
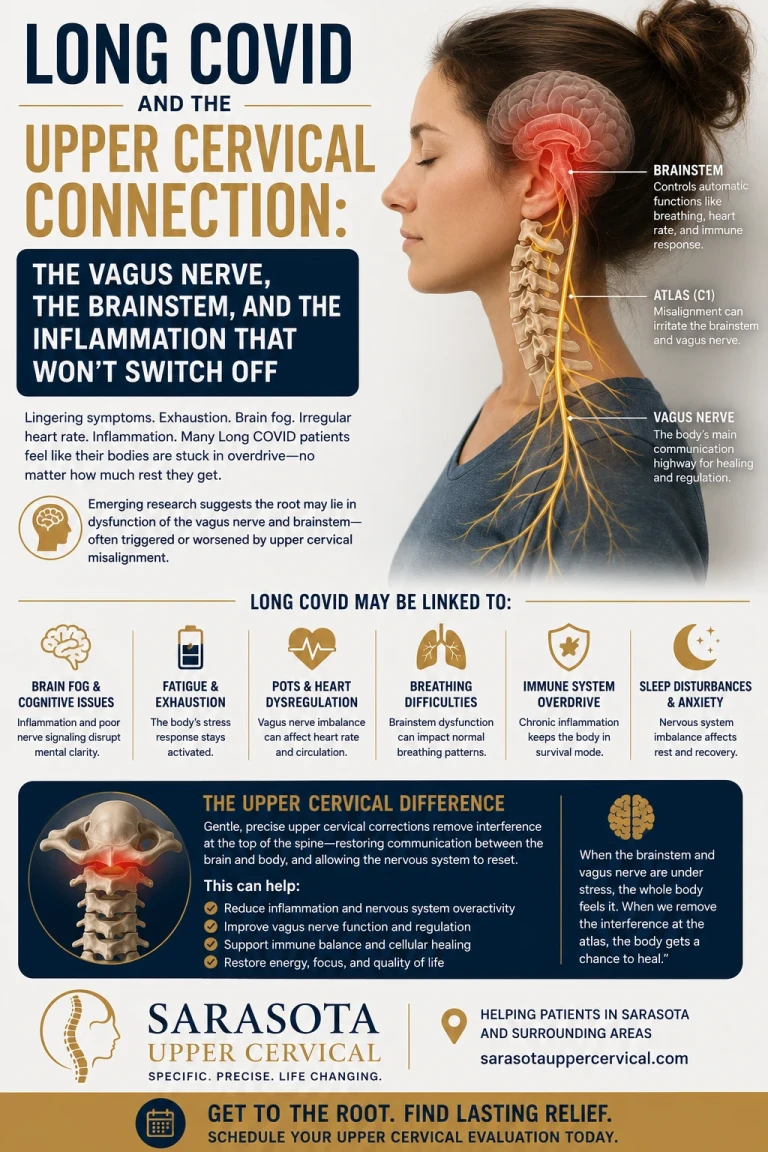
Months after the infection cleared, the symptoms remain: crushing fatigue, brain fog, a racing heart when you stand, poor sleep, and a body that feels like it's stuck in a state of alarm. Long COVID is real, it's neurological as much as it is immunological, and a growing body of research points to a single unifying thread — a disruption in the nervous system's ability to switch off inflammation. At the center of that thread sits the vagus nerve and the brainstem it emerges from. And the brainstem's mechanical environment is governed, in part, by the upper cervical spine.
This article is a deep look at the neuroimmunology of Long COVID, how the infection can leave the body unable to resolve its own inflammatory response, and where the upper cervical spine fits into that picture. To be clear from the outset: Long COVID is a serious medical condition that belongs under the care of qualified physicians. Upper cervical chiropractic does not treat the virus, cure Long COVID, or replace medical care. What it focuses on is one mechanical contributor to the system that's struggling to recover — the brainstem-and-autonomic environment at the top of the neck.
Schedule Your Appointment
Schedule appointmentThe core problem in Long COVID: inflammation that never resolves
A healthy immune response has two halves: an on switch that mounts inflammation to fight a threat, and an off switch that resolves it once the threat is gone. In acute COVID-19, the danger is a runaway on-switch — the "cytokine storm," an abrupt and intense inflammatory response that drives much of the damage. In Long COVID, the emerging picture is different but related: the off switch doesn't work properly. The body can't fully resolve the inflammatory state and return to balance.
Researchers describe Long COVID as arising from sustained inflammatory and neurological dysregulation — persistent fatigue, cognitive impairment, and autonomic dysfunction following the acute infection. The key word is sustained. Something is keeping the system from standing down. To understand what, you have to look at how the body switches inflammation off in the first place — and that mechanism runs through the vagus nerve.
The vagus nerve is the body's master off-switch for inflammation
Most people know the vagus nerve as the "rest and digest" nerve. Far fewer know that it is also the physical wiring of the immune system's off-switch — a circuit called the cholinergic anti-inflammatory pathway.
Here's how the circuit works. The vagus nerve is a two-way cable between the body and the brainstem. Its sensory (afferent) fibers constantly report the body's inflammatory status upward: receptors on afferent vagal fibers feeding into the nucleus tractus solitarius provide the brain with sensory input about the inflammatory status of peripheral tissues. When the brainstem registers rising inflammation, it fires back down the vagus's motor fibers, releasing acetylcholine that binds to receptors (α7-nicotinic receptors) on immune cells — and tells them to stop producing inflammatory cytokines. It is a reflex: inflammation up, vagal brake down, inflammation resolved. This reflex is the reason a healthy nervous system can adapt to an insult, contain it, and recover.
The central concept: Inflammation is supposed to be self-limiting. The vagus nerve, working through the brainstem, is the reflex that applies the brakes. If that reflex is impaired, inflammation loses its off-switch — and the body stays stuck in the alarm state that defines so much of Long COVID.
How COVID disrupts the off-switch — the neuroimmunology
This is where Long COVID becomes a nervous-system disease, not just an immune one. The research points to the virus interfering with the vagal anti-inflammatory reflex at multiple points along its path.
Related article
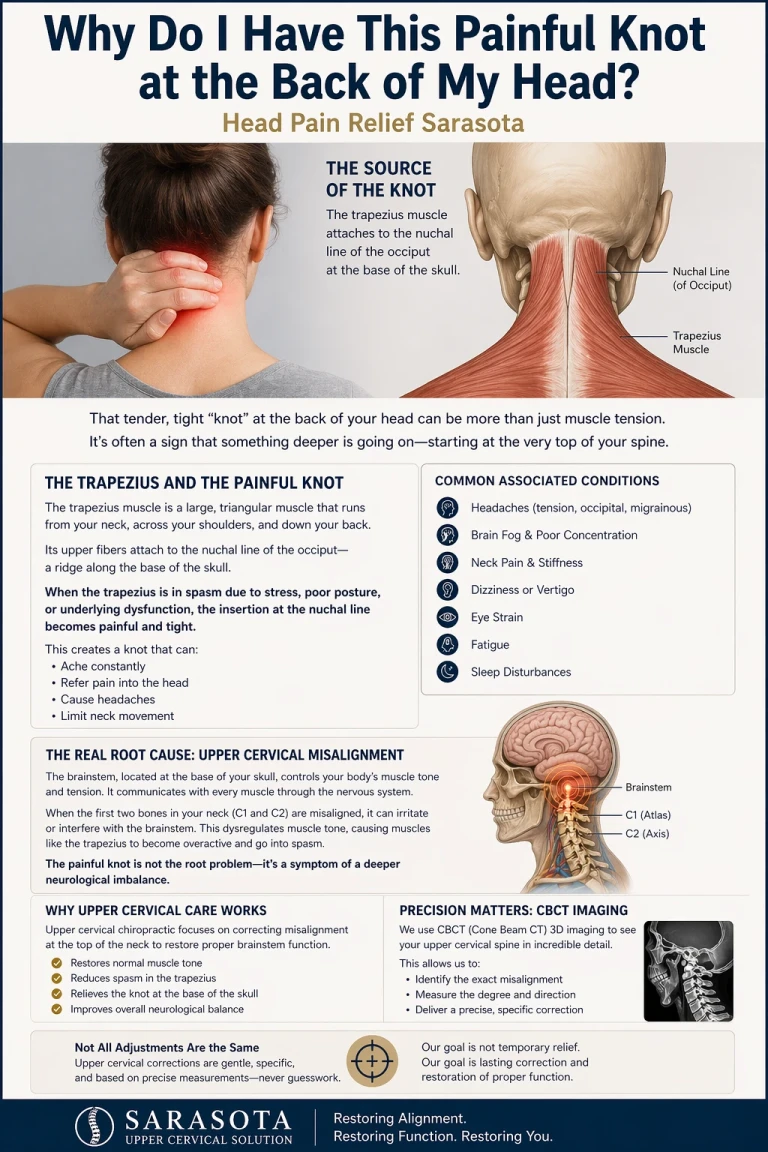
Why do I have this painful knot at the back of my head | Head Pain relief sarasota
Apr 23, 2026First, the route. The SARS-CoV-2 virus is prone to neuroinvading via the lung along the vagus nerve up to the brainstem autonomic centers, traveling the very cable that's supposed to carry the anti-inflammatory signal, up to the very control room that generates it. Second, the receptor. Analyses describe how the spike protein can interfere with the nicotinic acetylcholine receptors that the vagal off-switch depends on, blunting the pathway. The result, as one review frames it, is that cholinergic dysfunction, together with disruption of these receptors, drives hyperinflammation — and proinflammatory cytokines cross the blood-brain barrier, inhibiting the central anti-inflammatory response and producing neuroinflammation.
Now the loop becomes vicious. A weakened vagal brake lets inflammation run higher; the higher inflammation crosses into the brain and further impairs the brainstem centers that run the brake; the more impaired the brake, the higher the inflammation. The system can't adapt its way out. Researchers have connected this to a broader vagus-nerve–HPA-axis–mitochondrial dysfunction, in which suppression of the stress-hormone (cortisol) reflex impairs regulation of both innate and adaptive immunity — meaning the body's chemical anti-inflammatory backup is compromised at the same time as the neural one. Two off-switches, both jammed.
This is precisely the mechanism you feel as Long COVID: an autonomic nervous system stuck in sympathetic ("fight or flight") dominance with a weak parasympathetic brake. It's measurable, too — reduced heart rate variability (HRV), a direct readout of vagal tone, is a hallmark. Studies of post-COVID patients found sustained sympathetic dominance and diminished vagal cardiac modulation in the weeks after infection, and chronically low HRV correlates with increased inflammation, autonomic dysfunction, pain, and post-exertional malaise across many conditions, including long COVID. Low vagal tone is the fingerprint of a body that can't switch its inflammation off.
Why the brainstem — and the upper cervical spine — matters
Every part of this reflex passes through the brainstem. The sensory report arrives there (nucleus tractus solitarius); the motor command leaves from there (dorsal motor nucleus of the vagus); the integration happens there. If the brainstem environment is compromised, the whole cholinergic anti-inflammatory reflex is compromised — regardless of how healthy the rest of the vagus nerve is.
And the brainstem does not sit in isolation. It occupies the craniocervical junction — the space enclosed by the skull and the top two vertebrae of the neck, the atlas (C1) and axis (C2). This is the most neurologically dense, mechanically complex region of the spine, and the vagus nerve exits the skull immediately adjacent to it. When the upper cervical spine is misaligned — commonly after whiplash, head trauma, or the physical stress of prolonged illness — it can create mechanical irritation and altered proprioceptive input at exactly the level where the vagus emerges and the brainstem regulates autonomic function.
The proposed connection is this: an irritated, mechanically stressed brainstem environment may further impair an already-struggling vagal off-switch, making it even harder for the body to down-regulate the inflammatory state left behind by COVID and return to balance. Upper cervical care doesn't touch the virus or the immune cells. It focuses on restoring normal mechanical alignment and input at the craniocervical junction, with the aim of removing one source of interference from the brainstem-and-vagus system that has to do the recovering.
What the vagus nerve research suggests
The strongest external evidence that the vagus is central to Long COVID comes from studies that deliberately stimulate it. Vagus nerve stimulation (VNS) is being actively investigated, and the rationale maps exactly onto the mechanism above: preliminary evidence from small pilot studies suggests VNS may attenuate systemic inflammation by activating the cholinergic anti-inflammatory pathway, restoring autonomic balance and easing symptoms such as fatigue, cognitive dysfunction, and anxiety.

Early trials are encouraging while still preliminary. A 2024 trial of non-invasive vagal stimulation in long-COVID patients reported significant improvements in cognition, anxiety, depression, and sleep that were maintained or improved at one-month follow-up, with fatigue improvements reaching significance a month after the trial ended. This matters for the upper cervical conversation not because adjustment is the same as electrical stimulation — it is not, but because it establishes the principle: improving vagal function improves Long COVID symptoms. Anything that supports the brainstem-and-vagus system's ability to do its job is working on the right target. Upper cervical care approaches that same target from a different, mechanical angle — the alignment environment the brainstem and vagus operate within.
Where upper cervical care fits — and its firm limits
Long COVID is complex, serious, and still being understood. It requires medical evaluation and management, and no single intervention is a cure. Upper cervical chiropractic is not a treatment for the SARS-CoV-2 virus, not a cure for Long COVID, and not a substitute for the care of your physician. What it offers is a focus on one contributor the medical workup rarely examines: the mechanical state of the craniocervical junction where the brainstem and vagus nerve reside.
For a patient whose Long COVID includes prominent autonomic features — dysautonomia, POTS-like symptoms, low HRV, the "stuck in fight-or-flight" pattern — and especially one with a history of head or neck trauma, evaluating the upper cervical spine is a reasonable, low-risk avenue to pursue alongside medical care. The goal is not to override the body's healing but to remove a possible source of mechanical interference so the nervous system has the best chance to do what it's designed to do: resolve, adapt, and recover.
Why CBCT imaging matters here
Because any upper cervical correction is precise, the analysis must be precise. We use cone beam computed tomography (CBCT) as a precision measurement tool to see the true three-dimensional position of the atlas and axis, so an assessment is tailored to the individual's anatomy rather than estimated. (CBCT is a measurement and analysis tool; it is not a diagnostic test for Long COVID, which is a clinical medical diagnosis.)
When to seek medical care
Long COVID symptoms should always be evaluated by a physician. Seek prompt medical attention for chest pain, shortness of breath, fainting, severe or worsening heart-rate or blood-pressure changes, new neurological deficits, or any rapidly worsening symptom. Upper cervical care is a complement to medical management of Long COVID, never a replacement — and coordinating with your medical team is essential.
Questions and Answers
Can upper cervical chiropractic cure Long COVID?
No. Long COVID is a serious medical condition with no single cure, and upper cervical chiropractic does not treat the virus or cure the condition. What it focuses on is one mechanical contributor — the alignment of the craniocervical junction where the brainstem and vagus nerve reside. The aim is to reduce a possible source of interference with the nervous system that has to do the recovering, as a complement to medical care, not a replacement for it.

What does the vagus nerve have to do with Long COVID?
The vagus nerve runs the body's main anti-inflammatory reflex, called the cholinergic anti-inflammatory pathway — it senses inflammation and signals immune cells to switch it off. Research suggests SARS-CoV-2 can disrupt this pathway, including by traveling along the vagus to the brainstem and interfering with the receptors the reflex depends on. When that off-switch is impaired, inflammation doesn't fully resolve, which may help explain the sustained fatigue, brain fog, and autonomic symptoms of Long COVID.
Why would the neck affect the vagus nerve and inflammation?
The vagus nerve emerges from the brainstem and exits the skull right at the craniocervical junction — the region enclosed by the skull and the atlas and axis (C1 and C2). This is the most neurologically dense area of the spine. A misalignment here, often after whiplash or head trauma, can create mechanical irritation and altered input at exactly the level where the vagus emerges and the brainstem regulates autonomic function, potentially adding interference to an already-struggling system.
Is there research on the vagus nerve and Long COVID?
Yes. Reviews describe disruption of the vagal cholinergic anti-inflammatory pathway as a proposed mechanism in Long COVID, and vagus nerve stimulation is being studied as a treatment. Early trials of non-invasive vagal stimulation have reported improvements in cognition, mood, sleep, and fatigue. This research is still preliminary, but it establishes that supporting vagal function can improve Long COVID symptoms — which is the same brainstem-and-vagus target upper cervical care approaches mechanically.
What is heart rate variability, and why does it come up with Long COVID?
Heart rate variability (HRV) is a measure of the tiny beat-to-beat variations in your heart rate, and it reflects vagal (parasympathetic) tone. Low HRV indicates the body is stuck in sympathetic "fight or flight" dominance with a weak parasympathetic brake — a common finding in Long COVID that correlates with more inflammation, fatigue, and post-exertional malaise. It's essentially a readout of how well the nervous system's off-switch is working.
Should I still see my doctor if I pursue upper cervical care?
Absolutely. Long COVID requires medical evaluation and management, and upper cervical care is a complement to that, not a substitute. Seek prompt medical attention for chest pain, shortness of breath, fainting, significant heart-rate or blood-pressure changes, or new or rapidly worsening symptoms. Coordinating upper cervical care with your medical team is essential.
Long COVID and the upper cervical connection — Sarasota
If your Long COVID includes autonomic symptoms — fatigue, brain fog, racing heart, a body stuck in fight-or-flight — especially after any head or neck trauma, a focused upper cervical evaluation can help determine whether the mechanical environment of your brainstem and vagus nerve is worth addressing alongside your medical care.
Request a Consultation call 941 259-1891
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Long COVID (post-acute sequelae of SARS-CoV-2 infection) is a serious medical condition that must be evaluated and managed by qualified physicians. Upper cervical chiropractic does not treat SARS-CoV-2 infection, does not cure Long COVID, and is not a substitute for medical care; it focuses on mechanical and postural contributors at the craniocervical junction as a complement to appropriate medical management. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization or superiority is made or implied. Cone beam CT is used as a precision measurement and analysis tool, not as a diagnostic device for Long COVID. The mechanisms and research described — including the vagal cholinergic anti-inflammatory pathway and vagus nerve stimulation — are emerging, in many cases preliminary, and are presented for education rather than as proof of treatment outcomes. Individual results vary, and no specific outcome is guaranteed. Seek prompt medical attention for chest pain, shortness of breath, fainting, significant cardiovascular changes, or new or worsening neurological symptoms. Always consult your physician regarding diagnosis and management of Long COVID.



Leave a comment