
How the nervous system controls the immune system, why the brainstem sits at the center of long COVID, and how a structural problem at the head-neck junction can keep the body locked in chronic inflammation.
Long COVID has produced one of the most challenging clinical pictures of the last several years. Patients who were once healthy now describe a persistent constellation of fatigue, brain fog, dizziness, autonomic instability, post-exertional crashes, and a body that feels permanently inflamed. The acute infection has long since cleared, but the symptoms remain. Standard blood work often comes back normal or only mildly abnormal. Imaging is unremarkable. Patients are told the science is still emerging, that recovery is unpredictable, and that there is no clear treatment pathway.
Schedule Your Appointment
Schedule appointmentThat answer is honest, but it is also incomplete. The emerging science around long COVID is increasingly pointing in a specific direction: chronic neuroinflammation, autonomic dysregulation, and dysfunction in the brainstem — the very region that sits inside the upper cervical corridor. At Neckwise in Sarasota, we focus on a part of the picture that the conventional workup is rarely designed to evaluate. The structural relationship between the head and the neck has a direct influence on the brainstem, the autonomic nervous system, and through them, the immune system itself. For a meaningful subset of long COVID patients, a structural problem at the head-neck junction is not just a contributor to their symptoms — it may be the reason their body cannot exit the inflammatory state in the first place.
Neuroimmunology: The Nervous System Controls the Immune System
For most of medical history, the nervous system and the immune system were studied in isolation. The brain controlled thinking, sensation, and movement. The immune system fought infection. They were considered functionally separate. The last two decades of research have demonstrated that this view is wrong. The nervous system and the immune system are deeply interconnected — so much so that the field of neuroimmunology has emerged specifically to study how they communicate.
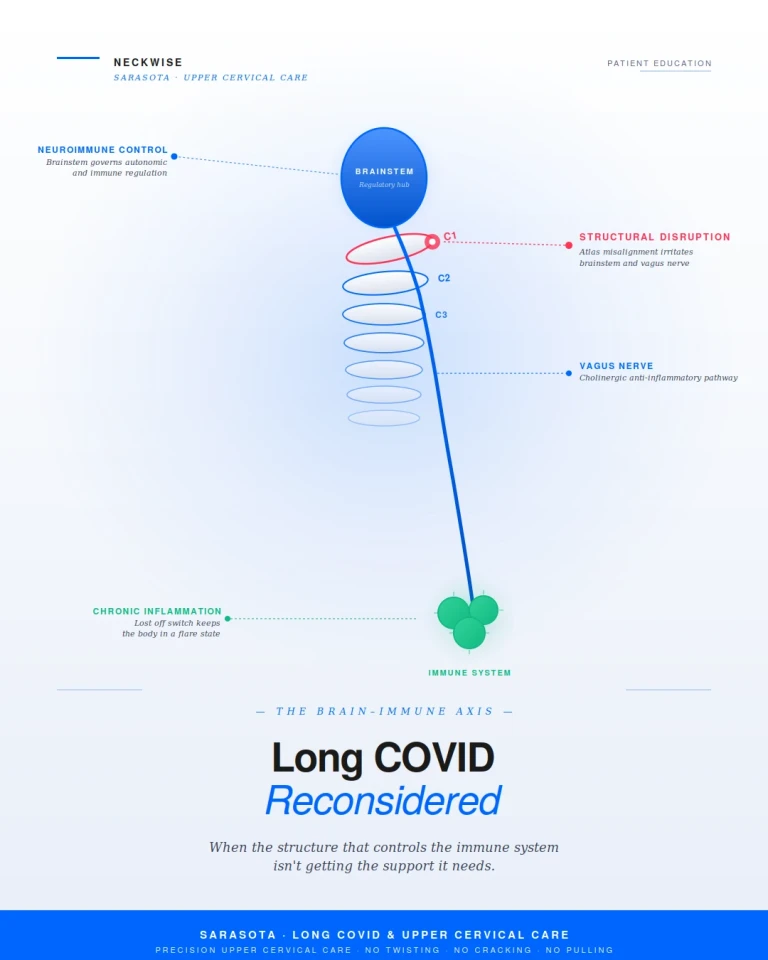
The autonomic nervous system, particularly the vagus nerve, is one of the central pathways through which the brain regulates the immune response. Through what researchers call the cholinergic anti-inflammatory pathway, the vagus nerve actively suppresses the release of inflammatory cytokines from immune cells. When vagus nerve function is robust, the immune system stays appropriately calibrated — it responds to threats and then stands down. When vagus nerve function is impaired, that off switch becomes harder to engage, and the immune system tends to remain in a low-grade, persistent state of activation.
The brainstem is the regulatory hub for this entire system. The vagus nerve emerges from the brainstem. The autonomic centers that govern heart rate, blood pressure, and inflammatory tone are located in the brainstem. The cerebrospinal fluid pathways that clear inflammatory metabolites from the brain pass through the craniocervical junction. The blood vessels that supply the brainstem with oxygen and remove waste pass through the same narrow corridor. The immune system, the nervous system, and the structural mechanics of the upper neck are not separate stories. They are one story, told from three angles.
Why Long COVID Looks Like a Brainstem Problem
The symptom pattern of long COVID is remarkably consistent, and once you know what to look for, it reads like a textbook description of brainstem and autonomic dysfunction. The acute viral infection appears to leave behind a state of chronic neuroinflammation, particularly affecting the brainstem and its surrounding tissues. The vagus nerve becomes mechanically and chemically irritated. The autonomic balance between sympathetic activation and parasympathetic recovery is lost. The cerebrospinal fluid that normally clears inflammatory waste no longer circulates as freely as it should. The result is a body that cannot calm down, cannot recover, and cannot return to baseline.
This pattern explains why long COVID symptoms are so diverse and so seemingly unrelated. They are not separate problems. They are the downstream expression of a single upstream issue — a brainstem and autonomic system stuck in a state of dysregulation, with inflammation that the body cannot resolve on its own.
Common Long COVID Symptoms and the Inflammatory Pattern
Patients with long COVID typically describe a wide-ranging combination of symptoms that touch nearly every system in the body. The full list is long, but the pattern points consistently back to neuroinflammation, autonomic dysregulation, and brainstem involvement. Common symptoms include:
Related article
• Persistent fatigue that is not relieved by rest, often described as a heaviness that no amount of sleep can fix
• Brain fog, difficulty concentrating, word-finding problems, and a sense of mental cloudiness
• Post-exertional malaise — a profound crash that follows even mild physical or cognitive activity
• Dizziness, lightheadedness, and a sense of being off-balance even while standing still
• Heart palpitations, racing heart on standing, and other signs of autonomic dysregulation including features of POTS
• Shortness of breath that does not match findings on pulmonary testing
• Headaches and migraines, often new in onset or significantly worse than before the infection
• Sleep disturbance, insomnia, or unrefreshing sleep that leaves patients exhausted on waking
• Persistent low-grade fever or temperature dysregulation
• Gastrointestinal symptoms — nausea, bloating, altered motility, food sensitivities
• Tingling, numbness, or burning sensations in the hands, feet, or face
Related article
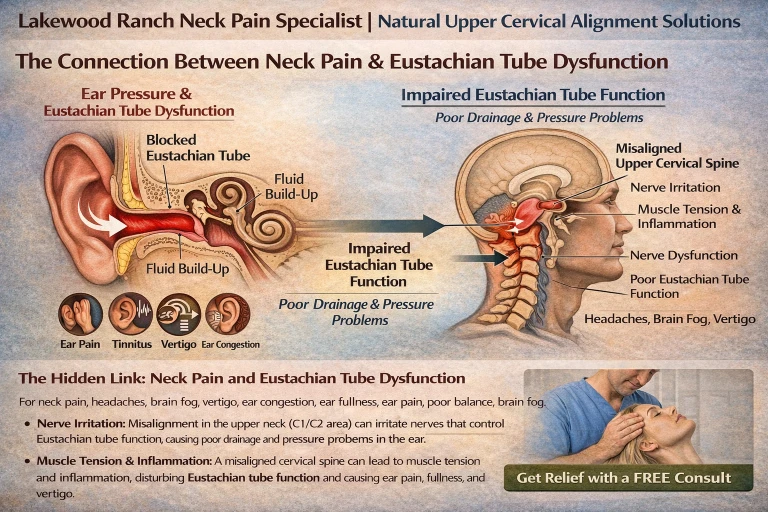
Lakewood Ranch Neck Pain Specialist | Natural Upper Cervical Alignment Solutions
Mar 19, 2026• Neck pain, neck stiffness, and tension at the base of the skull
• Heightened sensitivity to light, sound, and stress
• Mood symptoms — anxiety, depression, and a sense of being in fight-or-flight constantly
Each of these symptoms can be traced back to inflammation in or around the brainstem and the dysregulation of the autonomic nervous system that follows. The fatigue is not laziness. The brain fog is not anxiety. The post-exertional crashes are not deconditioning. They are the predictable output of a nervous system that cannot regulate itself, and an immune system that cannot stand down — both governed by structures that pass directly through the corridor at the top of the neck.
The Head-Neck Junction as a Structural Driver of Health
The craniocervical junction is one of the most mechanically demanding and biologically important regions in the human body. Within a space measured in millimeters, the brainstem transitions into the spinal cord, the vertebral arteries supply the brainstem with blood, the internal jugular veins drain the cranial vault, the cerebrospinal fluid moves between the brain and the spinal canal, and the vagus nerve begins its long descent to every major organ in the body. This is not a region that simply supports the head. It is a region that governs much of what makes you feel well or unwell on any given day.
The atlas (C1) sits at the foundation of this corridor. It is the only vertebra without a disc above or below it. It bears the full weight of the head and depends on a delicate balance of ligaments and small muscles to remain properly aligned. When the atlas is in its ideal position, the structures passing through the craniocervical junction operate freely. The brainstem is not under mechanical stress. The vagus nerve is not mechanically irritated. The vascular and CSF pathways drain as designed. The autonomic nervous system has the structural conditions it needs to regulate itself, which means the immune system has the structural conditions it needs to stay calibrated.
When the atlas is misaligned — even by fractions of a millimeter — that entire equation changes. The brainstem encounters sustained mechanical stress. The vagus nerve becomes irritated as it descends. The vascular and CSF outflow pathways are partially restricted, allowing inflammatory waste to accumulate in tissues that should be clearing it. The deep neck muscles hold sustained, asymmetric contractions that compress the surrounding soft tissue corridor. The autonomic nervous system loses its balance, the cholinergic anti-inflammatory pathway is impaired, and the immune system is left without the off switch it needs.
In a healthy body that has not faced a major immune challenge, this kind of upper cervical dysfunction can produce a slow, low-grade dysregulation that the body usually compensates for. In a body recovering from a significant viral insult — like SARS-CoV-2 — that compensation often fails. The structural problem that was previously manageable becomes the missing piece that prevents recovery. The infection has cleared, but the conditions for the body to fully reset are not in place, and the inflammatory state persists.
How Neckwise Evaluates Long COVID Patients
The Neckwise process is built around objectivity. We do not guess at whether a misalignment is present and we do not adjust based on how the neck feels to the touch. We measure.
The evaluation begins with a comprehensive consultation and history. We listen for the timeline of the long COVID symptoms, the pattern of associated complaints, prior trauma to the head or neck (including events that may have predated the infection by years), and the full constellation of autonomic and inflammatory signs. From there, we use objective testing — including a leg balance test and infrared thermography — to determine whether the nervous system is showing measurable signs of upper cervical involvement. These screens are repeatable, evidence-based, and tell us whether the upper cervical spine is part of the picture.
Related article

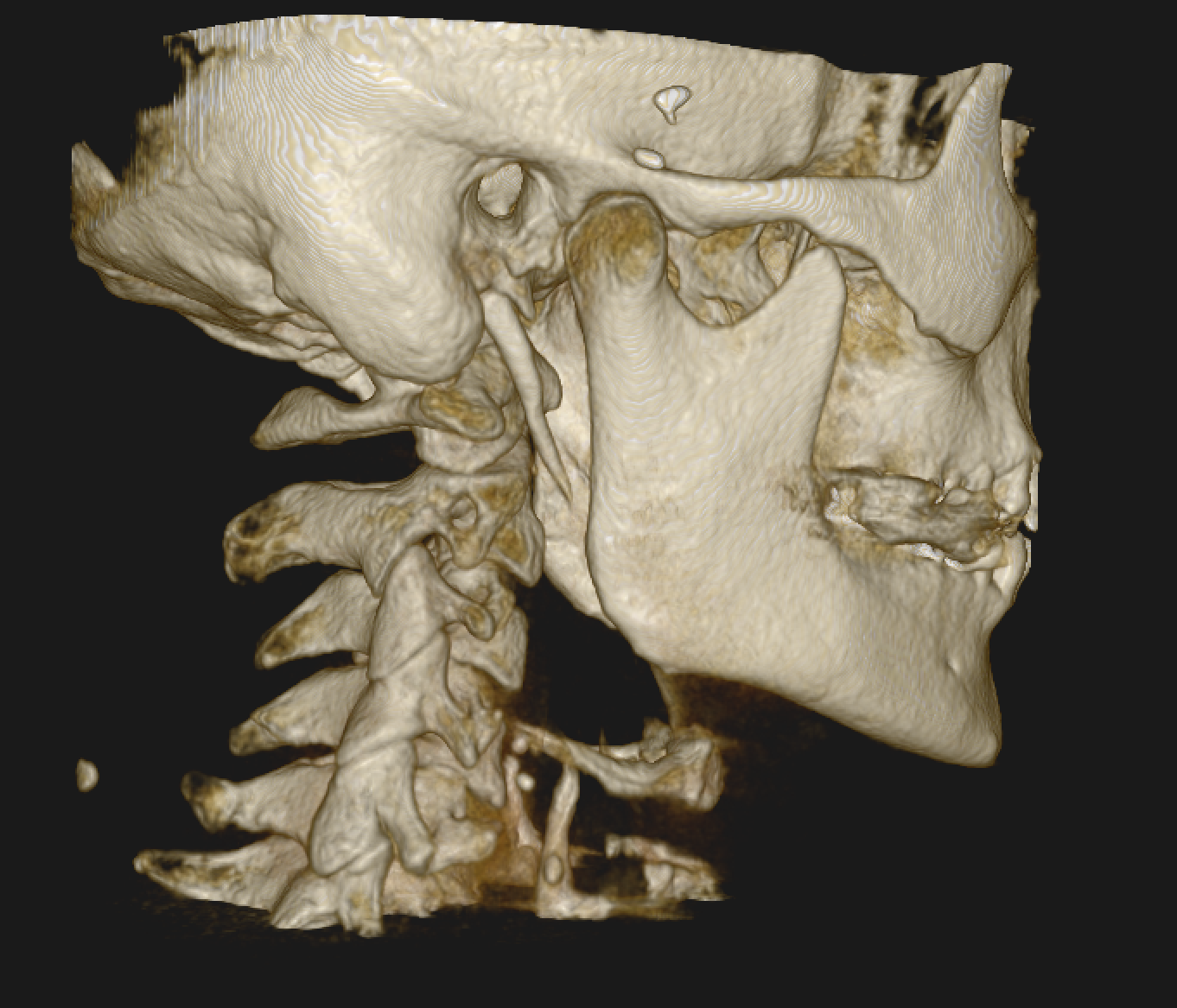
If the screens point toward upper cervical involvement, we move to imaging. Neckwise uses CBCT 3D imaging as a precision tool to visualize the atlas and axis in three dimensions. Unlike a flat X-ray, CBCT produces a true three-dimensional model of the upper cervical region, and the misalignment is quantified in degrees and millimeters across all axes of motion. This level of precision is critical because the atlas does not misalign in just one direction — it can shift forward or backward, rotate, and tilt in combination, and addressing one component without the others does not fully resolve the underlying mechanical compromise.
The Correction: No Twisting, No Cracking, No Pulling
The Neckwise correction is not what most people picture when they hear the word chiropractic. There is no twisting of the neck, no cracking or popping sound, and no forceful pulling or sudden movement of the head. This matters in general, and it matters even more for long COVID patients — because their nervous system is already in a state of heightened sensitivity, and forceful manipulation in this population can provoke symptom flares rather than provide relief.
Instead, the patient lies on their side on a precisely engineered table. The doctor uses the measurements taken from the CBCT imaging to determine the exact angle and direction needed to guide the atlas back toward its ideal position. The correction is delivered as a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place. The intent is to give the body a precise mechanical input that allows it to release the misalignment on its own terms, so the brainstem, the vagus nerve, and the autonomic nervous system can begin to operate without sustained mechanical stress.
What Recovery Can Look Like
When the upper cervical spine is restored toward its ideal position, several things begin to change in parallel. The brainstem is no longer under sustained mechanical irritation. The vagus nerve has the room it needs to function, which restores the cholinergic anti-inflammatory pathway and gives the immune system its off switch back. The vascular and CSF outflow pathways open, allowing inflammatory waste to clear from tissues that have been holding it. The deep neck muscles that have been holding asymmetric contractions begin to release. The autonomic nervous system has the structural conditions it needs to begin rebalancing.
Patients commonly report that the symptoms begin to shift in steps rather than all at once. Fatigue lifts gradually. Brain fog clears. Post-exertional crashes become less severe and less frequent. Heart rate stabilizes. Sleep deepens. The persistent inflammation begins to recede. The autonomic instability that has defined daily life slowly loses its grip. Healing in long COVID is rarely linear, and progress in chronic inflammatory conditions tends to come in waves, which is why care is structured as a corrective program over weeks to months — long enough for the nervous system to reorganize, the muscles to adapt, and the inflammatory state to resolve.
It is important to be honest about what this approach is and is not. Upper cervical care is not a cure for long COVID, and it is not a replacement for the rest of a patient's care team. The condition is multifactorial, and recovery is rarely the result of any single intervention. What upper cervical care does is address a specific, measurable, mechanical and neurological factor that is consistently overlooked — and for many patients, removing that obstacle is what finally allows the rest of their care to take effect.
Finding Real Answers in Sarasota
If you are living with long COVID and searching for answers in Sarasota, an upper cervical evaluation may be a meaningful next step in your care. The connection between the brainstem, the vagus nerve, the autonomic nervous system, and the immune system is anatomical, measurable, and increasingly well documented. The structural conditions at the head-neck junction influence every one of those systems. When that structural piece is missing from a patient's evaluation, the picture is incomplete by definition.
Neckwise focuses on patients who have not found lasting answers in the conventional system. Objective testing, CBCT 3D imaging, and a precise correction with no twisting, cracking, or pulling offer a structured, evidence-based path to determine whether the upper cervical spine is contributing to your long COVID symptoms — and if it is, to address it at the source so the body has the structural conditions it needs to finally recover.
To learn more or schedule a consultation, contact Neckwise Sarasota. Long COVID is real, the inflammation is real, and the autonomic dysregulation is real. For many patients, the path back to health begins with looking at the corridor that governs all of it — the place where the brainstem meets the spine.



Leave a comment