
How the nervous system regulates immunity, why upper cervical misalignment can disrupt that regulation, and how precision care at the head-neck junction can support the body's recovery from chronic immune-mediated disease.
Autoimmune disease is one of the fastest-growing categories of chronic illness in the modern world. Patients are told that their immune system has turned against their own tissues, that the cause is unknown, and that the standard treatment is to suppress the immune response with medication for the rest of their lives. Those medications can be effective at controlling symptoms, but they share a common limitation. They manage the consequences of immune dysregulation without addressing why the dysregulation began in the first place — or what the body might be capable of when its underlying regulatory systems are functioning properly.
Schedule Your Appointment
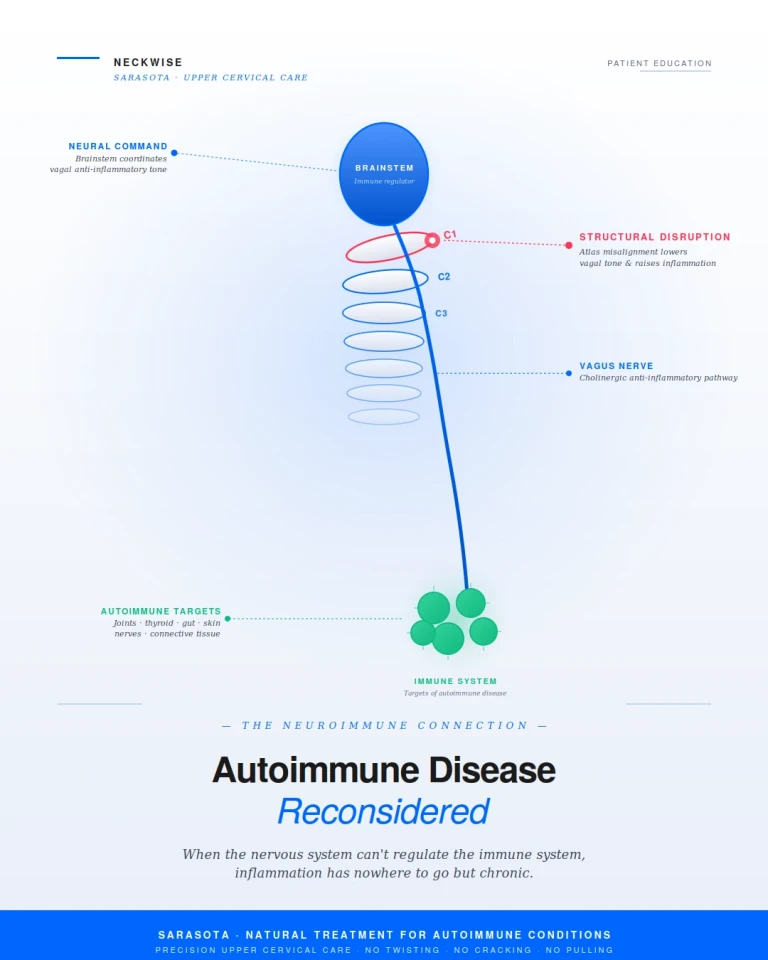
Schedule appointmentAt Neckwise in Sarasota, we focus on a part of the picture that the conventional rheumatology and immunology workup is rarely designed to evaluate. The immune system does not regulate itself in isolation. It is actively coordinated, moment by moment, by the nervous system — and the central regulator of that coordination is the brainstem, which sits inside the upper cervical corridor. When the structural conditions at the head-neck junction are compromised, the brainstem and the autonomic nervous system lose their ability to keep the immune response appropriately calibrated. For a meaningful number of autoimmune patients, this is not a peripheral detail. It is one of the central upstream factors that allows chronic immune dysregulation to take hold in the first place.
This blog walks through the science of neuroimmunology, the specific neural pathways through which the nervous system controls the immune response, why structural problems at the upper cervical spine matter, the autoimmune conditions most consistent with this model, and how precision upper cervical care can support the body's natural recovery process.
Neuroimmunology: The Science Connecting Two Systems Once Thought Separate
For most of medical history, the nervous system and the immune system were studied as independent entities. The nervous system controlled thought, sensation, and movement. The immune system fought infection. They were considered functionally separate, and the diseases of each were treated by different specialties. The last two decades of research have made it clear that this separation is artificial. The nervous system and the immune system are deeply, continuously, and bidirectionally interconnected.
The field of neuroimmunology has emerged specifically to study how these two systems communicate. The findings have been transformative. We now understand that the brain receives constant input from the immune system about inflammation in the body, and that the brain in turn sends regulatory signals back to the immune system that influence how strongly it responds, how long that response lasts, and when it should resolve. The immune system is not autonomous. It is supervised, modulated, and coordinated by the central nervous system in real time.
This understanding has major implications for autoimmune disease. If the immune system is being actively coordinated by the nervous system, then a breakdown in that coordination — not a defect in the immune cells themselves — may be the upstream cause of the chronic, self-targeting inflammation that defines autoimmunity. This is no longer a fringe theory. It is the direction that mainstream neuroimmunology research has been moving for years.
How the Nervous System Controls the Immune System
The most well-characterized pathway through which the nervous system regulates immunity is the cholinergic anti-inflammatory pathway. First described by Kevin Tracey and colleagues in the early 2000s, this pathway operates through the vagus nerve — cranial nerve ten — which emerges from the brainstem at the level of the medulla and travels throughout the body, communicating directly with immune cells in the spleen, gut, lungs, liver, and other organs.
Through the cholinergic anti-inflammatory pathway, the vagus nerve releases acetylcholine, which binds to alpha-7 nicotinic acetylcholine receptors on immune cells and actively suppresses the release of pro-inflammatory cytokines such as TNF-alpha, IL-6, and IL-1 beta. In other words, the vagus nerve functions as a continuous brake on inflammation. When vagal tone is robust, the immune system stays appropriately calibrated. It mounts a response when there is a threat, and it stands down once the threat has been resolved.
Pavlov VA, Tracey KJ. The cholinergic anti-inflammatory pathway. Brain, Behavior, and Immunity. The vagus nerve, through release of acetylcholine acting on alpha-7 nicotinic receptors on macrophages, dampens production of pro-inflammatory cytokines including TNF, IL-6, and IL-1 beta.
When vagal tone is low — when the vagus nerve is not firing strongly enough to provide that continuous anti-inflammatory signal — the immune system loses its off switch. Inflammation that should resolve becomes chronic. Cytokines that should be suppressed continue to circulate. The immune response that should stand down once a threat has cleared instead remains active, and over time, that prolonged activation creates the conditions in which the immune system can begin to target the body's own tissues.
This mechanism has been studied extensively across multiple autoimmune conditions. Research consistently shows that patients with rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease, and other autoimmune diseases have measurably lower vagal tone compared to healthy controls. The reduction in vagal activity has even been shown to precede the onset of clinical disease, suggesting that loss of neural regulation is not just a consequence of autoimmunity — it is part of how autoimmunity begins.
Koopman FA, et al. Vagus nerve stimulation inhibits cytokine production and attenuates disease severity in rheumatoid arthritis. Proceedings of the National Academy of Sciences. Multiple studies have demonstrated that tonic vagus nerve activity is diminished in autoimmune disease, and that reduction in vagal tone precedes the onset of clinical disease.
This is also why vagus nerve stimulation has emerged as a serious clinical intervention for autoimmune disease. The Nature Medicine pivotal trial published in 2025 demonstrated that vagus nerve stimulation produced clinically meaningful improvements in rheumatoid arthritis patients who had not responded to conventional disease-modifying drugs. Similar trials are underway in lupus, Crohn's disease, and systemic sclerosis. The principle is the same in each case: restore neural regulation of the immune system, and the inflammatory state has the conditions it needs to begin resolving.
RESET-RA pivotal randomized controlled trial. Nature Medicine, 2025. Vagus nerve-mediated neuroimmune modulation produced significant ACR20 response in rheumatoid arthritis patients with inadequate response to biologics. Engaging the inflammatory reflex through the vagus nerve led to reduced TNF, IL-6, and IL-1 beta production.
The Brainstem at the Heart of Immune Regulation
The vagus nerve does not generate its anti-inflammatory signal in isolation. It is governed by the brainstem — specifically the dorsal motor nucleus of the vagus and the nucleus tractus solitarius, both located in the medulla. These brainstem nuclei integrate input from the immune system, the cardiovascular system, the gut, and higher brain centers, and they coordinate the autonomic response in real time. When the brainstem is functioning optimally, vagal tone is high, sympathetic and parasympathetic balance is maintained, and the immune system has the regulatory framework it needs to operate within healthy limits.
When the brainstem is under sustained mechanical or chemical stress, that regulatory function degrades. Vagal output decreases. Sympathetic dominance takes over. The cholinergic anti-inflammatory pathway weakens. The body shifts into a chronic fight-or-flight state, and the immune system loses its ability to stand down. This is the neural pattern increasingly documented across autoimmune populations: high sympathetic tone, low parasympathetic tone, and a brainstem operating under conditions of sustained stress.
This is where the structural piece becomes critical. The brainstem does not exist in a protected vacuum. It sits inside the upper cervical corridor, surrounded by the atlas and axis vertebrae, and the mechanical conditions at the craniocervical junction directly influence how the brainstem functions.
How Upper Cervical Misalignment Disrupts the Brainstem

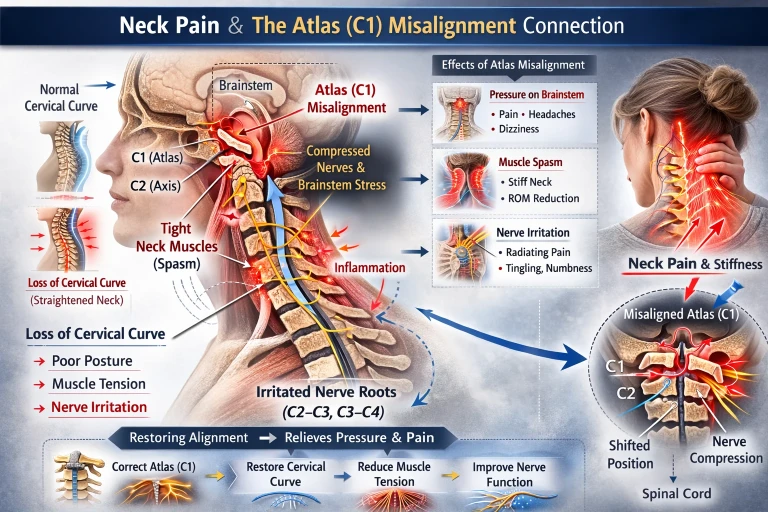
The atlas, or C1, is the topmost vertebra of the spine. It bears the full weight of the head, sits directly beneath the skull, and surrounds the brainstem and the upper portion of the spinal cord. Unlike the rest of the spine, the atlas has no disc above or below it. It depends on a delicate balance of ligaments and small muscles to remain properly aligned. When the atlas is in its ideal position, the structures passing through the craniocervical junction — the brainstem, the vagus nerve as it exits the skull, the vertebral arteries, the internal jugular veins, and the cerebrospinal fluid pathways — all operate in a mechanically clear corridor.
When the atlas shifts even fractions of a millimeter out of its ideal position, the geometry of this entire region changes. The brainstem can be subjected to sustained mechanical stress. The vagus nerve becomes mechanically irritated as it exits the jugular foramen. The arterial inflow to the brainstem and the venous drainage from the cranial vault can be partially compromised. Cerebrospinal fluid that normally circulates freely between the cranial vault and the spinal canal encounters resistance at the foramen magnum. The deep suboccipital muscles, in their attempt to compensate for the misalignment, hold sustained asymmetric contractions that further compress the surrounding soft tissue corridor.
The result is a brainstem operating under conditions it was never designed for, and a cascade of downstream consequences that touch every system the brainstem regulates — autonomic balance, cardiovascular function, sleep, digestion, and most importantly for this discussion, immune coordination.
The clinical implications of this connection have been studied directly. Heart rate variability research has consistently shown that upper cervical adjustments can produce measurable shifts in autonomic balance, increasing parasympathetic activity and improving vagal tone. A randomized cross-over study by Win and colleagues, published in 2015, demonstrated significant improvements in heart rate variability following manipulation of the upper cervical segments specifically, with shifts toward parasympathetic dominance that were not seen with lower cervical interventions.
Win NN, et al. Effects of Upper and Lower Cervical Spinal Manipulative Therapy on Blood Pressure and Heart Rate Variability in Volunteers and Patients With Neck Pain: A Randomized Controlled, Cross-Over, Preliminary Study. Journal of Chiropractic Medicine, 2015. Standard deviation of normal-to-normal R-R intervals increased significantly after upper cervical manipulation, indicating enhanced parasympathetic activity.
Similar findings have been documented in research on atlas-specific corrections and cardiovascular regulation. A randomized controlled trial published in the Journal of Human Hypertension found that a single precise atlas correction produced clinically significant reductions in blood pressure that were sustained over time — an effect the researchers attributed to improved autonomic regulation through the brainstem.
Bakris G, et al. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: a pilot study. Journal of Human Hypertension, 2007. Restoration of atlas alignment was associated with marked and sustained reductions in blood pressure, attributed to improved brainstem-mediated autonomic regulation.
These findings are not proof that upper cervical care cures autoimmune disease. They are proof that the structural conditions at the upper cervical spine measurably influence the autonomic nervous system that, in turn, regulates the immune response. That mechanistic link is real, it is documented in peer-reviewed literature, and it represents a piece of the autoimmune picture that the standard rheumatology workup does not evaluate.
How a Structural Breakdown Can Set the Stage for Autoimmunity
Autoimmune disease is rarely caused by a single factor. The current scientific consensus is that autoimmunity emerges from a combination of genetic predisposition, environmental triggers (such as infections, toxins, or stressors), gut microbiome changes, hormonal influences, and chronic neuroinflammation. The relevant question is not whether upper cervical dysfunction causes autoimmunity in isolation. The relevant question is whether it is one of the upstream factors that creates the conditions in which autoimmunity is more likely to emerge — and harder to resolve once it has begun.
The mechanistic chain is straightforward when laid out. Upper cervical misalignment places sustained mechanical stress on the brainstem. The brainstem's regulation of the autonomic nervous system degrades. Vagal tone decreases and sympathetic tone rises. The cholinergic anti-inflammatory pathway weakens, removing the body's primary brake on inflammation. Pro-inflammatory cytokines circulate at higher baseline levels. Chronic, low-grade systemic inflammation becomes the default state. In a body already carrying genetic susceptibility, environmental triggers, or gut dysbiosis, this loss of neural regulation can be the missing piece that allows the immune system to begin targeting the body's own tissues.
Once autoimmunity has been established, the same mechanism explains why these conditions tend to become chronic and why patients struggle to achieve true remission. The body cannot fully resolve the inflammatory state if the regulatory framework that would normally bring it back to baseline is structurally compromised. Medication can suppress the cytokine cascade, but it cannot restore vagal tone. Diet and lifestyle changes can address some of the contributing factors, but they cannot address a brainstem operating under sustained mechanical stress. This is why so many autoimmune patients describe their condition as managed but never resolved — the upstream regulatory system is still not working the way it was designed to.
Common Autoimmune Conditions Where This Connection Matters
There are over a hundred recognized autoimmune diseases, and the underlying neuroimmune mechanism applies to most of them in some form. The conditions below are among the most common and the most consistently associated with autonomic dysregulation, low vagal tone, and the kind of chronic neuroinflammation that upper cervical care is positioned to address. The presence of one of these diagnoses does not guarantee that upper cervical dysfunction is contributing — but for many patients with these conditions, especially those who have not achieved lasting relief through conventional care, it deserves a serious look.
• Rheumatoid arthritis — chronic synovial inflammation with documented reductions in vagal tone preceding clinical onset, now an active target of vagus nerve stimulation therapy
To listen to one of our patients recovery from rheumatoid arthritis click here.
• Systemic lupus erythematosus (SLE) — multi-system autoimmune disease with measurable autonomic dysregulation and a growing body of research on neuroimmune intervention
• Hashimoto's thyroiditis — autoimmune destruction of the thyroid gland, frequently associated with broader autonomic dysfunction and chronic systemic inflammation
• Graves' disease — autoimmune hyperthyroidism, often coexisting with sympathetic overactivity that mirrors the autonomic pattern of upper cervical dysfunction
• Multiple sclerosis (MS) — autoimmune demyelinating disease with strong neuroinflammatory components and well-documented autonomic involvement
• Crohn's disease and ulcerative colitis (IBD) — inflammatory bowel diseases now subjects of active vagus nerve stimulation clinical trials due to the strong vagal-immune connection in the gut

• Celiac disease — autoimmune reaction to gluten with extensive systemic and neurological manifestations beyond the gut
• Psoriasis and psoriatic arthritis — chronic inflammatory skin and joint conditions with strong autonomic and neurogenic components
• Sjogren's syndrome — autoimmune destruction of moisture-producing glands, frequently accompanied by autonomic dysregulation and chronic fatigue
• Type 1 diabetes — autoimmune destruction of pancreatic beta cells, increasingly studied in the context of neuroimmune regulation
• Fibromyalgia — though debated as a true autoimmune condition, it shares the neuroinflammatory and autonomic patterns characteristic of immune dysregulation
• Chronic fatigue syndrome (ME/CFS) and post-viral autoimmune syndromes — including the long COVID population now being evaluated through the same neuroimmune lens
This list is not exhaustive, but it represents the conditions for which the underlying connection between the nervous system, the immune system, and the upper cervical spine has the strongest mechanistic and clinical relevance.
Common Symptoms That Cross Conditions
Patients with autoimmune disease often describe symptom patterns that extend well beyond the disease's hallmark features. Many of these shared symptoms point directly back to autonomic dysregulation and chronic neuroinflammation rather than to the autoimmune target tissue itself. Common patterns include:
• Persistent fatigue that is not relieved by rest
• Brain fog, difficulty concentrating, and word-finding problems
• Sleep disturbance and unrefreshing sleep
• Heat or cold intolerance and temperature dysregulation
• Digestive issues — bloating, motility changes, food sensitivities
• Heart palpitations, lightheadedness on standing, or other signs of dysautonomia
• Chronic muscle pain, joint pain, and stiffness beyond the primary disease
• Headaches and migraines
• Mood symptoms, anxiety, and a sense of being in fight-or-flight
• Neck pain, neck stiffness, and tension at the base of the skull
• Heightened sensitivity to stress, light, sound, and exertion
The presence of these symptoms — and especially the presence of cervical and autonomic symptoms alongside the primary autoimmune diagnosis — is one of the strongest signals that the upper cervical spine deserves evaluation.
How Neckwise Evaluates Autoimmune Patients
Related article
Neck pain relief in Sarasota, Bradenton, and Lakewood Ranch| Upper Cervical Chiropractor near me
Mar 07, 2026
The Neckwise process is built around objectivity. We do not guess at whether a misalignment is present, and we do not adjust based on how the neck feels to the touch. We measure.
The evaluation begins with a comprehensive consultation and history, with particular attention to the timeline of the autoimmune diagnosis, the pattern of associated autonomic symptoms, prior trauma to the head or neck (including events that may have predated the autoimmune diagnosis by years or decades), and the full picture of how the nervous system is currently functioning. From there, we use objective testing — including a leg balance test and infrared thermography — to determine whether the nervous system is showing measurable signs of upper cervical involvement. These screens are repeatable and evidence-based, and they tell us with confidence whether the upper cervical spine is part of the picture.
If the screens point toward upper cervical involvement, we move to imaging. Neckwise uses CBCT (cone beam computed tomography) 3D imaging as a precision tool to visualize the atlas and axis in three dimensions. Unlike a flat X-ray, CBCT produces a true three-dimensional model of the upper cervical region, and the misalignment is quantified in degrees and millimeters across all axes of motion. This level of precision is essential because the atlas does not misalign in just one direction. It can shift forward or backward, rotate, and tilt — often in combination — and addressing one component without the others does not fully resolve the underlying mechanical compromise.
Precision Correction with No Twisting, Cracking, or Pulling
The Neckwise correction is not what most people picture when they hear the word chiropractic. There is no twisting of the neck, no cracking or popping sound, and no forceful pulling or sudden movement of the head. This matters in general, and it matters even more for patients with autoimmune disease — because the autonomic nervous system in this population is already in a state of heightened sensitivity and dysregulation, and forceful manipulation can provoke flares rather than provide relief.
Instead, the patient lies on their side on a precisely engineered table. The doctor uses the measurements taken from the CBCT imaging to determine the exact angle and direction needed to guide the atlas back toward its ideal position. The correction is delivered as a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place. The intent is to give the body a precise mechanical input that allows it to release the misalignment on its own terms.
The goal of care is not a single dramatic adjustment. The goal is for the upper cervical spine to learn to hold its corrected position, so that the brainstem and central nervous system can operate without sustained mechanical stress over time. Healing in autoimmune conditions is rarely linear, and progress in chronic immune-mediated disease tends to come in waves rather than in a single step. Care is structured as a corrective program over weeks to months precisely because the nervous system needs sustained time to reorganize, the muscles and ligaments need time to adapt to the new position, and the inflammatory state needs time to resolve.
What Recovery Can Look Like
When the upper cervical spine is restored toward its ideal position and learns to hold that position, several changes begin to occur in parallel. The brainstem is no longer under sustained mechanical irritation. The vagus nerve has the room it needs to function, which restores the cholinergic anti-inflammatory pathway and gives the immune system its primary off switch back. Vagal tone improves. Sympathetic and parasympathetic balance shifts back toward equilibrium. The chronic, low-grade systemic inflammation that has been the default state begins to ease. The autonomic instability that has defined daily life slowly loses its grip.
Patients commonly report that the symptoms shift in steps rather than all at once. Energy returns gradually. Brain fog clears. Sleep deepens. Digestive symptoms ease. Joint pain and stiffness become less intense and less frequent. Flares become shorter and less severe. The associated symptoms that travel with autoimmune disease — anxiety, palpitations, light sensitivity, fatigue — often improve in parallel because they share the same upstream regulatory cause.
It is important to be honest about what this approach is and is not. Upper cervical care is not a cure for autoimmune disease, and it is not a replacement for the rest of a patient's care team. Autoimmune disease is multifactorial, and recovery rarely results from any single intervention. What upper cervical care does is address a specific, measurable, structural and neurological factor that is consistently overlooked — one that the peer-reviewed literature increasingly supports as central to immune regulation. For many patients, restoring this piece of the picture is what finally allows the rest of their care — medication, diet, lifestyle, gut health, stress management — to take full effect.
Finding Natural Treatment and Relief for Autoimmune Conditions in Sarasota
If you are living with an autoimmune condition and searching for natural treatment and relief in Sarasota, an upper cervical evaluation may be a meaningful next step in your care. The connection between the brainstem, the vagus nerve, the autonomic nervous system, and the immune system is anatomical, measurable, and well-documented in modern neuroimmunology research. The structural conditions at the head-neck junction influence every one of those systems. When that structural piece is missing from a patient's evaluation, the picture is incomplete by definition.
Neckwise focuses on patients who have not found lasting answers in the conventional system. Objective testing, CBCT 3D imaging, and a precise correction with no twisting, cracking, or pulling offer a structured, evidence-based path to determine whether the upper cervical spine is contributing to your autoimmune condition — and if it is, to address it at the source so the body has the structural conditions it needs to support recovery. The goal is for the neck to hold its corrected position over time, so that the brainstem and central nervous system can do what they were designed to do: regulate, calibrate, and protect.
To learn more or schedule a consultation, contact Neckwise Sarasota. Autoimmune disease is real, the inflammation is real, and the dysregulation is real. The science behind the brain-immune connection is no longer theoretical — it is the direction modern medicine is moving. For many patients, the path back toward health begins with looking at the corridor that governs the entire system: the place where the brainstem meets the spine.
Selected References
Pavlov VA, Tracey KJ. The cholinergic anti-inflammatory pathway. Brain, Behavior, and Immunity. Foundational review of the vagus-mediated regulation of inflammation through alpha-7 nicotinic acetylcholine receptors.
Koopman FA, et al. Vagus nerve stimulation inhibits cytokine production and attenuates disease severity in rheumatoid arthritis. Proceedings of the National Academy of Sciences. Demonstrated clinical efficacy of vagus nerve stimulation in autoimmune disease.
RESET-RA pivotal randomized controlled trial. Nature Medicine, 2025. Vagus nerve-mediated neuroimmune modulation produced significant improvements in patients with rheumatoid arthritis who had inadequate response to biologics.
Das UN. Can vagus nerve stimulation halt or ameliorate rheumatoid arthritis and lupus? Lipids in Health and Disease, 2011. Review of subnormal vagal tone and elevated sympathetic activity across autoimmune inflammatory conditions.
Win NN, et al. Effects of Upper and Lower Cervical Spinal Manipulative Therapy on Blood Pressure and Heart Rate Variability. Journal of Chiropractic Medicine, 2015. Demonstrated parasympathetic shifts following upper cervical manipulation.
Bakris G, et al. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients. Journal of Human Hypertension, 2007. Documented sustained blood pressure reduction following precise atlas correction.
Welch A, Boone R. Sympathetic and parasympathetic responses to specific diversified adjustments to chiropractic vertebral subluxations of the cervical and thoracic spine. Journal of Chiropractic Medicine. Heart rate variability research on autonomic responses to spinal adjustment.
Han R, et al. Cholinergic reflex control of inflammation: mechanistic and translational advances in transcutaneous auricular vagus nerve stimulation across rheumatic, metabolic, and postoperative disorders. Frontiers in Immunology, 2026. Recent comprehensive review of the neuroimmune interface in autoimmune disease.



Leave a comment