

Why chronic ear fullness and pressure that does not resolve with standard treatment may have a structural cause at the top of the neck.
Obstructive eustachian tube dysfunction is the most common form of ETD and one of the most common reasons adults present to ENT clinics. The condition produces chronic ear fullness, muffled hearing, pressure that will not equalize, and the frustrating sense that something is just not right inside the ear. For some patients, the symptoms resolve with standard treatment — a course of nasal steroids, allergy management, or simply waiting out an upper respiratory infection. For others, the symptoms persist for months or years despite every medication and intervention available, and the conventional workup runs out of answers.
Schedule Your Appointment
Schedule appointmentFor these chronic non-responders, there is a structural factor that the standard workup does not routinely examine: the alignment of the craniocervical junction, where the skull meets the first two vertebrae of the neck. This article explains what obstructive ETD actually is, how the craniocervical junction connects to eustachian tube function, and when a structural evaluation deserves a place in the workup.
If chronic ear fullness has not responded to medical management, the structural angle may be the missing piece.
Call 941-259-1891 to schedule a free consultation.
What Obstructive Eustachian Tube Dysfunction Is
The eustachian tube is a small passageway, roughly an inch and a half long, that connects the middle ear to the back of the nasal cavity. Its job is to keep the air pressure inside the middle ear matched to the air pressure outside the head, to drain fluid that accumulates in the middle ear, and to limit the spread of secretions from the throat into the ear. The tube does this by briefly opening during swallowing, yawning, or chewing, then closing again to act as a one-way valve.
In obstructive ETD, the tube fails to open properly. The opening is incomplete, too brief, or does not occur at all when it should. The result is that pressure cannot equalize, fluid cannot drain, and the middle ear sits in a sustained state of negative pressure with mild fluid retention. The eardrum is pulled inward by the pressure difference, which restricts its movement and produces the muffled, dampened hearing patients describe. The fluid that accumulates contributes to the sensation of fullness.
Obstructive ETD is by far the most common subtype, accounting for the vast majority of chronic ETD cases. It is distinct from patulous ETD — where the tube stays open too much and patients hear their own voice echoing — and from baro-challenge-induced ETD, where the tube cannot keep up with rapid pressure changes during flying or diving.
How Obstructive ETD Feels
The symptom pattern is familiar to anyone who has had it.
A persistent sensation of ear fullness, plugging, or pressure that will not release. Muffled hearing, often in one ear more than the other, as if the volume on the world has been turned down. Audible popping, clicking, or crackling when swallowing, yawning, or moving the jaw. Difficulty equalizing pressure, with attempts to pinch the nose and blow either failing to clear the ear or clearing it for only seconds before the fullness returns. Mild tinnitus, often a low hum or rushing sound, frequently on the same side as the fullness. Symptoms that vary with head position, sometimes improving when lying down or leaning to one side. And sometimes, mild dizziness or imbalance — the middle and inner ear are mechanically connected, and chronic middle ear pressure can produce subtle vestibular effects.
Related article

Tinnitus Relief: Understanding the Upper Cervical Connection to Ear Ringing
Jan 26, 2026What separates the chronic obstructive ETD population from short-lived cases is duration. Symptoms that have persisted for three months or longer, that have not responded to medical treatment, and that interfere with daily life are the cases where a broader evaluation is warranted.
The Causes Standard Workups Focus On
The conventional medical workup for obstructive ETD focuses on identifiable causes of inflammation and mechanical obstruction.
Upper respiratory infections cause mucosal swelling that temporarily obstructs the tube. Most viral colds produce a few days of ETD. Allergies — particularly chronic environmental allergies — produce sustained mucosal inflammation that can compromise the tube opening over months and years. Chronic sinusitis maintains low-grade inflammation in the nasopharynx that affects the eustachian tube. Acid reflux can produce mucosal irritation in the back of the throat that propagates into the eustachian tube area. Anatomical issues — a deviated septum, enlarged adenoids in younger patients, nasal polyps — can mechanically interfere with the tube opening. And lifestyle factors like smoking impair ciliary function and mucosal health throughout the upper airway.
When one of these causes is identified and addressed, obstructive ETD often resolves. The chronic patient population — the one this article is written for — has already been through this workup. The allergies have been treated. The sinuses are clean. The septum has been examined. The symptoms continue anyway.
The Craniocervical Connection
The craniocervical junction is the region where the skull meets the first two vertebrae of the spine, the atlas (C1) and the axis (C2). Three bones — the occiput, the atlas, and the axis — sit in a precise relationship that supports the head, allows the head to rotate, and houses the corridor through which the spinal cord, brainstem, vertebral arteries, and major fluid pathways pass between the skull and the body.
When this region is misaligned — most often due to whiplash, head injury, sports trauma, falls, or even cumulative postural strain — the consequences extend beyond local neck symptoms. The craniocervical junction has specific anatomical and neurological connections to the structures that govern eustachian tube function. Three pathways are most relevant for obstructive ETD.
Pathway 1: Shared neurology with the trigeminal nerve
The eustachian tube does not open passively. It is actively opened by the contraction of a small muscle in the soft palate called the tensor veli palatini. This muscle is innervated by the mandibular division of the trigeminal nerve. The trigeminal nerve has direct interconnections with the upper cervical region through a brainstem area called the trigeminocervical complex — a zone where sensory fibers from the upper cervical nerves (C1, C2, and C3) and sensory fibers from the trigeminal nerve share neurons.
When the upper cervical region is misaligned, the irritation arising from C1, C2, or C3 can affect the function of trigeminal-mediated structures, including the tensor veli palatini. If the muscle does not fire correctly when it should, the eustachian tube does not open correctly. The result, sustained over months and years, is exactly the pattern obstructive ETD produces. This is the most direct anatomical pathway connecting craniocervical alignment to eustachian tube function.
Pathway 2: Autonomic regulation of the upper airway mucosa
The mucosal lining of the eustachian tube and middle ear is regulated by the autonomic nervous system, including parasympathetic fibers that emerge from the brainstem. The brainstem sits inside the corridor formed by the upper cervical vertebrae, and its mechanical environment can be influenced by craniocervical alignment. Chronic low-grade brainstem irritation, secondary to upper cervical misalignment, can disrupt autonomic regulation of the upper airway mucosa — contributing to baseline mucosal congestion, altered ciliary function, and impaired drainage.
This mechanism is less direct than the trigeminal pathway but explains why some patients with craniocervical structural problems have a generalized pattern of upper airway sensitivity — chronic congestion, recurrent sinus symptoms, and ETD all coexisting in a way that does not point to a single identifiable cause.
Related article
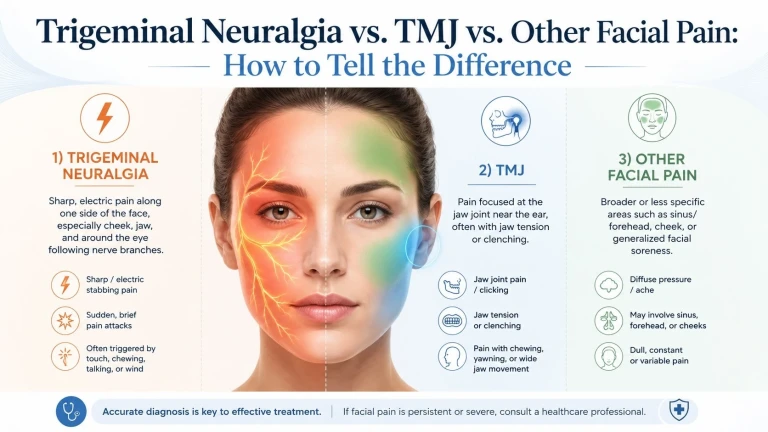
Trigeminal Neuralgia vs. TMJ vs. Other Facial Pain: How to Tell the Difference
Jul 08, 2026Pathway 3: Fascial and muscular tension propagation
The deep suboccipital muscles, the muscles of the upper neck, and the soft tissues supporting the pharynx and palate share fascial connections. Chronic asymmetric tension at the craniocervical junction can propagate through these connections into the upper pharyngeal region, affecting the soft tissues surrounding the eustachian tube opening. Patients with significant upper cervical dysfunction often have palpable asymmetry in the upper pharynx that mirrors the asymmetry in their neck.
The Choke Point Factor: Venous Drainage and Ear Pressure
Beyond the direct neural pathways, the craniocervical junction is the corridor through which the venous drainage of the head passes. Chiropractic neurologist Michael Flanagan, in his 2015 paper in Neurology Research International, described the craniocervical junction as a potential choke point for craniospinal hydrodynamics — a region where misalignment can compromise venous outflow from the skull (Flanagan, 2015).
For chronic obstructive ETD, this matters in a specific way. The venous drainage of the middle ear and surrounding structures is part of the broader cranial venous system. When craniocervical alignment compromises venous outflow, congestion in the upstream tissues — including the structures of the middle ear and the eustachian tube — can develop. Chronic venous congestion contributes to mucosal swelling, persistent fluid retention, and pressure dysregulation. This mechanism does not replace the direct neural pathways, but it adds another layer to why chronic ETD can persist in patients whose anatomy and inflammatory factors otherwise look normal.
If chronic ETD has persisted despite a clean ENT workup, a structural evaluation of the craniocervical junction may add the missing piece.
Call 941-259-1891 for a free consultation.
Who Is Most Likely to Have a Craniocervical Contribution
Not every patient with obstructive ETD has a craniocervical structural component. Some have clear inflammatory or anatomical causes that respond to standard treatment. The pattern that suggests a structural contribution worth investigating includes several recognizable features.
A history of neck trauma — whiplash from a car accident, sports concussion, falls, or other forceful events — even if the event occurred years or decades before the ear symptoms began. ETD that began after a specific identifiable injury, or that started gradually in the years following one. Symptoms that vary with head position, jaw position, or neck movement, suggesting a mechanical component. Associated symptoms that point to broader craniocervical involvement — chronic headache, dizziness, tinnitus, neck pain, jaw pain, brain fog. Persistent ETD despite a complete ENT workup that has not identified a clear cause or surgical target. Symptoms that recur after initial improvement from medical management. Asymmetric symptoms, with one ear consistently more affected than the other.
Patients who recognize several of these features in their own history are good candidates for an upper cervical evaluation. The structural angle may not apply to every chronic ETD case, but for the patients who fit this pattern, it deserves to be examined.
How Sarasota Upper Cervical Chiropractic Approaches This
Our practice focuses specifically on the precise structural relationship between the occiput, atlas, and axis. The approach combines precision imaging, objective testing, and specific low-force corrections delivered only when the measurements indicate a misalignment is present.
Three-dimensional CBCT imaging
Cone beam computed tomography is a low-dose three-dimensional imaging technology that produces a true 3D reconstruction of the upper cervical anatomy. Standard two-dimensional X-rays cannot reliably capture the geometric complexity of the craniocervical junction. CBCT can, and the measurements it provides are precise to within fractions of a degree. This is the imaging that allows us to identify whether a structural misalignment is present and, if so, exactly what its direction and magnitude are.
Leg length analysis and infrared thermography
Before any adjustment is delivered, two objective tests are performed at every visit. Leg length analysis measures functional asymmetry produced by upper cervical misalignment. Paraspinal infrared thermography measures asymmetric autonomic activity along the cervical spine. If both tests indicate the spine is in alignment, no adjustment is delivered. If they indicate a shift, a precise correction is delivered along the vector calculated from the CBCT.
Precision without manipulation
When a correction is indicated, it is specific to the upper cervical segment that has moved, delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The force is low. The motion is small. This precision-based approach is appropriate for patients with sensitized systems — including those with chronic ear symptoms whose autonomic regulation is already disrupted.
Related article
Post-Concussion Syndrome and the Upper Neck: The Missing Piece in Cases That Don't Recover
Jun 16, 2026Honest expectations
We will tell you honestly during your evaluation whether we believe upper cervical care is appropriate for your specific situation. If the structural exam, history, and imaging do not suggest a meaningful cervical contribution to your symptoms, we will say so. If they do suggest a contribution, we will explain what care would involve, what improvement typically looks like, and what we cannot promise. Symptomatic improvement in chronic ETD, when it occurs, is generally gradual rather than instantaneous, and outcomes vary by individual.
When to Schedule an Evaluation
An upper cervical evaluation is worth considering when several of the following are true alongside chronic obstructive ETD symptoms.
Your symptoms have persisted for three months or longer. Medical management — nasal steroids, antihistamines, decongestants, allergy treatment — has not produced lasting relief. Your ENT workup has not identified a clear surgical target, or you have been offered a procedure (tube placement, balloon dilation) and want to explore non-surgical options first. You have a history of whiplash, concussion, or other neck trauma in your past. You have associated symptoms — headache, dizziness, tinnitus, neck pain, jaw pain — that suggest broader craniocervical involvement. Your symptoms vary with head position or neck movement. The ear that is affected has been consistently one-sided in a pattern that matches a history of injury or asymmetric structural changes.
None of these alone is diagnostic. Several of them together suggest that the craniocervical junction deserves to be evaluated as part of your workup.
Schedule a free consultation to find out whether the craniocervical junction is part of your ETD picture. Call 941-259-1891.
Take the Next Step
Chronic obstructive ETD that has not responded to standard medical management deserves a thorough evaluation that includes the structural angle. For patients whose history and presentation suggest a craniocervical contribution, the assessment is non-invasive, informative, and often reveals what the conventional workup has not.
Sarasota Upper Cervical Chiropractic serves patients throughout the Sarasota and Bradenton areas. To schedule your free consultation, call 941-259-1891.
References
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Schilder, A. G. M., Bhutta, M. F., Butler, C. C., et al. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with chronic ear symptoms should pursue appropriate medical evaluation alongside any structural assessment. No claim is made or implied tha



Leave a comment