
Racing heart. Shaking. Lightheadedness. A wave of dread that feels like it comes out of nowhere. If you've experienced these and been told "it's just anxiety", but the explanation never quite fit, you're in one of the most common diagnostic mix-ups in medicine. POTS (postural orthostatic tachycardia syndrome) and anxiety can produce nearly identical sensations, yet they come from very different places. One is a malfunction of the autonomic nervous system. The other is rooted in psychological distress. Telling them apart matters enormously, because the right answer changes everything about what actually helps.
This article walks through how to distinguish POTS from anxiety, why the two are so often confused, how they can genuinely coexist, and, the thread that runs through the whole cluster — how the autonomic nervous system and the upper cervical spine sit at the center of the physical version of these symptoms. One boundary first: POTS and anxiety are both diagnosed and managed medically, and upper cervical chiropractic does not diagnose, treat, or cure either. What it focuses on is one possible contributor to autonomic balance, the mechanical environment of the brainstem at the top of the neck.
Schedule Your Appointment
Schedule appointmentWhy POTS and anxiety look so much alike
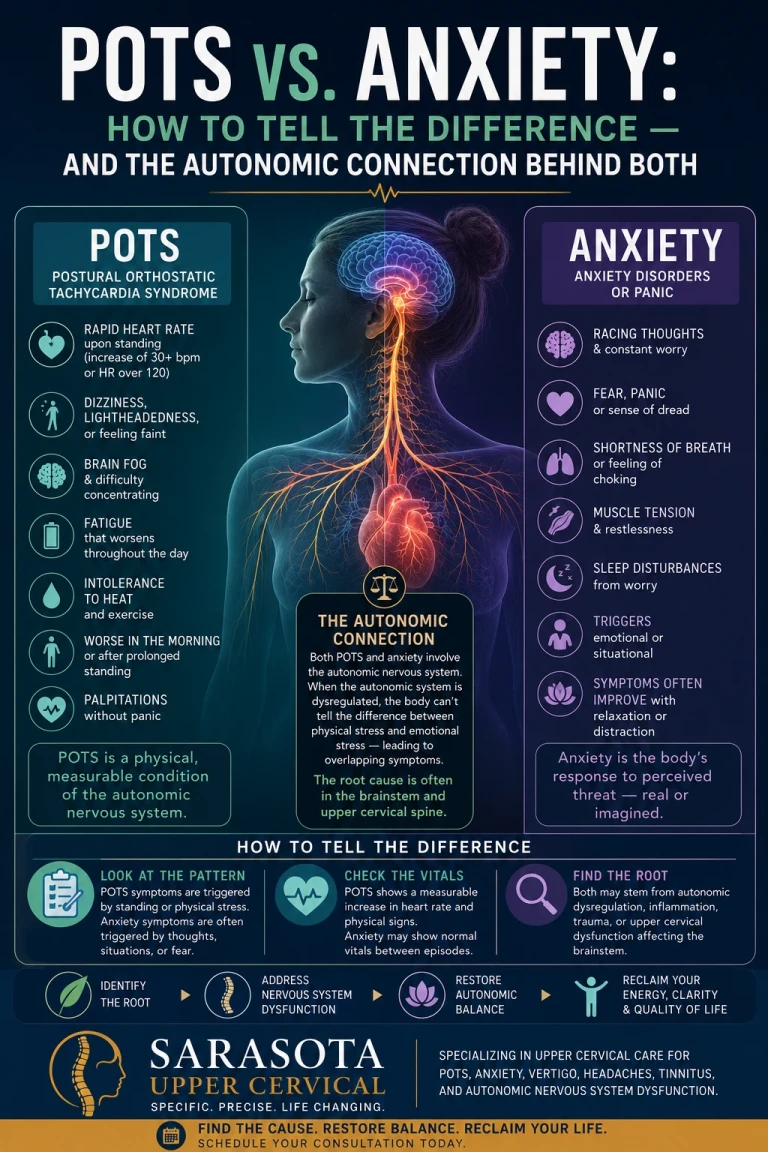
The overlap isn't a coincidence, it's physiology. Both conditions can activate the sympathetic "fight-or-flight" nervous system, which produces the same downstream effects regardless of what triggered it: a pounding or racing heart, sweating, trembling, shortness of breath, chest tightness, and that unmistakable sense of unease. When your heart is hammering, your body can't tell you whether the cause was a frightening thought or a drop in circulation on standing. The sensation is identical.
That's exactly why misdiagnosis is so common. As one clinical overview puts it, POTS and anxiety share similar symptoms like racing heart and sweating, but the underlying causes and key differentiators are very different. The tragedy is that many POTS patients spend years being told their very physical symptoms are "all in their head" before receiving a correct diagnosis, a detour that delays real help and adds a layer of being disbelieved on top of being ill.
An important, stigma-correcting fact: Research shows POTS patients do not have a higher prevalence of anxiety disorders than the general population. The anxiety-like symptoms of POTS are physiological events produced by a dysregulated autonomic nervous system, not evidence of an anxiety disorder. If you've been made to feel your illness is imagined, the science does not support that.
The single clearest difference: does gravity trigger it?
If you remember one thing, remember this: POTS is position-dependent; anxiety is not.
POTS symptoms are triggered by being upright and relieved by lying down. The hallmark is a measurable, objective sign, a heart rate increase of 30 or more beats per minute upon standing, which improves when lying down, a positional pattern that doesn't occur with anxiety. Anxiety symptoms, by contrast, can strike in any position and are typically tied to stressful thoughts, situations, or triggers, not to gravity. If your heart reliably races when you stand up from bed or rise after sitting a while, and settles when you lie back down, that positional signature points toward POTS rather than a primary anxiety disorder.
Related article
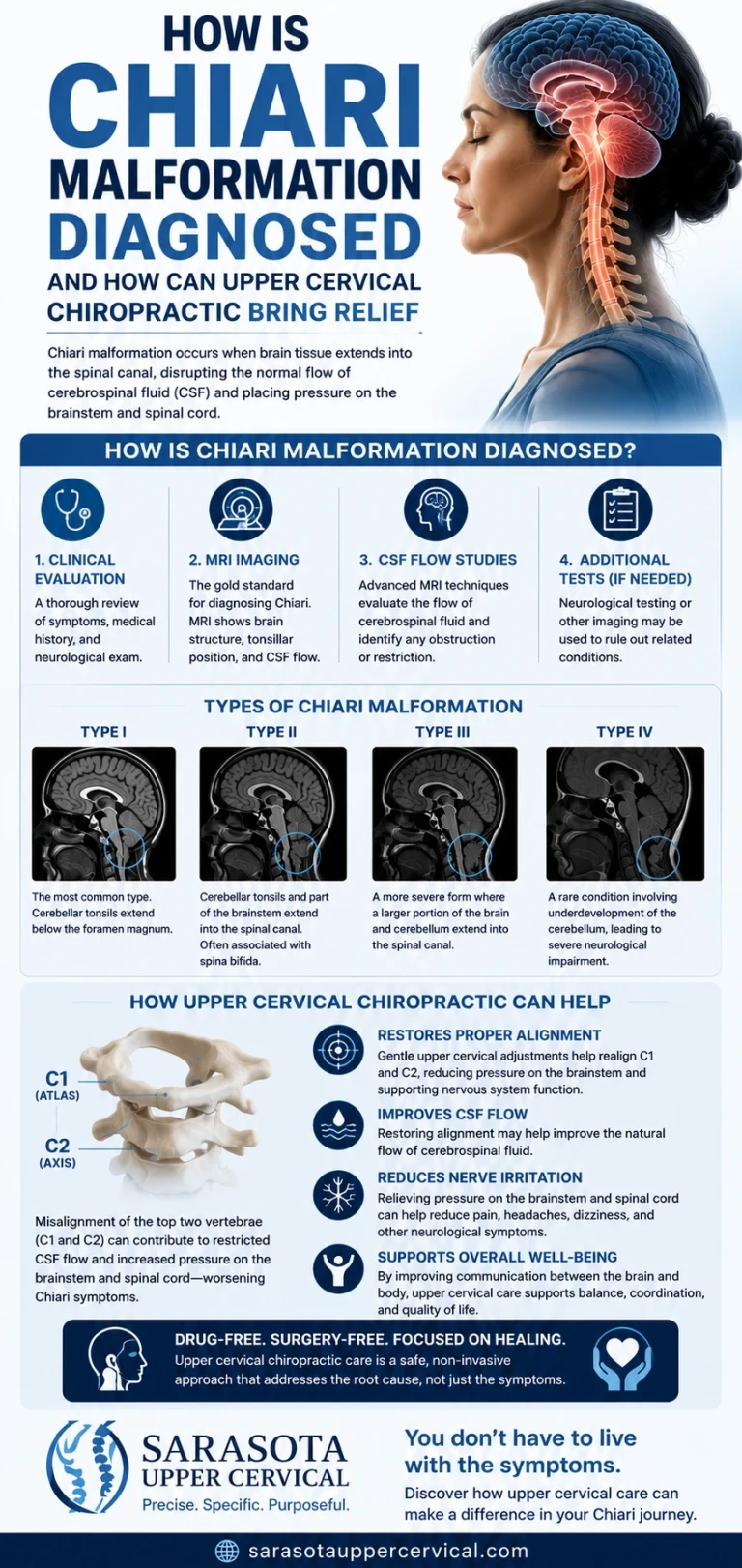
How is chiari malformation diagnosed and how can upper cervical chiropractic bring relief
Jul 12, 2026How to tell them apart
The practical takeaway: a simple, objective test settles much of it. A tilt table test is the gold standard, but an in-office active stand test, lie down, then stand while heart rate and blood pressure are measured, can reveal the positional heart-rate rise that anxiety doesn't produce. If you suspect POTS, this is the conversation to have with your physician.
They can also genuinely coexist — and that matters
Here's the honest nuance that a lot of "POTS vs. anxiety" content gets wrong by making it purely either/or: the two can occur together, and that's common. Some people have POTS. Some have anxiety. Some have both. Importantly, living with an unpredictable, frightening physical condition like POTS can produce a secondary, understandable anxiety — as one review notes, it's common for people with POTS to experience increased anxiety as a result of the distressing nature of their physical symptoms and the impact on daily life. That anxiety is real and deserves care, it just isn't the root cause of the racing heart on standing.
So the goal isn't to prove your symptoms are "really POTS and not anxiety," or to dismiss an anxiety diagnosis. It's to get an accurate, complete picture, because the two are managed differently and getting it wrong has consequences.
The autonomic nervous system: the common ground beneath both
To understand where the upper neck fits, it helps to see what POTS and the physical side of anxiety actually share: both are states of autonomic imbalance, specifically a tilt toward sympathetic ("fight-or-flight") dominance over the parasympathetic ("rest-and-digest") brake.
That balance is governed in the brainstem. The master regulator of sympathetic outflow is a region called the rostral ventrolateral medulla (RVLM), the "pressor area" of the medulla, responsible for basal and reflex control of sympathetic activity, and central to the baroreflex that adjusts heart rate and blood pressure when you change position. Right beside it sit the sensory and parasympathetic nuclei, the nucleus tractus solitarius and the dorsal motor nucleus of the vagus, that run the vagal brake. This tight cluster of brainstem nuclei is the physical hardware of autonomic balance, and a recent mechanistic review confirms these structures, the nucleus tractus solitarius, dorsal motor nucleus of the vagus, and rostral ventrolateral medulla, reside within the medulla and are where orthostatic-intolerance and POTS-like phenotypes can arise from craniocervical-junction disorders.
And that hardware lives inside the craniocervical junction, the space enclosed by the base of the skull and the top two vertebrae of the neck, the atlas (C1) and axis (C2). The autonomic control room sits at the very top of your neck.
Related article
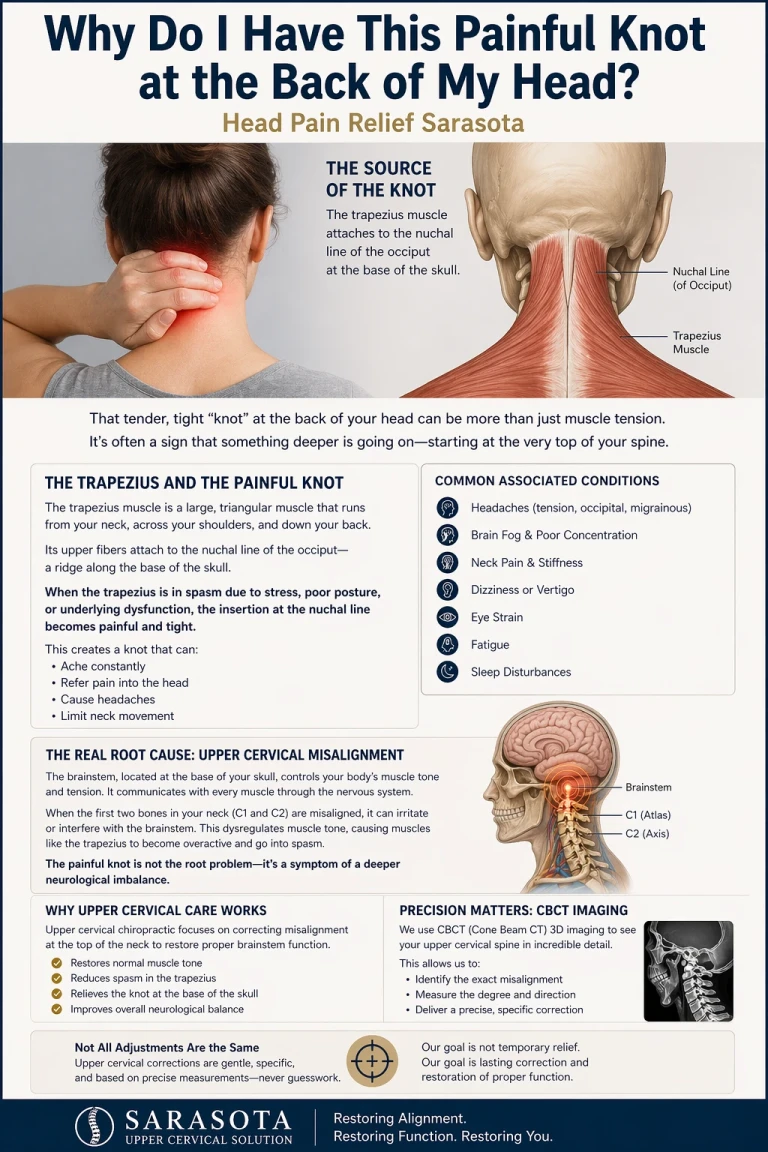
Why do I have this painful knot at the back of my head | Head Pain relief sarasota
Apr 23, 2026The upper cervical connection: how the atlas influences autonomic balance
This is where the upper cervical spine enters, and it's specific neuroanatomy, not a vague claim. The upper neck is the most proprioceptively dense region of the body, and its position sensors don't only feed posture and balance; they feed the autonomic system. Research tracing upper cervical sensory nerves found that stimulating the second cervical nerve altered central respiratory drive and increased perfusion pressure, and revealed a response in sympathetic nerve activity, with the responsible fibers identified as proprioceptive. There is a documented network of neurophysiological connections between the cervical spine mechanoreceptors and the sympathetic nervous system.
When the atlas is misaligned and the upper cervical joints lose normal motion, often after whiplash, concussion, or head/neck trauma, that proprioceptive signal becomes distorted. In chronic cervical dysfunction, the cervical afferents transmit impaired proprioceptive signals, with these patients often having a history of neck pain, whiplash, or concussion. The proposed consequence is that distorted upper cervical input, plus mechanical irritation of the brainstem environment at the craniocervical junction, may nudge an already-dysregulated autonomic system further toward sympathetic dominance — the same overdrive state that produces both POTS symptoms and the physical sensations mistaken for anxiety.
The thermostat analogy: Picture the brainstem as the thermostat regulating your autonomic "temperature," with the upper cervical proprioceptors as part of the sensor feeding it. When the atlas is misaligned, it's like draping a towel over that sensor, the thermostat starts getting faulty readings and can crank the sympathetic "heat" when it shouldn't. The control center is intact; the input and output are distorted.
Where upper cervical care fits — honestly
What upper cervical care focuses on is autonomic balance, restoring normal alignment and proprioceptive input at the craniocervical junction, so the brainstem receives an accurate position signal and one source of mechanical interference is removed from the system that sets sympathetic and parasympathetic tone. The rationale is that the upper cervical spine surrounds and protects the brainstem, and when the atlas or axis becomes even slightly misaligned it can alter the environment around the brainstem, with care focused on improving the body's ability to self-regulate.
There's supportive direction from the research, too: a randomized controlled trial found that cervical lordosis rehabilitation produced measurable changes in autonomic nervous function and cervical sensorimotor control. This work is still emerging and doesn't prove a cure, but it points at the same target the upper cervical approach aims to support. For someone with genuine POTS, especially with a history of head or neck trauma, evaluating the upper cervical spine is a reasonable, low-risk avenue to pursue alongside medical care, not instead of it.
Why CBCT imaging matters here
Because any upper cervical correction is precise, the analysis must be precise. We use cone beam computed tomography (CBCT) as a precision measurement tool to see the true three-dimensional position of the atlas and axis, so an assessment is tailored to the individual's anatomy rather than estimated. (CBCT is a measurement and analysis tool; it is not a diagnostic test for POTS or anxiety, which are diagnosed clinically.)
What to do if you think you've been misdiagnosed
If your "anxiety" reliably tracks with standing and eases when you lie down, it's worth a specific conversation with your physician about POTS and asking about an active stand test or tilt table test. Advocate for objective measurement — the positional heart-rate rise is something a test can capture. And remember it's not either/or: you can pursue an accurate POTS evaluation while also caring for any real anxiety. The goal is the complete, correct picture, so your treatment actually matches what's happening in your body.
Related article
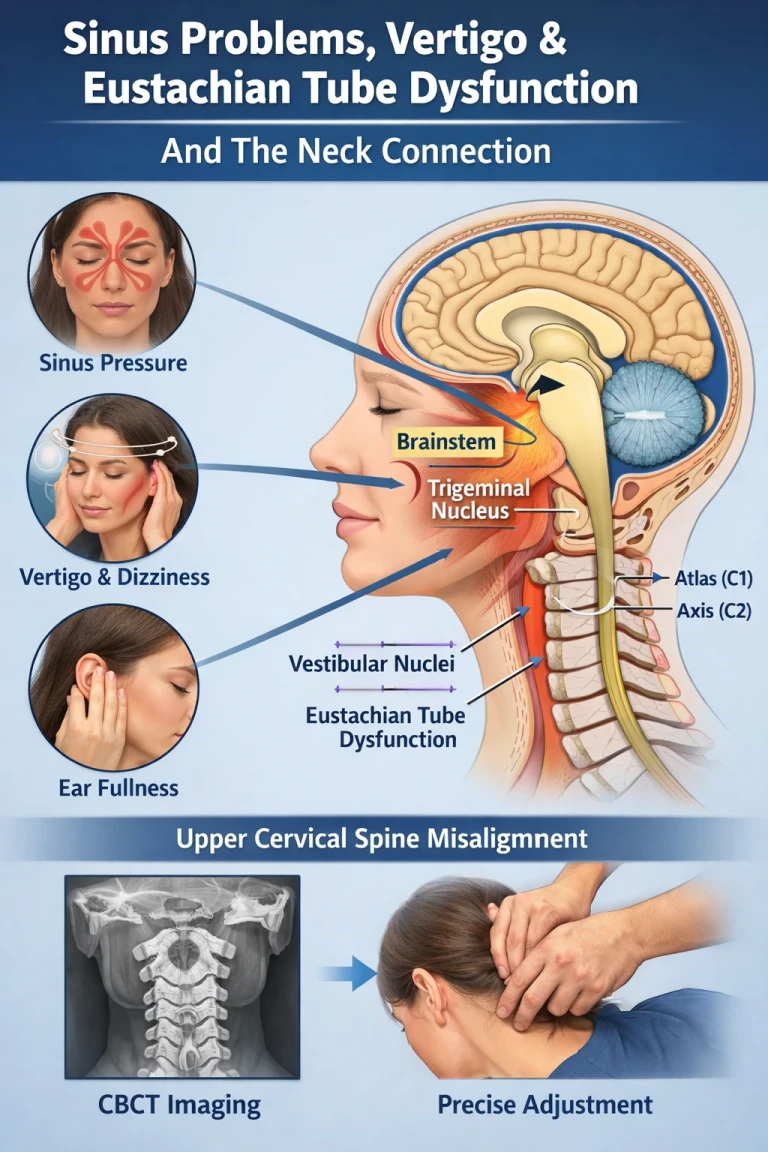
Sinus Problems, Eustachian Tube Dysfunction, Vertigo, and the Neck Connection
Apr 18, 2026Questions and Answers
How can I tell if it's POTS or anxiety?
The clearest difference is position. POTS symptoms are triggered by standing and improve when you lie down, and they come with a measurable heart-rate rise of 30 or more beats per minute on standing. Anxiety symptoms can occur in any position and are typically tied to stressful thoughts rather than gravity. If your racing heart reliably appears when you stand and settles when you lie down, that positional pattern points toward POTS — and an in-office standing test or tilt table test can confirm it.
Is POTS just anxiety?
No. POTS is a malfunction of the autonomic nervous system that produces physical symptoms which happen to resemble anxiety. Research shows POTS patients do not have higher rates of anxiety disorders than the general population, and the symptoms are physiological events driven by autonomic dysregulation, not psychological distress. Being told it's "all in your head" is not supported by the science.
Can I have both POTS and anxiety?
Yes, and it's common. Some people have POTS, some have anxiety, and some have both. Living with an unpredictable, frightening physical condition like POTS can also produce a secondary, understandable anxiety. Both deserve care. The goal isn't to prove your anxiety is "really POTS" — it's to get an accurate, complete diagnosis so each is treated appropriately.
Why does getting the right diagnosis matter so much?
Because the treatments differ and one can worsen the other. SSRIs and SNRIs often help anxiety, but in POTS, SNRIs can increase sympathetic drive and worsen symptoms, and SSRIs show minimal benefit. Being treated for anxiety when you actually have POTS can mean a medication that raises the very sympathetic activity driving your symptoms. Effective POTS care targets the autonomic dysfunction directly, under medical supervision.
What does the neck have to do with POTS or anxiety-like symptoms?
Both POTS and the physical side of anxiety involve autonomic imbalance toward sympathetic overdrive, and that balance is regulated in the brainstem, which sits inside the craniocervical junction at the top of the neck. The upper neck's dense position sensors feed into the brainstem and can influence sympathetic output. When the atlas is misaligned, that input can become distorted, potentially nudging an already-dysregulated system further toward overdrive. Upper cervical care focuses on that mechanical contributor, alongside medical care.
Can upper cervical chiropractic cure my POTS or anxiety?
No. Upper cervical care does not diagnose, treat, or cure POTS or anxiety, both of which require medical and, where relevant, mental-health care. It focuses on autonomic balance by restoring normal alignment and proprioceptive input at the craniocervical junction, to remove one possible source of mechanical interference. It's a complement to medical care, especially for those with a history of head or neck trauma, not a replacement or a cure.
POTS, anxiety, and the upper cervical connection — Sarasota
If your "anxiety" tracks with standing and eases when you lie down — especially after a head or neck injury — a focused upper cervical evaluation can help determine whether the mechanical environment of your brainstem is worth addressing alongside your medical care.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. POTS and anxiety are distinct conditions that must be diagnosed and managed by qualified medical and, where appropriate, mental-health professionals; they can also coexist. Upper cervical chiropractic does not diagnose, treat, or cure POTS or anxiety and is not a substitute for medical or mental-health care; it focuses on mechanical and proprioceptive contributors at the craniocervical junction that may influence autonomic balance, as a complement to appropriate care. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization or superiority is made or implied. Cone beam CT is used as a precision measurement and analysis tool, not as a diagnostic device. Medication information is described in general terms from published research and is not individual medical advice; never start, stop, or change any medication except under the direction of your physician. The mechanisms and research described are emerging and presented for education; individual results vary, and no specific outcome is guaranteed. Seek prompt medical attention for chest pain, fainting, severe or irregular heart rate, or new or worsening symptoms, and seek immediate help for any mental-health crisis. Always consult qualified healthcare providers regarding diagnosis and treatment.



Leave a comment