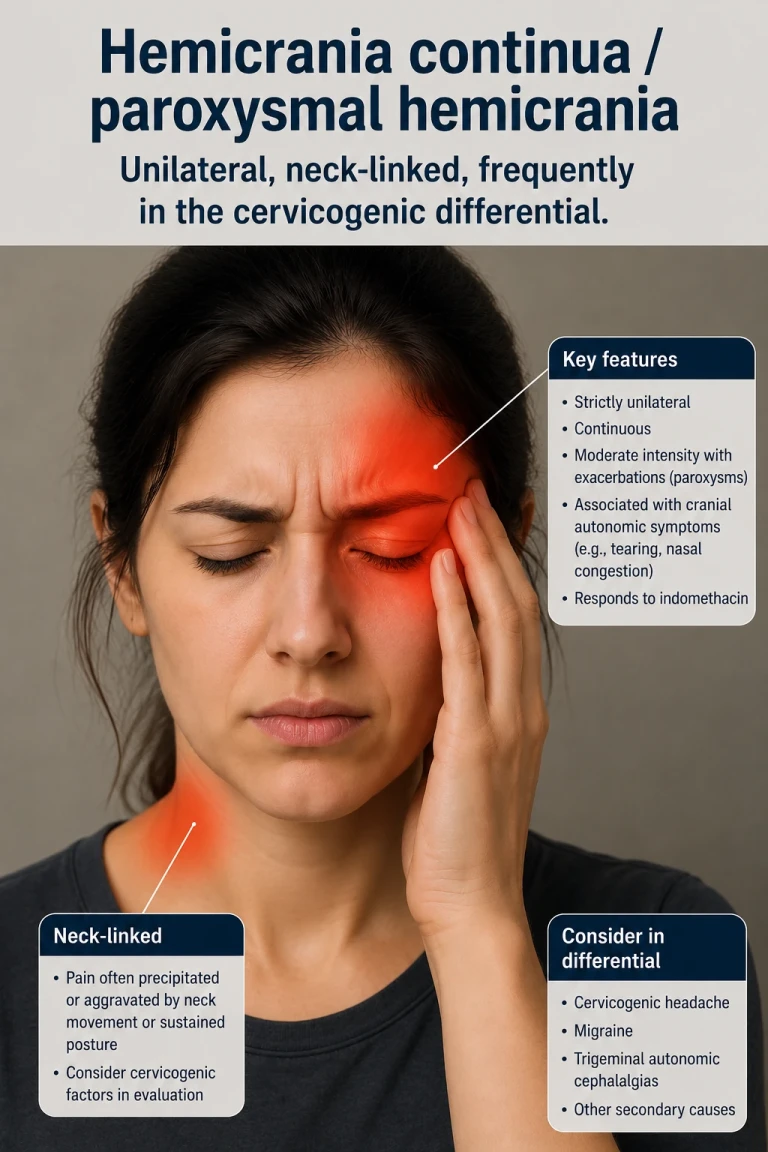
Hemicrania continua (and its short-attack relative, paroxysmal hemicrania) are primary headache disorders — meaning the headache is the condition itself, not a symptom referred from somewhere else like the neck. They're one-sided and continuous, which is why they get confused with cervicogenic headache. But they carry two tells that point away from the neck:
Autonomic signs on the painful side — a watering or red eye, a drooping or swollen eyelid, a stuffy or running nostril, all on the same side as the pain. Cervicogenic headache typically doesn't produce these.
A complete response to one specific prescription medication (indomethacin). This response is so reliable that doctors use it to confirm the diagnosis. Cervicogenic headache does not behave this way.
That second point is the cleanest dividing line of all. If a one-sided constant headache resolves completely on that specific medication, it's pointing toward hemicrania continua, and that's a conversation for a physician — not something upper cervical care treats or claims to. We're telling you this precisely so you don't waste months in the wrong place. Getting the label right is the whole point of this article.
A quick side-by-side — for understanding, not self-diagnosis.
Cervicogenic headache
Hemicrania continua
Where it comes from
Referred from the upper neck
A primary headache disorder of its own
Changes with neck movement or posture
Often, yes
Usually not
Eye watering, droopy lid, stuffy nose on the painful side
Typically absent
Commonly present in flares
Linked to a past neck injury
Frequently
Not characteristically
Confirmed by complete response to indomethacin
No
Yes — this is the hallmark
Why getting this right matters so much
These two conditions don't just have different causes — they have completely different solutions. A headache driven by the upper neck won't be solved by treating it as a primary headache disorder, and a primary headache disorder won't be solved by addressing the neck. People spend years cycling through the wrong approach simply because no one stopped to ask which problem they actually had. The first job isn't treatment — it's identifying the right source.
How we look at it in Sarasota
Upper cervical chiropractic focuses on the alignment and movement of the top two vertebrae of the neck — the structures most likely to be the hidden source of a cervicogenic headache. Our approach is built around finding the source first.
That starts with an evaluation, not a treatment. We take a careful history — including injuries you may have forgotten about — and examine how the top of your neck is aligning and moving. If we find an upper cervical pattern that fits your headache, we'll explain it in plain language and discuss whether gentle, precise upper cervical care is appropriate for you. The corrections themselves are specific and low-force — none of the forceful twisting people often picture with chiropractic.
Related article
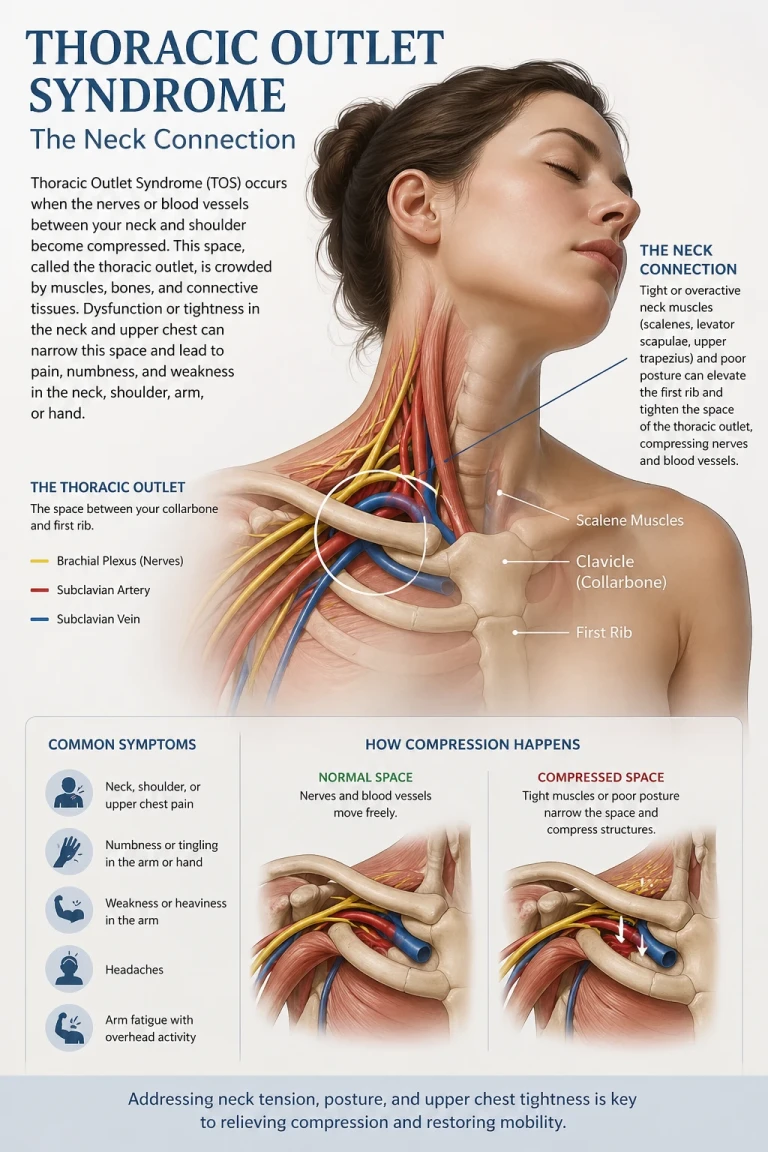
Thoracic Outlet Syndrome Treatment and Relief Sarasota | Sarasota Upper Cervical
Apr 28, 2026And if your headache doesn't fit the cervical picture — if the signs point toward hemicrania continua or another primary headache disorder — we'll tell you that honestly and help you get to the right kind of provider. Sending you to the right place is part of doing this well. Individual results vary, and a thorough examination is the only way to know whether your upper neck is the source in your case.
How would I know if my headache is coming from my neck?
Common clues include pain that stays on one side and starts at the base of the skull, headaches that change with neck movement or sustained posture, a history of neck injury, and reduced neck motion. These are reasons to have your upper neck evaluated — they aren't a self-diagnosis. An examination is the only way to know.
I have a watering eye and stuffy nose with my headache. What does that suggest?
Autonomic signs like a watering or red eye, a droopy or swollen eyelid, and a stuffy or running nostril on the painful side are more typical of the trigeminal autonomic headaches, including hemicrania continua, than of cervicogenic headache. If you have these features, it's worth raising them with a physician.
What does an upper cervical evaluation involve?
It starts with a detailed history and an examination of how the top of your neck is aligning and moving. If a structural pattern is found that fits your symptoms, we explain it plainly and discuss whether gentle, precise upper cervical care is appropriate. If your headache doesn't fit the cervical picture, we'll point you toward the right provider.
References
Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (ICHD-3).
Bogduk N, Govind J. Cervicogenic headache: assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurology.
Prakash S, Patel P. Hemicrania continua: clinical review, diagnosis and management. Journal of Pain Research, 2017.
Hemicrania Continua. StatPearls, NCBI Bookshelf, 2024.
Bartsch T, Goadsby PJ. Anatomy and physiology of pain referral in the trigeminocervical complex.
This article is for general educational purposes only and does not constitute medical advice, diagnosis, or treatment, and it does not establish a doctor–patient relationship. Cervicogenic headache, hemicrania continua, and paroxysmal hemicrania require professional evaluation to diagnose. Results of upper cervical care vary from person to person, and no specific outcome is promised or guaranteed. If you are experiencing a severe, sudden, or rapidly worsening headache, or a headache with neurological symptoms, seek medical care promptly. Always consult your physician or other qualified health provider with questions about a medical condition.



Leave a comment