
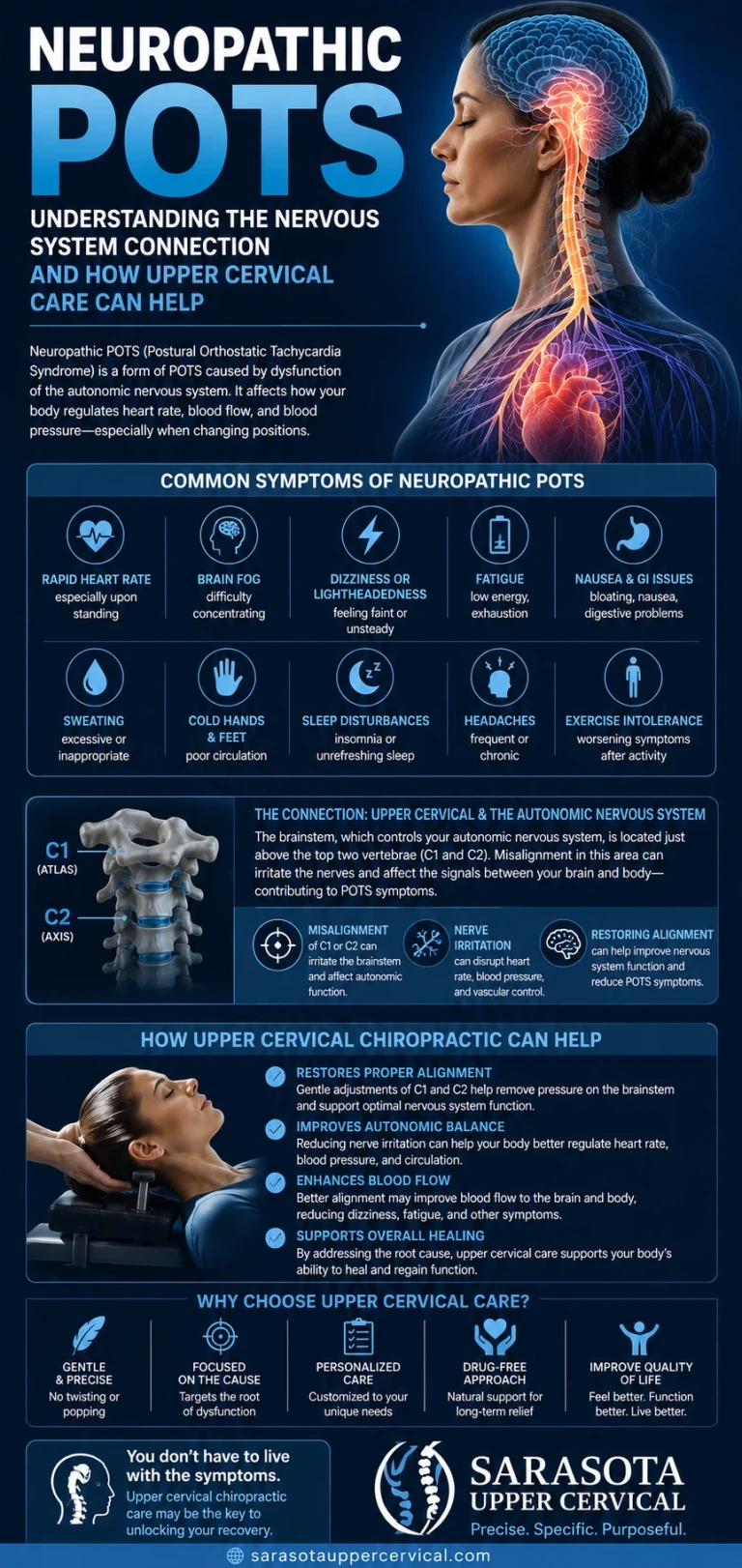
Not everyone with POTS has the same POTS. Some patients run hot, anxious, and tremoring with sky-high standing adrenaline. Others feel drained, heavy-legged, and cold, with blue-tinged feet and gut symptoms that flare after meals. This second pattern points toward a distinct, well-documented subtype: neuropathic POTS, driven not by an overactive nervous system but by damage to the smallest nerve fibers in the body. This guide explains what neuropathic POTS is, how it differs from the sympathetic-overdrive picture covered in our article on hyperadrenergic POTS, and where the upper cervical spine and brainstem plausibly enter a condition whose root cause sits mostly in the periphery.
What Makes Neuropathic POTS Different
In tertiary referral studies, somewhere between a third and half of POTS patients show evidence of a partial peripheral autonomic neuropathy, most pronounced in the legs. This is called neuropathic POTS, and the underlying problem is damage to small, unmyelinated and thinly myelinated nerve fibers, the same fibers responsible for pain and temperature sensation, sweating, and the fine-tuned constriction of blood vessels in the skin and lower body.
Schedule Your Appointment
Schedule appointmentBecause these fibers fail in a length-dependent pattern, meaning the longest nerves are affected first, the legs and feet bear the brunt of the damage. When someone with neuropathic POTS stands up, the blood vessels in their legs can't constrict properly to push blood back toward the heart and brain. Blood pools in the lower body, venous return drops, and the heart compensates the only way it can: by beating faster.
Recognizing the Neuropathic Pattern
Neuropathic POTS tends to carry a distinct symptom fingerprint, separate from the hyperadrenergic picture:
Acrocyanosis — the feet turning blue or purple on standing, a visible sign of blood pooling and poor venous return
Patchy loss of sweating in the legs (anhidrosis), detectable on specialized testing such as QSART or a thermoregulatory sweat test
Related article
When You Feel Like You Are Still on a Boat: MdDS Relief and treatment in Sarasota
May 19, 2026
Burning, tingling, numbness, or electric-shock sensations in the hands and feet, direct symptoms of small fiber damage
Heat intolerance, since heat causes further vasodilation and worsens the pooling problem
Gastrointestinal symptoms after eating, particularly larger or high-carbohydrate meals, reflecting denervation of the enteric nervous system and a diversion of blood to the digestive tract that the body can no longer compensate for
Profound, heavy fatigue, often described differently than the anxious, wired fatigue reported in hyperadrenergic presentations
On testing, neuropathic POTS is associated with reduced norepinephrine spillover specifically from the legs, abnormal sweat testing, and, in some research settings, reduced intraepidermal nerve fiber density on skin biopsy, direct histological evidence of small fiber loss. It's worth noting these subtypes are not always neatly separate: research has found that a neuropathic POTS patient often develops hyperadrenergic features over time, as the brain increases sympathetic drive to compensate for the peripheral nerve failure. That overlap matters, and it's where the upper cervical conversation becomes relevant.
Where the Brainstem Fits Into a Peripheral Problem
To be direct from the outset: the primary lesion in neuropathic POTS is peripheral, in the small nerve fibers themselves, not in the brainstem or upper cervical spine. Upper cervical care does not repair damaged peripheral nerve fibers and does not reverse small fiber neuropathy. That said, two mechanisms are worth understanding.
The compensatory sympathetic overlay
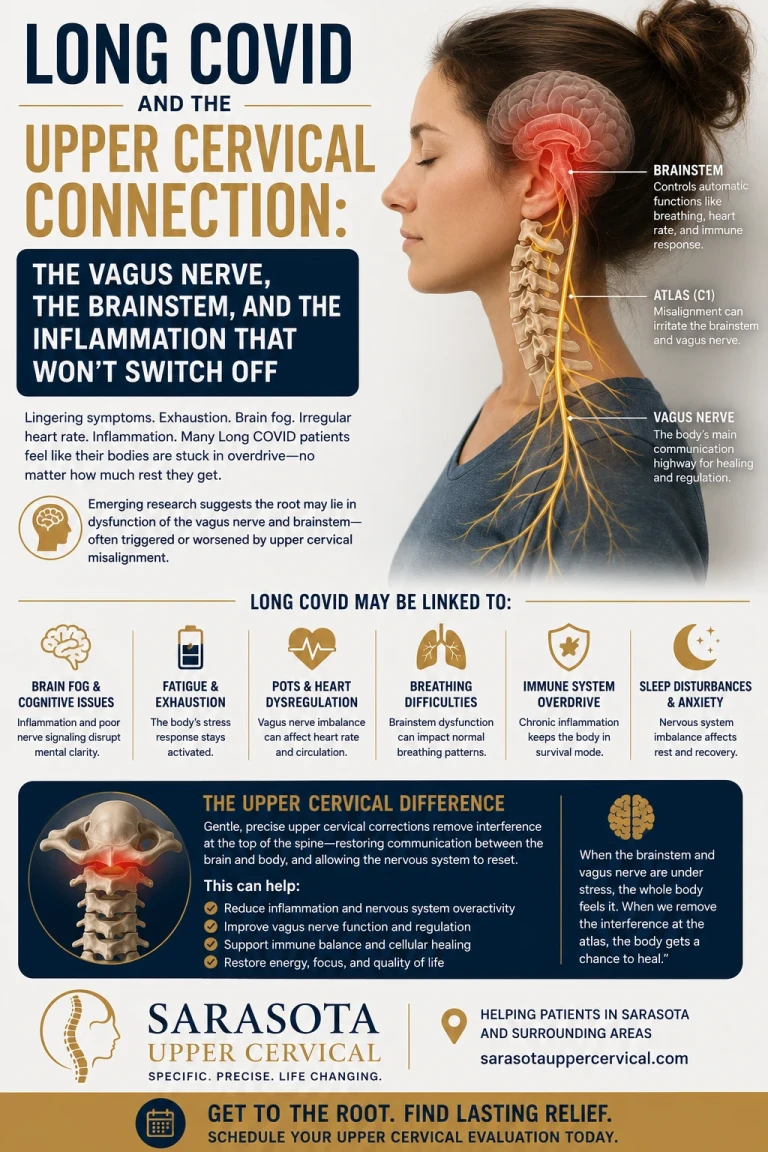
Because the brainstem's cardiovascular control centers, including regions in the medulla oblongata, are what actually drive the compensatory increase in sympathetic outflow when peripheral vasoconstriction fails, the degree to which a person develops secondary hyperadrenergic symptoms on top of their neuropathic baseline may relate to how well this brainstem sympathetic control system itself is functioning. If the craniocervical junction, the area directly beneath the brainstem formed by the atlas (C1) and axis (C2), is mechanically compromised, it may add irritation to the very system now being asked to compensate harder than normal.
Proprioceptive aberrancy and altered sensory input
The upper cervical spine contains an unusually high density of proprioceptive nerve receptors constantly reporting head and neck position to the brainstem. When the atlas is misaligned, this sensory input can become distorted, a phenomenon sometimes called dysafferentation. Distorted input reaching a brainstem that is already working overtime to manage a failing peripheral vasoconstriction system is not a favorable combination, even though it does not address the underlying nerve fiber damage itself.
The myodural bridge and general brainstem irritation
The deep suboccipital muscles at the base of the skull connect directly to the dura mater surrounding the brainstem through connective tissue bridges called myodural bridges. Chronic tension or dysfunction in this region, often following whiplash, concussion, or repetitive postural stress, may contribute a low-grade mechanical irritation to the brainstem's cardiovascular and autonomic centers, layered on top of, not instead of, the peripheral small fiber problem driving the underlying condition.
What Atlas Correction May and May Not Do Here
Upper cervical chiropractic does not treat, cure, or reverse neuropathic POTS, and it does not regenerate damaged small nerve fibers. What a focused upper cervical evaluation addresses is the mechanical environment of the craniocervical junction: atlas and axis alignment, and the proprioceptive and brainstem-level input that environment generates. For some patients, particularly those whose neuropathic POTS has developed a significant secondary hyperadrenergic overlay, or who have a clear history of neck trauma, addressing that mechanical layer may help reduce additional autonomic strain, working alongside, not in place of, medical management of the underlying neuropathy.
Questions and Answers
Related article
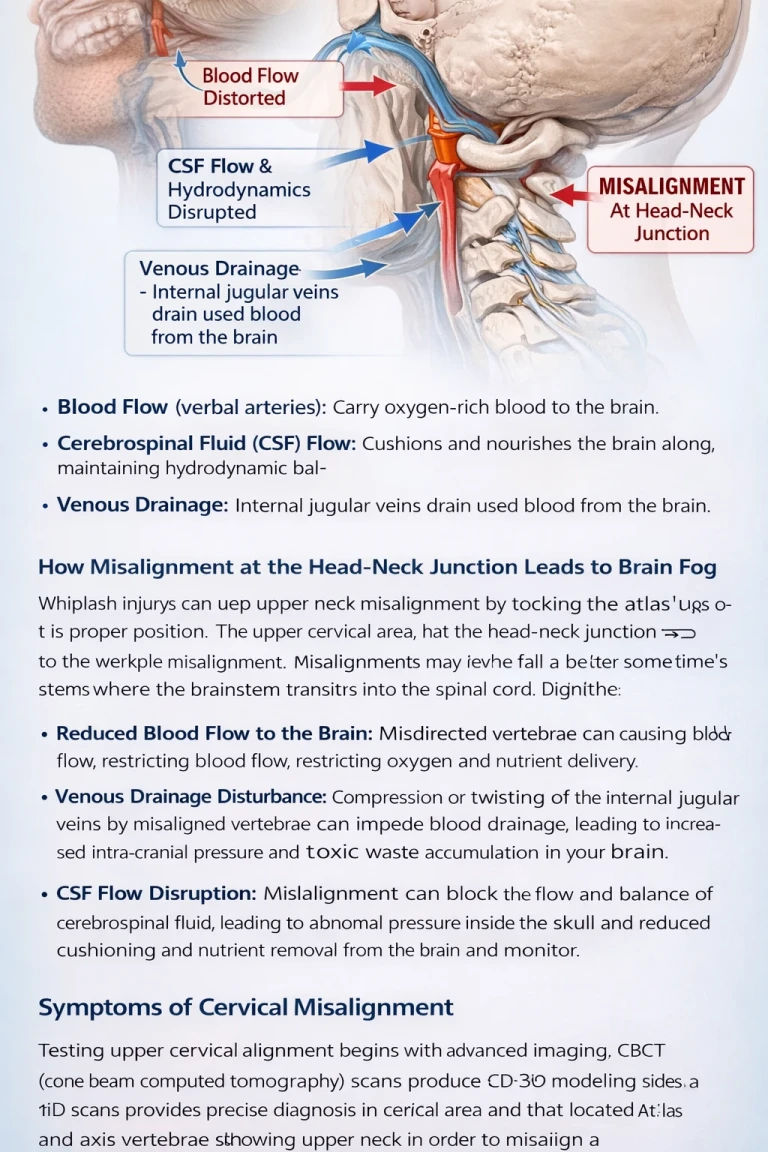
Brain Fog Might Be Coming From an Upper Neck Misalignment | Brain Fog Relief Sarasota
Mar 22, 2026
What percentage of POTS patients have the neuropathic subtype?
Studies from tertiary referral centers estimate that roughly a third to half of POTS patients show evidence of a partial peripheral autonomic neuropathy consistent with neuropathic POTS, though exact figures vary by study population and testing method.
How is neuropathic POTS diagnosed?
Testing may include QSART or a thermoregulatory sweat test to detect patchy sweating loss, measurement of norepinephrine levels specifically from the legs, and in some cases a skin biopsy to assess intraepidermal nerve fiber density directly.
Can someone have both neuropathic and hyperadrenergic POTS?
Yes. Research has found that neuropathic POTS patients often develop secondary hyperadrenergic features as the brain increases sympathetic output to compensate for failing peripheral vasoconstriction. The subtypes frequently overlap rather than existing as entirely separate conditions.
Does upper cervical chiropractic treat small fiber neuropathy?
Upper CervicalCare in this area focuses on the biomechanics of the craniocervical junction, which may influence the brainstem-level compensatory response layered on top of the underlying peripheral nerve damage.
Why do the feet turn blue in neuropathic POTS?
This is called acrocyanosis, and it results from blood pooling in the lower legs when damaged small nerve fibers fail to trigger proper vasoconstriction on standing. It's considered a distinguishing clinical sign of the neuropathic subtype.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Neuropathic POTS is a medical condition that must be diagnosed and managed by qualified medical professionals. Upper cervical chiropractic does not treat, correct, or cure neuropathic POTS, small fiber neuropathy, or any POTS subtype, and is intended only to address the biomechanics of the craniocervical junction as a complement to medical care. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization is made or implied. Individual results vary, and no specific outcome is guaranteed. Always consult your physician or autonomic specialist regarding diagnosis and treatment of POTS or any neurological or autonomic symptoms.



Leave a comment