
How upper cervical care addresses the brainstem and cervical spine connection at the root of facial nerve irritation.
Trigeminal neuralgia, often called TN or the “suicide disease” because of its devastating intensity, is one of the most painful conditions in modern medicine. Patients describe sudden, electric-shock-like attacks across the face, triggered by something as simple as brushing teeth, chewing, smiling, a cool breeze, or even a light touch. For many people in the Sarasota area, the condition disrupts work, relationships, sleep, and the basic ability to enjoy daily life.
Schedule Your Appointment
Schedule appointmentConventional treatment typically focuses on managing the pain rather than addressing what is irritating the nerve in the first place. Medications such as anticonvulsants, nerve blocks, and in some cases surgical procedures like microvascular decompression or rhizotomy are common pathways. While these can offer relief for some, many patients find the relief incomplete, temporary, or accompanied by side effects that introduce new challenges.
At Sarasota upper cervical, we approach TN from a different angle. Rather than asking only how to quiet the pain, we ask why the trigeminal nerve is misfiring in the first place — and that question leads us directly to the brainstem and the upper cervical spine.
Understanding Trigeminal Neuralgia
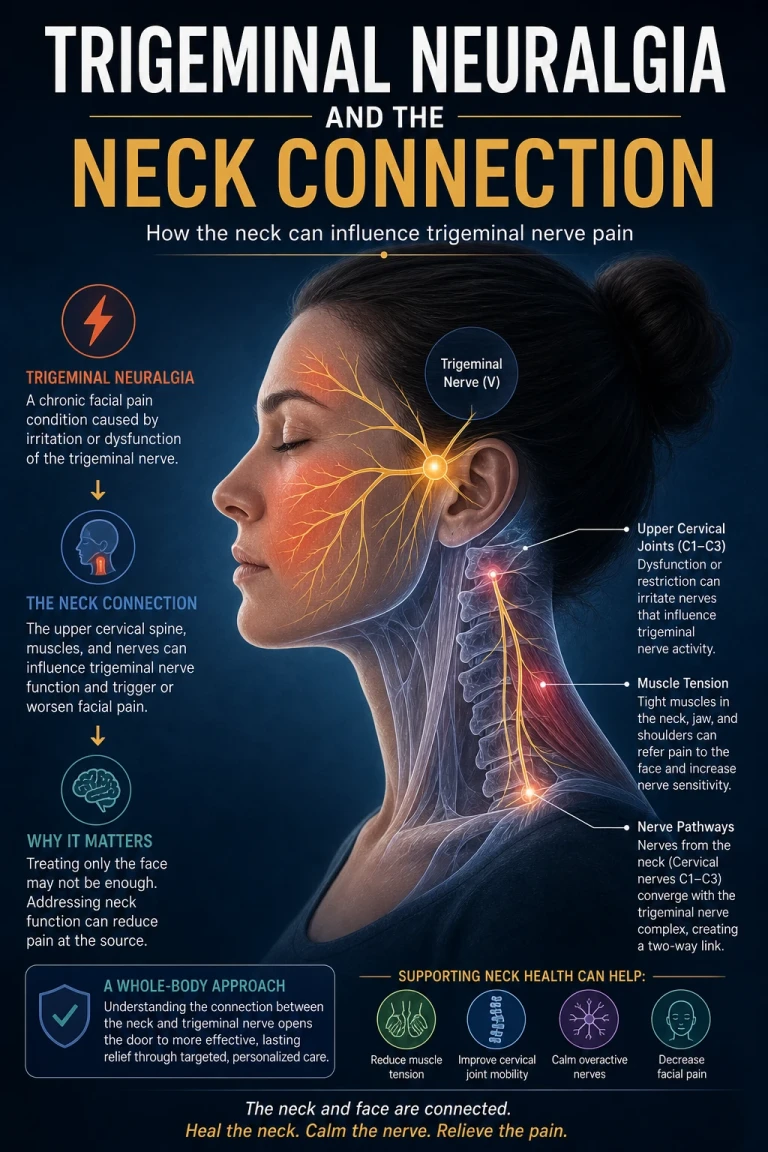
The trigeminal nerve is the fifth cranial nerve and the largest of the cranial nerves. It is responsible for almost all of the sensation in the face, as well as the motor function of chewing. It has three primary branches: the ophthalmic branch (forehead and eye area), the maxillary branch (cheek, upper jaw, and upper teeth), and the mandibular branch (lower jaw, lower teeth, and part of the ear).
In trigeminal neuralgia, this nerve becomes hypersensitive and reactive. Signals that should register as ordinary touch or temperature instead fire as searing, stabbing, or electrical pain. Episodes can last seconds or minutes, and clusters of attacks can continue for weeks before easing. Over time, the pattern often worsens, with longer episodes, shorter pain-free intervals, and a growing list of triggers.
The medical community generally divides TN into two categories. Classical or Type 1 TN involves sharp, episodic, shock-like pain. Atypical or Type 2 TN involves a more constant, burning, aching quality. Many patients experience features of both. Imaging sometimes reveals a blood vessel pressing on the trigeminal nerve where it exits the brainstem, but a meaningful number of patients show no clear structural cause on standard imaging — which is part of what makes TN so frustrating to live with and to treat.
Related article
The Brainstem: Where the Trigeminal System Lives
To understand why upper cervical care matters for TN, it helps to look at where the trigeminal nerve actually originates. The trigeminal nerve emerges from the brainstem, specifically from a region called the pons. From there, its sensory fibers travel down into a long structure known as the spinal trigeminal nucleus, which extends from the brainstem all the way down into the upper segments of the cervical spinal cord.
This is a critical anatomical detail. The spinal trigeminal nucleus is not contained neatly inside the skull. It physically extends down into the region of the upper neck, often reaching as far as the C2 or C3 spinal level. That means the same neurological pathway responsible for facial sensation runs directly through the territory governed by the top two vertebrae of the spine — the atlas (C1) and the axis (C2).
Researchers refer to the functional overlap of head, neck, and facial nerve input in this region as the trigeminocervical complex. In this complex, sensory information from the upper cervical nerves and the trigeminal nerve converges in the brainstem and shares the same processing pathways. This convergence is now well established in the neurology and headache literature, and it explains why neck issues so frequently produce face, jaw, and head symptoms — and why facial nerve conditions so frequently coexist with neck dysfunction.
How Upper Cervical Misalignment Can Irritate the System
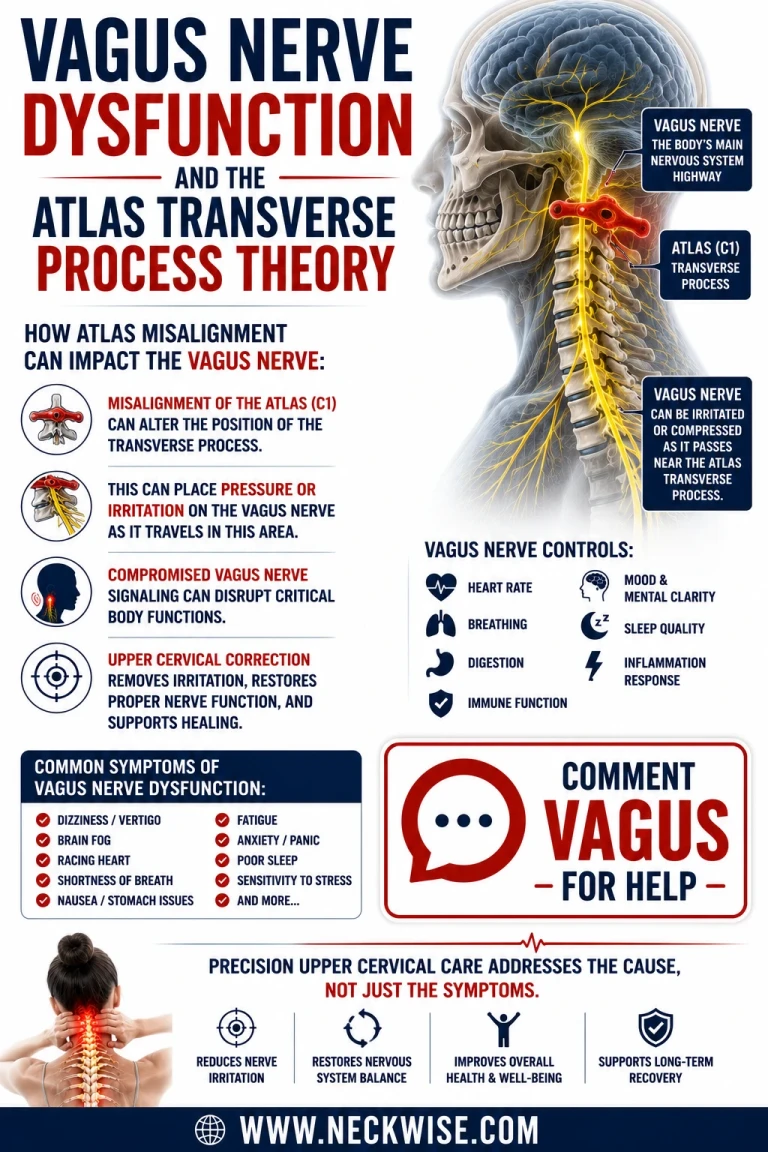
The atlas (C1) is the top vertebra of the spine. It sits directly beneath the skull and surrounds the brainstem and the upper portion of the spinal cord. Unlike the rest of the spine, the atlas has no disc above or below it, and it relies on a delicate balance of ligaments and small muscles to remain properly aligned. When the atlas shifts even a fraction of a millimeter out of its ideal position, it can place mechanical irritation on the surrounding neural structures.
Because the spinal trigeminal nucleus extends into the upper cervical region, mechanical irritation at the C1-C2 area has a plausible and increasingly documented relationship with trigeminal symptoms. When the upper cervical spine is misaligned, several things can occur:
• Mechanical irritation of the brainstem and upper spinal cord, where the trigeminal pathway lives.
• Altered blood flow and cerebrospinal fluid drainage through the small openings at the base of the skull.
• Sustained tension and dysfunction in the suboccipital muscles, which feed sensory input directly into the trigeminocervical complex.
• Disrupted communication between the brainstem and the body, contributing to a hyper-reactive nervous system.
In a system that is already on edge — as it is in TN — these forms of low-grade, ongoing irritation can act as a constant background stimulus that lowers the threshold for an attack. Patients often describe their nervous system as feeling “wired” or “on high alert,” and when the upper cervical spine is involved, that description is often more literal than figurative.
Why So Many TN Patients Have a History of Neck Trauma
One of the most consistent patterns we see at Neckwise is that patients with trigeminal neuralgia often have a history of head or neck trauma — sometimes recent, sometimes decades old. Common contributors include car accidents, sports injuries, falls, dental procedures involving prolonged jaw opening, and even childhood injuries that were never thought to be significant at the time.
These events can disturb the delicate alignment of the atlas and axis, and the body often compensates around the misalignment for years before symptoms appear. The trigeminal system is remarkably resilient, but it has a threshold. Add enough stress over enough time — postural strain, hidden inflammation, accumulated tension at the base of the skull — and that threshold is eventually crossed. The result, for some patients, is the onset of TN symptoms that seem to appear out of nowhere.
Understanding this history is part of why the upper cervical evaluation is so important. The injury that started the cascade may be long forgotten, but its mechanical legacy in the upper neck can still be present and measurable today.
The Neckwise Approach in Sarasota
Neckwise focuses on precision upper cervical care. Our work centers on identifying and correcting misalignment of the atlas and axis with a level of accuracy that general chiropractic does not require. Because the upper cervical region sits so close to the brainstem and the trigeminal pathway, precision is non-negotiable.
Related article
Chiari Malformation Healing After Surgery: A Sarasota Upper Cervical Success Story
Apr 14, 2026The process begins with a comprehensive consultation and neurological examination. We listen to the full history of the condition, including prior injuries, prior treatments, and the specific patterns of pain — what triggers an episode, what relieves it, and how it has changed over time. From there, we use CBCT 3D imaging as a precision tool to visualize the upper cervical spine in three dimensions. This imaging is not used for diagnosis of TN itself, but to map the exact position of the atlas and axis so that any correction can be planned with millimeter-level specificity.
If a misalignment is identified and the patient is a candidate for care, the doctor delivers a pinpoint atlas adjustment. This is not a forceful, high-velocity manipulation of the neck. It is a controlled, precise correction designed to allow the upper cervical spine to return to its ideal position so that the surrounding neural structures are no longer mechanically irritated. From there, the body is given the time and the inputs it needs to heal — which is the central premise of our 12-Week Corrective Program.
What Patients Can Realistically Expect
Trigeminal neuralgia is a serious neurological condition, and Neckwise does not present upper cervical care as a guaranteed cure. What we can say is this: when the upper cervical spine is contributing to the irritation of the trigeminal system, correcting that misalignment can meaningfully reduce the stress on the nerve and create the conditions in which the nervous system can begin to settle.
Many patients report that as care progresses, the frequency and intensity of their attacks decrease. Some find that triggers which used to set off a full episode now produce only a flicker, or nothing at all. Some experience longer pain-free intervals between episodes and a return of confidence in everyday activities — eating, talking, going outside on a windy day. Healing in the nervous system is not always linear, and progress in TN often comes in steps rather than a single dramatic moment. Sustained improvement typically requires consistent care over a period of weeks to months, which is why our corrective program is structured the way it is.
Upper cervical care can also be integrated alongside the care a patient is receiving from their neurologist or primary physician. We do not ask patients to stop medications or abandon other treatment pathways. Our role is to address a specific mechanical and neurological factor that is often overlooked — the relationship between the upper cervical spine and the brainstem — and to offer that piece of the puzzle to patients who have not found lasting answers elsewhere.
Taking the Next Step in Sarasota
If you are searching for a trigeminal neuralgia specialist in Sarasota, and especially if your search has already taken you through neurologists, dentists, oral surgeons, and pain management clinics, an upper cervical evaluation may be a meaningful next step. The connection between the brainstem, the cervical spine, and the trigeminal system is not theoretical — it is anatomical, and it is increasingly supported by the literature on the trigeminocervical complex and chronic facial pain.
Neckwise serves the Sarasota community with two locations and a team trained specifically in upper cervical care. Our process is designed to determine whether the upper cervical spine is part of your TN picture, and if so, to correct it with the precision the region demands. For patients who have spent years being told there is nothing more to be done, the discovery that a small, specific misalignment may have been driving a much larger problem can be the beginning of real change.
To learn more or schedule a consultation, contact Neckwise Sarasota. Relief from trigeminal neuralgia is not always simple, but it often begins by looking in the right place — and that place, more often than not is the neck.



Leave a comment