
"Why mechanical irritation of the vestibular system is often misdiagnosed as a viral inflammation — and how precision upper cervical care offers a path forward"
Vestibular neuritis is one of the most common causes of acute, severe vertigo. Patients describe sudden, intense spinning that comes on without warning, often lasting days, sometimes accompanied by nausea, vomiting, imbalance, and a profound inability to function. The textbook explanation is straightforward: a viral inflammation of the vestibular nerve, the nerve that carries balance information from the inner ear to the brainstem. Patients are typically told to wait it out, take meclizine for symptom control, and trust that the inflammation will resolve on its own.
Schedule Your Appointment
Schedule appointmentFor some patients, that recovery happens. For many others, it does not. The acute spinning may settle, but lingering dizziness, brain fog, head pressure, motion sensitivity, and chronic imbalance persist for months or years. These patients cycle through ENTs, neurologists, and vestibular therapists searching for an answer that the standard workup never quite provides.
At Sarasota upper cervical, we focus on a part of the picture that is consistently overlooked. The vestibular system does not exist in isolation — it is mechanically and neurologically connected to the upper cervical spine. When the atlas and axis are misaligned, the vestibular system can be irritated in ways that mimic, complicate, or directly cause what looks like vestibular neuritis. The clinical presentation can be nearly identical, which is part of what makes this condition so difficult to diagnose accurately.
What Vestibular Neuritis Actually Is
The vestibular nerve, technically the vestibular branch of the eighth cranial nerve, carries signals from the semicircular canals and otolith organs of the inner ear to the vestibular nuclei in the brainstem. These signals tell the brain where the head is in space, how it is moving, and how to coordinate balance, eye movements, and posture in real time.
When this nerve becomes inflamed or irritated, the brain receives garbled input. The brainstem interprets the corrupted signal as motion that is not actually occurring, producing the hallmark symptom of severe rotational vertigo. The traditional diagnosis is made clinically — based on the pattern of symptoms, an examination of eye movements, and the absence of hearing loss (which would suggest labyrinthitis instead). Imaging is usually normal.
The conventional explanation is viral. The theory holds that a reactivation of a herpes-family virus inflames the vestibular nerve, and once the inflammation resolves, the nerve recovers. This is a reasonable hypothesis for many cases. The problem is that the diagnosis is rarely confirmed with any objective test. There is no virus identified. There is no scan that shows inflammation. The diagnosis is based on what the symptoms look like — and what the symptoms look like overlaps significantly with mechanical irritation of the vestibular system from the upper cervical spine.
The Vestibular Centers and the Upper Cervical Spine
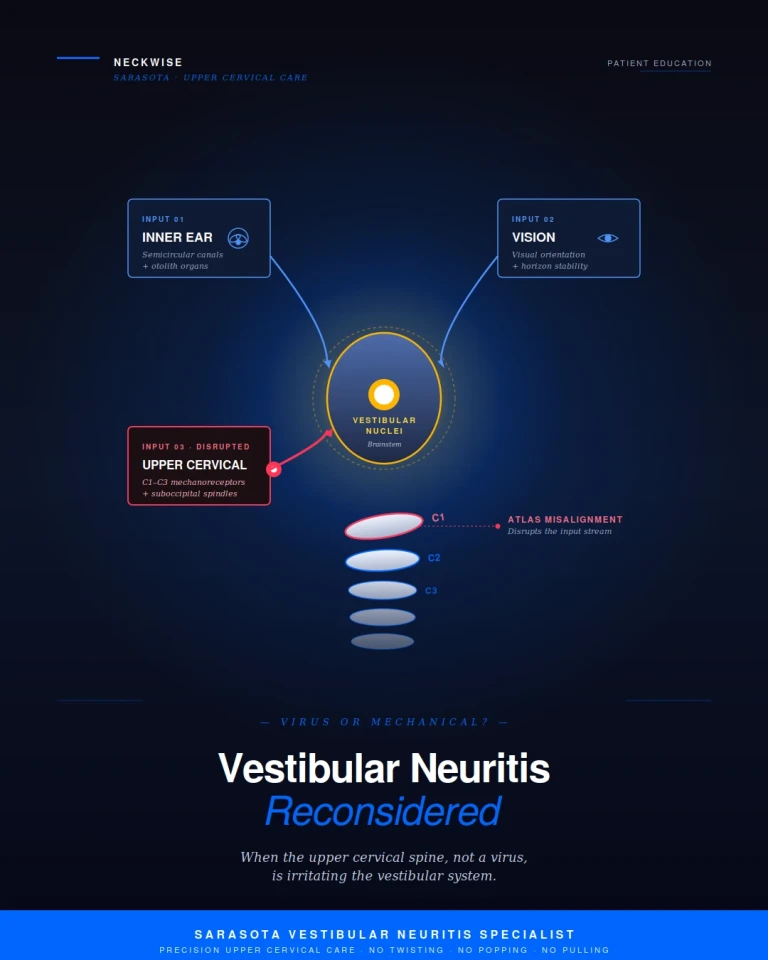
The vestibular nuclei sit in the brainstem at the level of the pontomedullary junction — the precise area that lives directly inside the upper cervical corridor. They are not isolated processing centers. They receive convergent input from three major sources: the inner ear, the visual system, and the proprioceptive system of the upper neck. The brain integrates all three streams to produce a stable sense of where the body is in space.
The upper cervical spine, particularly the C1, C2, and C3 region, contains an exceptionally dense supply of mechanoreceptors and proprioceptors. The deep suboccipital muscles alone contain some of the highest concentrations of muscle spindles found anywhere in the human body. Every joint capsule, ligament, and small muscle in this region is constantly streaming positional data into the brainstem, and that data flows directly into the vestibular nuclei. The neck does not just support the head — it tells the brainstem where the head is.
This convergence has been documented repeatedly in the neuroscience literature, and it has practical clinical consequences. When upper cervical input is normal, the vestibular system has a clean reference signal. When upper cervical input is abnormal — because of a misalignment, sustained muscle contraction, or joint dysfunction — the vestibular nuclei receive conflicting information. The brain attempts to reconcile the mismatch, and the result can be vertigo, dizziness, motion sensitivity, and imbalance that look indistinguishable from a viral inflammation of the vestibular nerve.

The Diagnostic Problem: Virus or Mechanical Irritation?
This is where the conventional model runs into trouble. A patient presents with sudden, severe vertigo. The exam is consistent with a peripheral vestibular issue. Imaging is unremarkable. The clinician makes a diagnosis of vestibular neuritis based on pattern recognition and tells the patient it is viral. But the truth is that the underlying cause cannot be confirmed by any test that is routinely ordered. The diagnosis is, in many cases, a label applied to a presentation rather than an identification of the actual mechanism.
Consider the overlap. Both viral inflammation and upper cervical mechanical irritation can produce sudden onset vertigo, both can produce nausea and imbalance, both can affect a patient who recently had a cold or stressful event, and both can leave behind lingering dizziness, brain fog, and motion sensitivity. The acute presentation is often clinically identical.
There are, however, clues that point toward a mechanical contribution. Patients with mechanically driven vestibular symptoms often have a history of head or neck trauma — sometimes recent, often years or decades old. They frequently report neck stiffness or tension that worsens during episodes. They may notice that certain head positions, sleeping postures, or sustained sitting trigger or worsen symptoms. They sometimes describe their dizziness as feeling "connected" to their neck in a way that pure viral neuritis would not. And critically, they often fail to recover on the timeline a viral inflammation would predict — because the irritation never resolves on its own when the underlying mechanical cause is still present.
This does not mean that vestibular neuritis is never viral. It means that when the diagnosis has been made, recovery has stalled, or symptoms recur, the mechanical contribution from the upper cervical spine deserves a serious look. The two can also coexist: a viral event that initially inflamed the nerve can leave behind a sensitized vestibular system that is then perpetuated by underlying upper cervical dysfunction.
Common Associated Symptoms
Patients who present to Neckwise with what has been diagnosed as vestibular neuritis or post-neuritis vestibular dysfunction commonly report a constellation of symptoms beyond the primary vertigo. These often include:
• Persistent dizziness or unsteadiness, particularly in busy visual environments such as grocery stores
• Brain fog, difficulty concentrating, and a sense of being mentally slow
• Motion sensitivity in cars, on escalators, or while watching screens
• Head pressure or fullness, often described as a heavy or foggy feeling
Related article
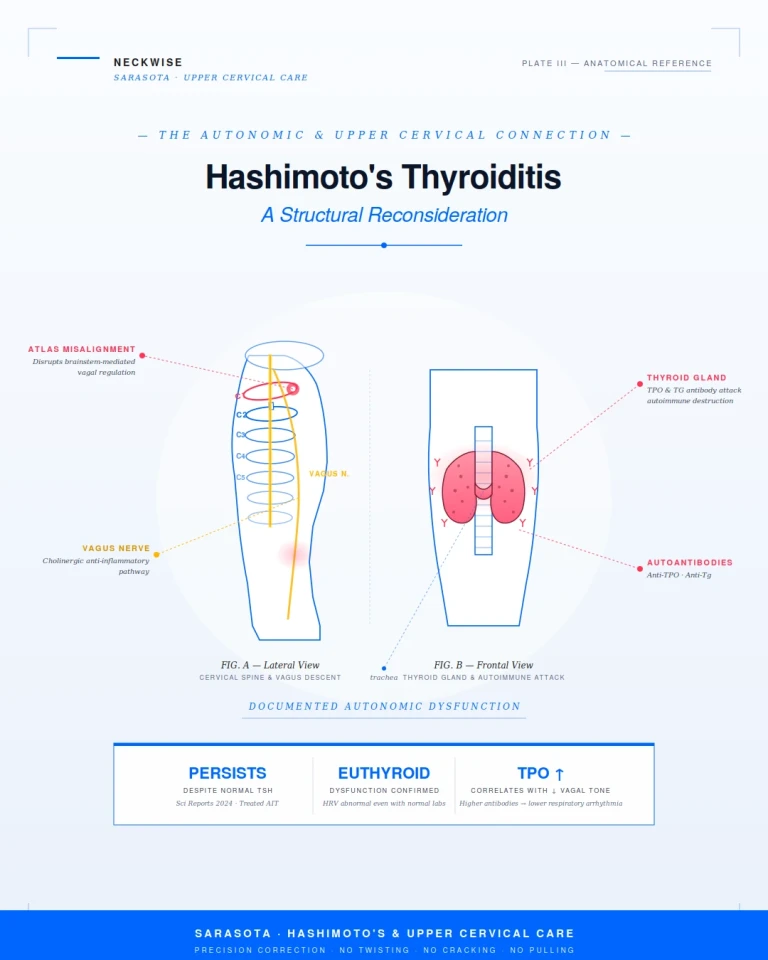
Hashimoto's Thyroiditis Treatment Support in Sarasota | The Autonomic and Upper Cervical Connection
May 14, 2026• Tinnitus or ear fullness without measurable hearing loss
• Neck pain, stiffness, or tension at the base of the skull
• Headaches or migraines that began or worsened around the same time as the vertigo
• Nausea triggered by head movement, even months after the acute episode
• Anxiety or a fear of leaving the house, often secondary to unpredictable symptoms
• Disrupted sleep, fatigue, and a general sense that the nervous system is on edge
This pattern — vertigo plus neck symptoms plus autonomic and cognitive symptoms — is a strong clinical signal that the upper cervical spine is contributing. A purely viral process would not typically produce this full picture, and especially not its persistence.
How Neckwise Evaluates Vestibular Cases
The evaluation at Neckwise is built around a simple question: is the upper cervical spine measurably contributing to this patient's vestibular symptoms? The process is structured to answer that objectively rather than by intuition or feel.
It begins with a comprehensive consultation and history. We listen for the timeline of the vertigo, prior treatments, prior trauma, and the full pattern of associated symptoms. From there, we use objective testing to determine whether the nervous system is showing measurable signs of upper cervical involvement. A leg balance test reveals neurological compensation patterns produced by the body trying to balance over an off-axis foundation, and infrared thermography captures the autonomic temperature differences that occur when the nervous system is under mechanical stress at the upper cervical level.
If those screens point toward upper cervical involvement, we move to imaging. Neckwise uses CBCT 3D imaging as a precision tool to visualize the atlas and axis in three dimensions. Unlike a flat X-ray, CBCT produces a true three-dimensional model of the upper cervical region and quantifies the misalignment in degrees and millimeters across all axes of motion. This level of precision matters because the upper cervical spine does not misalign in just one direction — it can shift forward, rotate, and tilt in combination, and addressing one component without the others does not fully resolve the underlying problem.
Related article
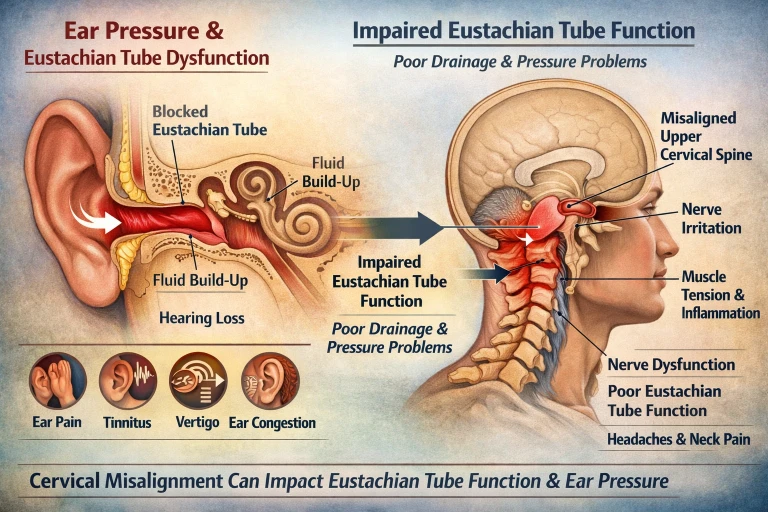
Why Won’t My Ear Pop? Eustachian Tube Dysfunction Relief in Sarasota and Bradenton
Mar 14, 2026The Correction: No Twisting, No Popping, No Pulling
The Neckwise correction is not what most people picture when they hear the word chiropractic. There is no twisting of the neck, no cracking or popping sound, and no forceful pulling or sudden movement of the head. This is particularly important for vestibular patients, because forceful manipulation of an already irritated vestibular system can provoke severe symptoms and is appropriately avoided.
Instead, the patient lies on their side on a precisely engineered table. The doctor uses the measurements taken from the CBCT imaging to determine the exact angle and direction needed to guide the atlas back toward its ideal position. The correction itself is delivered as a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place. The intent is to give the body a precise mechanical input that allows it to release the misalignment on its own terms.
Because the correction is so specific and so gentle, it is appropriate for patients who are in active vertigo, patients who have been told they are not candidates for traditional chiropractic care, patients with prior neck injuries, and patients who are simply uncomfortable with the idea of forceful neck manipulation. The vestibular system needs to settle, not be provoked further. The Neckwise approach is built around that principle.
What Happens After the Correction
When the upper cervical spine is restored toward its ideal position, several things begin to change. The suboccipital muscles no longer have to hold a sustained, asymmetric contraction, and they slowly begin to release. The flood of corrupted positional data into the vestibular nuclei diminishes. The brainstem starts to receive a cleaner reference signal, and the vestibular system gains the conditions it needs to recalibrate.
Patients commonly report that the dizziness becomes less constant, the episodes less severe, and the recovery between episodes faster. Motion sensitivity decreases. Brain fog clears in steps rather than all at once. The associated symptoms — neck tension, head pressure, ear fullness, sleep disruption — often improve in parallel, because they share the same underlying mechanical cause. Healing in the vestibular system is rarely linear, and a corrective program is structured over weeks to months precisely because the nervous system needs time to reorganize around the new input.
Upper cervical care is also designed to integrate alongside the rest of a patient's care team. We do not ask patients to stop vestibular therapy, abandon medication, or skip ENT and neurology appointments. Our role is to address a specific mechanical and neurological factor that is consistently overlooked, and to bring that piece into the broader picture so the system as a whole has the best chance of recovery.
Finding Real Answers in Sarasota
If you are searching for a vestibular neuritis treatment specialist in Sarasota — and especially if you have been told the inflammation should have resolved by now, but your dizziness, brain fog, or imbalance has lingered for months — an upper cervical evaluation may be a meaningful next step. The diagnostic line between a viral inflammation and a mechanical irritation of the vestibular system is far less clear than the conventional model suggests, and a measurable upper cervical contribution is something that can actually be tested for, imaged, and addressed.
Upper Cervical chiropractic focuses on patients who have not found lasting answers in the conventional system. The combination of objective testing, CBCT 3D imaging, and a precise correction with no twisting, popping, or pulling offers a structured, evidence-based way to determine whether the upper cervical spine is part of your vestibular picture — and if it is, to address it at the source.
To learn more or schedule a consultation, contact Neckwise Sarasota. Recovery from vestibular dysfunction is rarely simple, but for many patients, it begins with looking in a place the standard workup has not yet looked.



Leave a comment