

Understanding the Brainstem, Upper Cervical Spine, and Precision Correction
Atypical trigeminal neuralgia (ATN), often called Type 2 trigeminal neuralgia, is one of the most frustrating and misunderstood chronic pain conditions affecting the face. Patients frequently describe a constant, burning, aching, or pressure-like pain that can feel relentless and life-altering. Unlike classic trigeminal neuralgia, this condition often doesn’t follow a predictable pattern, making both diagnosis and treatment more complex.
Schedule Your Appointment
Schedule appointmentIn this article, we’ll break down the difference between typical and atypical trigeminal neuralgia, explore the neurology of the brainstem and trigeminal system, and explain how upper cervical spine misalignment may play a role—along with how precise upper cervical correction in Sarasota may help restore function and provide relief.
What Is Atypical Trigeminal Neuralgia?
Trigeminal neuralgia is a disorder of the fifth cranial nerve—the trigeminal nerve—which is responsible for sensation in the face. When this nerve becomes irritated or damaged, it can produce severe facial pain.
Typical vs. Atypical Trigeminal Neuralgia
Understanding the difference between these two forms is critical:
Typical Trigeminal Neuralgia (TN1)
Sudden, intense, electric shock-like pain
Episodes last seconds to minutes
Triggered by light touch (talking, brushing teeth, wind)
Pain comes in bursts with pain-free intervals
Atypical Trigeminal Neuralgia (TN2)
Constant, dull, burning, or aching pain
Less sharp but more persistent
May include occasional sharp flares
Often lacks clear triggers and is harder to diagnose
Many patients actually experience a combination of both types, which can further complicate treatment.
Why Atypical Trigeminal Neuralgia Is So Challenging
Atypical trigeminal neuralgia is often misdiagnosed as:
TMJ dysfunction
Dental pain
Sinus issues
Migraines
Because the pain is constant rather than episodic, it doesn’t always fit the “classic” trigeminal neuralgia pattern. Additionally, imaging like MRI may not always reveal a clear cause, even though underlying nerve irritation exists.
This is why many patients go years without real answers.
The Brainstem Connection: Where the Problem Begins
To truly understand trigeminal neuralgia—especially atypical—you must understand the brainstem.
Related article

Facet syndrome and posture | Facet syndrome treatment and relief Sarasota
Jun 24, 2026The trigeminal nerve originates in the brainstem, specifically in an area called the trigeminal nucleus complex. This nucleus is not just a small point—it actually extends downward into the upper cervical spinal cord, reaching approximately the level of C2–C3 (this is often referred to as the trigeminocervical complex).
This is a critical concept.
Why This Matters:
The trigeminal system and upper cervical spine are neurologically connected
Sensory input from the face and upper neck converges in the same region
Dysfunction in the upper neck can influence trigeminal nerve processing
This neurological overlap explains why patients with:
Neck injuries
Whiplash
Postural distortions
Upper cervical misalignment can develop facial pain syndromes, including trigeminal neuralgia.
How Upper Cervical Misalignment May Affect the Trigeminal System
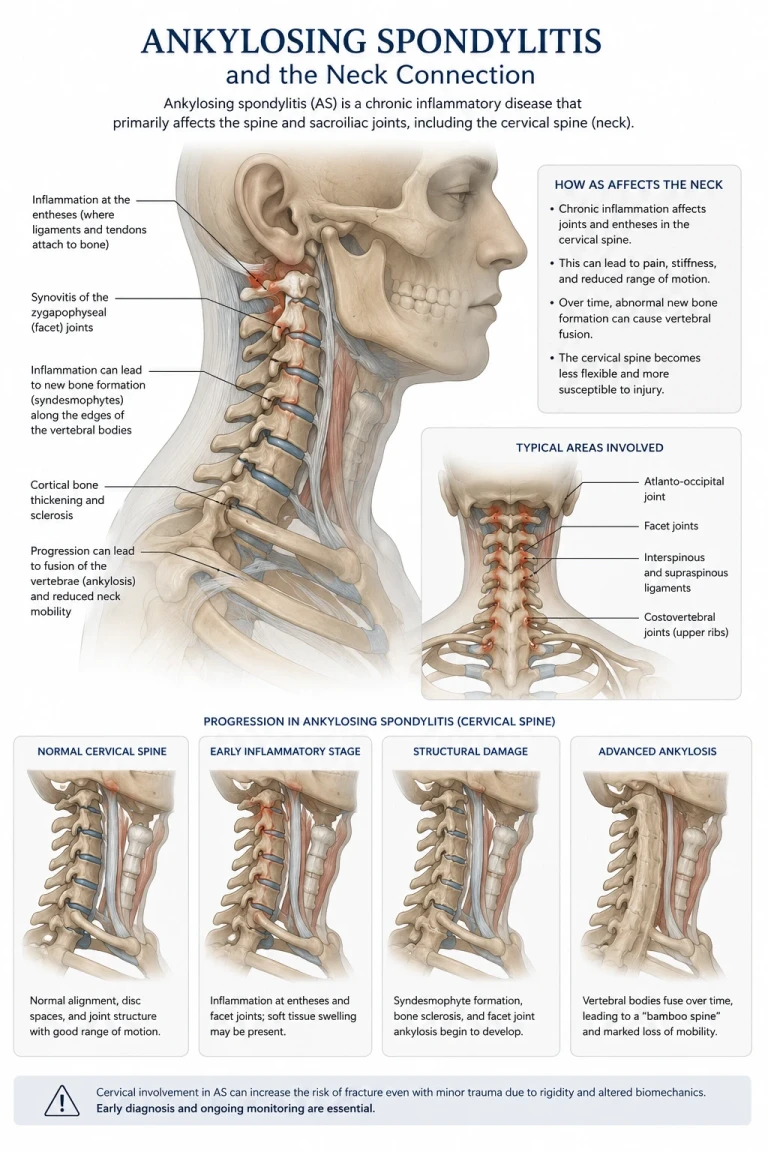
The atlas (C1) and axis (C2) vertebrae sit directly beneath the skull and surround the brainstem. This area is one of the most neurologically dense regions in the body.
When these vertebrae become misaligned, several things can occur:
1. Mechanical Stress on the Brainstem
Even slight misalignments can alter the position and tension of surrounding tissues, potentially affecting brainstem function.
2. Abnormal Sensory Input (Dysafferentation)
The upper cervical joints are rich in mechanoreceptors. When misaligned:
They send abnormal signals to the brainstem
This disrupts normal sensory processing
The trigeminal nucleus may become hypersensitive
3. Altered Muscle Tone & Nerve Irritation
Changes in muscle tone around the skull base can:
Increase tension on cranial nerves
Affect blood flow and neural signaling
Contribute to chronic pain patterns
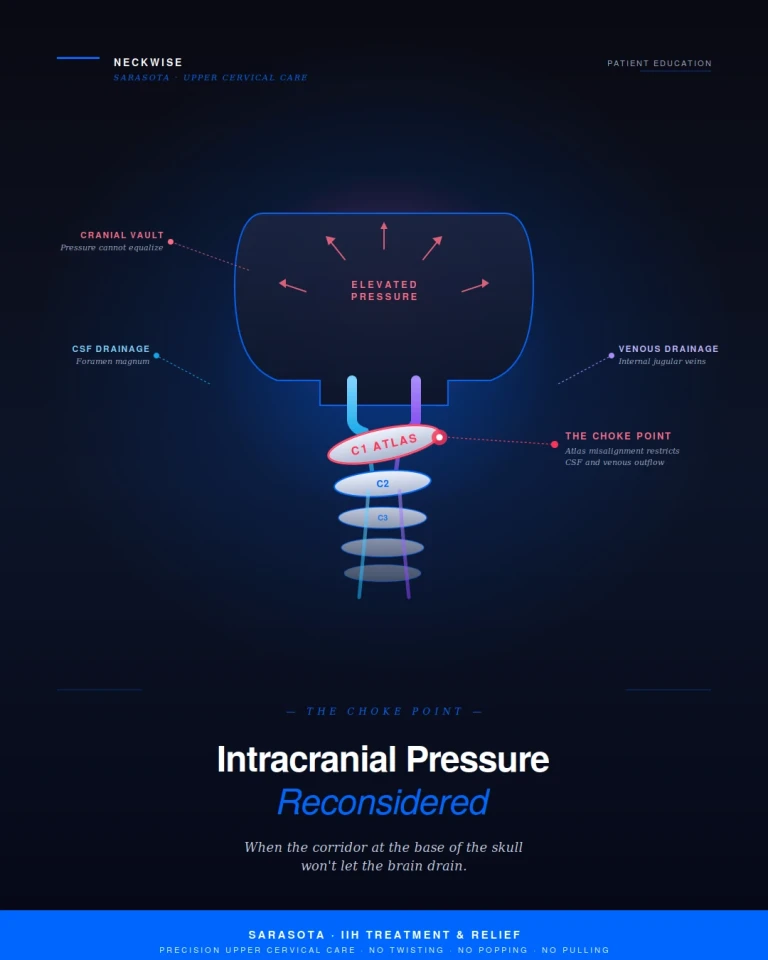
4. Vascular and CSF Dynamics
The brainstem is also responsible for regulating:
Blood flow
Cerebrospinal fluid (CSF) movement
Trigeminal neuralgia is often associated with vascular compression near the brainstem , and any disruption in this region may contribute to nerve irritation.
The Missing Link: The Trigeminocervical Complex
One of the most important but overlooked concepts is the trigeminocervical complex.
This is where:
Trigeminal nerve fibers (face)
Upper cervical nerve fibers (neck)
…merge and communicate.
This means:
A problem in the neck can be perceived as pain in the face
A trigeminal condition may actually have cervical involvement
This is why many atypical trigeminal neuralgia patients also report:
Neck stiffness
Headaches
Occipital pain
Worsening symptoms with head movement
Conventional Treatment Options
Medical treatment for trigeminal neuralgia typically includes:
Medications
Carbamazepine (first-line treatment)
Anticonvulsants
Antidepressants (for atypical cases)
Procedures
Microvascular decompression
Radiofrequency ablation
Gamma Knife radiosurgery
While these can help, they often:
Address symptoms rather than root cause
Have side effects
May not fully resolve atypical cases
Upper Cervical Chiropractic: A Different Approach
Upper cervical chiropractic focuses on correcting structural misalignments at the top of the spine—specifically C1 and C2.
Why This Approach Makes Sense for ATN
If the trigeminal system and upper cervical spine are neurologically linked, then restoring proper alignment may:
Normalize input to the brainstem
Reduce trigeminal nerve hypersensitivity
Improve overall neurological function
Decrease chronic pain signaling
The Role of 3D Imaging (CBCT)
One of the biggest advancements in upper cervical care is the use of Cone Beam CT (CBCT) imaging.
Why 3D Imaging Matters
Every person’s misalignment is unique.
CBCT allows doctors to:
Visualize the exact orientation of C1 and C2
Measure misalignment in three dimensions
Identify asymmetries and rotations
Create a precise, customized correction
This is not guesswork.
Precision Upper Cervical Correction
Unlike traditional chiropractic adjustments, upper cervical corrections are:
Extremely specific
Based on imaging
Gentle (no twisting, cracking, or popping)
Designed to restore alignment—not force movement
The goal is simple:
👉 Correct the misalignment
👉 Allow the body and nervous system to normalize
When the brainstem is no longer under abnormal stress and sensory input becomes balanced, many patients experience:
Reduced facial pain
Fewer flare-ups
Improved nervous system regulation
Why This Matters for Sarasota Patients
In Sarasota, many patients suffering from atypical trigeminal neuralgia have:
Tried medications without lasting relief
Seen dentists, neurologists, and specialists
Been told “everything looks normal”
But when you understand the relationship between:
The brainstem
The trigeminal nerve
The upper cervical spine
…it opens a completely new pathway for evaluation and care.
Final Thoughts: A New Perspective on Facial Pain
Atypical trigeminal neuralgia is not just a nerve problem—it’s often a brainstem processing issue.
And the brainstem sits directly adjacent to the upper cervical spine.
That connection cannot be ignored.
While not every case of trigeminal neuralgia is caused by upper cervical misalignment, many patients—especially those with chronic, atypical, or treatment-resistant symptoms—may have an underlying cervical component that has never been addressed.
If You’re Struggling with Atypical Trigeminal Neuralgia
Ask yourself:
Did your symptoms begin after a neck injury or trauma?
Do you also have neck stiffness or headaches?
Have traditional treatments failed to give lasting relief?
If so, it may be time to look at the upper cervical spine.
Because sometimes, the source of facial pain isn’t just in the face…
…it’s in the alignment of the neck and the function of the brainstem.



Leave a comment