
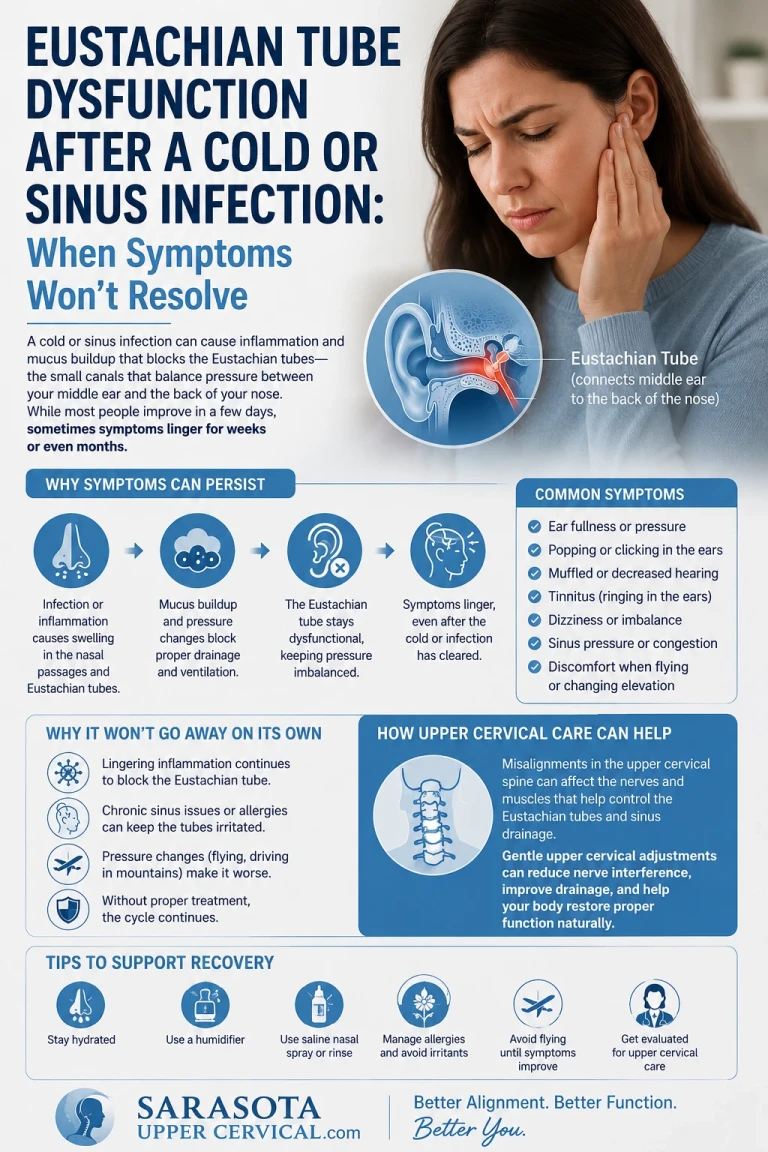
"Eustachian Tube Dysfunction After a Cold or Sinus Infection: When Symptoms Won't Resolve
The cold is gone. The sinus infection has cleared. But your ears are still blocked, your hearing is still muffled, and the pressure won't go away. For many patients, the answer to why recovery has stalled lies in the upper cervical spine — and addressing it may be the missing piece"
The pattern is familiar to many patients. A cold or sinus infection takes hold. The runny nose, the congestion, the cough, the general feeling of illness all work through their typical course over a week or two. The acute infection resolves. Energy returns. The body feels recovered. But the ears do not get the message. The fullness that started during the infection persists. The muffled hearing continues. The pressure that should have resolved within days of the infection clearing remains weeks later. Patients return to normal activity assuming their ears will catch up, but they don't. Days become weeks. Weeks become months. The ears remain in the post-infection state long after every other symptom has resolved.
Schedule Your Appointment
Schedule appointmentThis is post-infectious Eustachian tube dysfunction (ETD) that has failed to resolve, and it is one of the most common entry points into chronic ETD. Most patients who get colds or sinus infections recover their ear function within two to three weeks as inflammation subsides and the Eustachian tube returns to normal function. A substantial subset, however, does not. The infection clears but the tube does not return to normal. The patient is left with persistent ETD that may continue for months, become chronic, or progress to broader symptoms involving hearing, balance, and quality of life.
The honest question is why some patients recover fully and others don't. The infection itself is not different — these are the same viruses, the same bacteria, the same upper respiratory conditions that affect billions of people. What differs is the underlying state of the system when the infection hits and the underlying capacity for recovery afterward. For a substantial portion of patients with persistent post-infectious ETD, that underlying state involves the upper cervical spine and the structural and neurological factors that depend on it.
This article focuses on the upper cervical case for understanding and addressing persistent post-infectious ETD. The mechanisms by which craniocervical structural problems compromise Eustachian tube function are anatomical, neurological, and vascular. The reasons some patients don't recover from infections that others handle without lasting consequence often trace back to these underlying structural factors. For Sarasota patients whose ears have been stuck in the post-infection state for weeks or months, understanding what may be holding back recovery clarifies why upper cervical evaluation may be the path forward when other approaches haven't helped.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
When Post-Infectious ETD Becomes Persistent
Understanding the difference between normal recovery and persistent dysfunction clarifies when something more is at work than just infection aftermath.
What normal recovery looks like
Normal post-infectious recovery follows a recognizable pattern. During acute infection, the Eustachian tube becomes obstructed by mucosal swelling, increased mucus production, and inflammation in the nasopharynx and surrounding tissues. Ear pressure, fullness, muffled hearing, and sometimes pain develop. As the infection resolves over one to two weeks, the inflammation subsides, mucosal function returns to normal, mucus clears, and the Eustachian tube returns to its baseline function. By two to three weeks after the acute infection, most patients have normal ear function again. The system was designed to handle this kind of insult and recover from it.
When recovery stalls
For some patients, this recovery does not happen. The acute infection resolves but the ear symptoms persist. Three weeks pass. Four weeks. Six weeks. Three months. The pressure remains. The hearing stays muffled. The fullness continues. Some patients describe the symptoms as fluctuating — worse with weather changes, allergies, stress, or any minor congestion. Others describe persistent steady symptoms that don't vary much. Either way, the system has not returned to baseline, and the failure of recovery suggests underlying factors compromising the system's capacity to heal.
The signs of persistence
Persistent post-infectious ETD typically involves several recognizable features. Ear fullness or pressure that has continued beyond three weeks past the resolution of the acute infection. Muffled hearing or sense of hearing being underwater. Crackling or popping sounds with swallowing or jaw movement. Sometimes mild dizziness or unsteadiness. Sometimes ear pain, particularly with weather changes or congestion. The symptoms may affect one ear or both. The persistence is the key feature — these symptoms should have resolved as the infection cleared, and they haven't.
Why this matters
Persistent post-infectious ETD is not simply slow recovery from an infection. It represents the underlying capacity for recovery being inadequate to restore normal function. Something is holding the system in the dysfunctional state. Understanding what may be holding it there is the path to addressing it. For many patients, the answer involves the upper cervical spine and the structural and neurological factors that the cervical region influences.
Related article
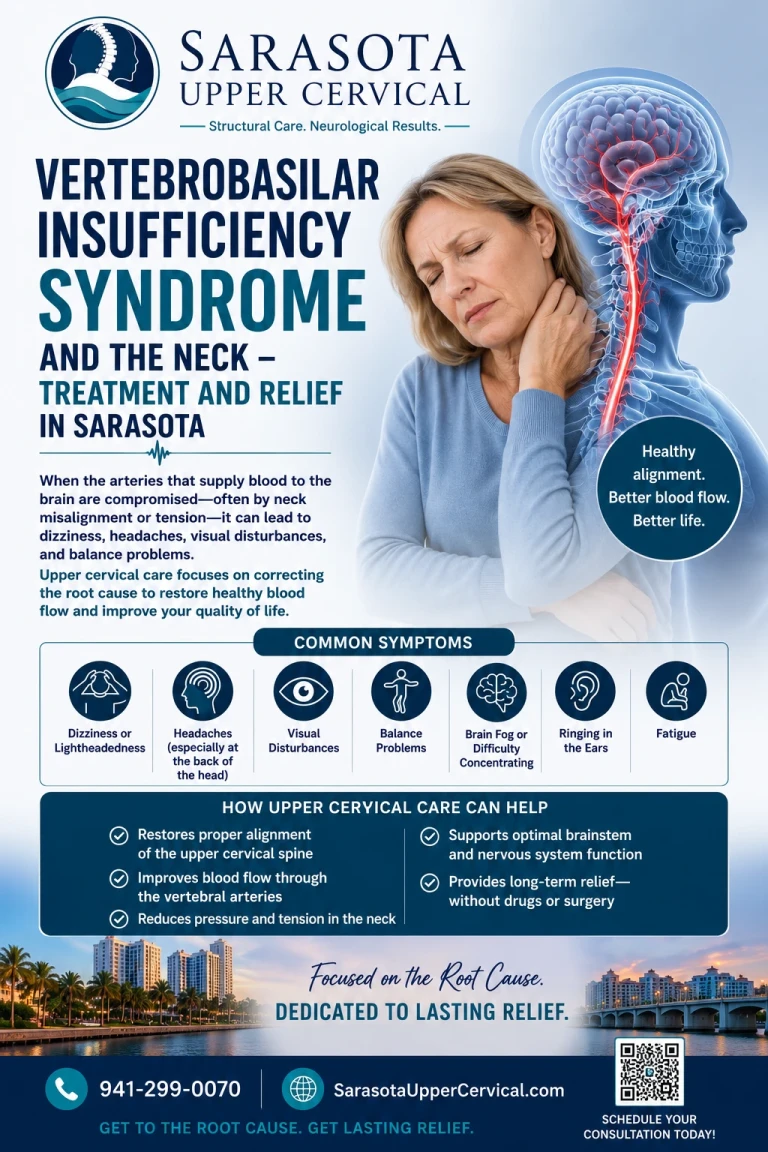
vertebrobasilar insufficiency syndrome and the neck - treatment and relief in Sarasota
Jun 23, 2026Why the Upper Cervical Spine Matters for Eustachian Tube Recovery
The Eustachian tube does not exist in isolation. Its function depends on muscular control, neural regulation, vascular supply, mucosal health, and structural relationships — all of which connect back to the upper cervical region in specific anatomical ways. Understanding these connections clarifies why structural cervical problems can compromise the system's capacity to recover from infections that should resolve normally.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
The tensor veli palatini and its trigeminal control
The Eustachian tube is opened primarily by the tensor veli palatini muscle. When this muscle contracts during swallowing, it pulls the cartilaginous portion of the tube open, allowing pressure equalization and drainage. The muscle is innervated by the mandibular branch (V3) of the trigeminal nerve. The trigeminal nuclei are located in the brainstem, with the spinal trigeminal nucleus extending down into the upper cervical region. The 2003 paper by Bartsch and Goadsby in Current Pain and Headache Reports established the anatomical convergence of trigeminal and upper cervical input in what is known as the trigeminocervical complex (Bartsch & Goadsby, 2003).
What this means for post-infectious ETD recovery is direct. The neural pathways controlling the muscle that must open the Eustachian tube run through and integrate with the upper cervical region. Structural problems at this level — chronic compensatory muscle tension, altered proprioceptive input, distorted neural signaling environment — affect the broader function of the trigeminal system. The muscle that must work efficiently to restore Eustachian tube function may not have the optimal neural environment when craniocervical structural problems persist. The system needed to recover is the system that craniocervical problems compromise.
The cervical sympathetic chain and mucosal recovery
Recovery from post-infectious mucosal inflammation depends on appropriate sympathetic regulation of vascular tone and mucosal function. The cervical sympathetic chain runs along the cervical spine, with the superior cervical ganglion located near the upper cervical region. This ganglion sends fibers to multiple targets including the mucosa of the nasopharynx, the lining of the Eustachian tube, and surrounding tissues. Sympathetic regulation affects blood flow, mucus production, mucosal tone, and inflammatory resolution.
When upper cervical structural problems affect the cervical sympathetic chain — through proximity, altered mechanics, or surrounding tissue tension — the sympathetic regulation of mucosal recovery may be compromised. The inflammation that should resolve doesn't fully resolve. The mucus production that should normalize doesn't normalize. The mucosal tone that should return to baseline doesn't return. The system needed to clear the post-infectious state cannot do its job adequately because the regulatory input is being affected by structural cervical factors.
The brainstem control environment
Beyond the specific nerve pathways, the broader brainstem environment affects multiple systems involved in Eustachian tube function. The cervical proprioceptive input feeds into brainstem processing through dense pathways. The 2001 study by Kulkarni and colleagues in Neurology India documented the exceptional muscle spindle density in suboccipital muscles (Kulkarni et al., 2001) — these muscles generate disproportionate proprioceptive output that feeds into brainstem processing. When this input is distorted by chronic compensatory tension from craniocervical structural problems, the brainstem environment in which multiple control systems operate is affected.
The trigeminal control of the tensor veli palatini, the autonomic regulation of mucosal recovery, the vestibular processing that integrates with auditory function, and various other systems all operate within this brainstem environment. Persistent distorted cervical input affects the broader functional state in ways that may compromise multiple systems simultaneously, including the system responsible for Eustachian tube function and recovery.
The fascial and structural continuity
The Eustachian tube runs through anatomical regions with fascial and structural relationships extending back to the upper cervical region. The deep cervical fascia, the prevertebral fascia, the carotid sheath, and the various muscular and connective tissue layers create continuity between cervical structures and the regions surrounding the Eustachian tube. The 1995 paper by Hack and colleagues in Spine documented direct connective tissue continuity between the rectus capitis posterior minor muscle and the spinal dura mater (Hack et al., 1995) — establishing that cervical muscles have direct mechanical relationships with structures often considered distinct. The broader fascial network connecting cervical and upper aerodigestive structures provides mechanical pathways by which cervical structural problems may affect Eustachian tube anatomy and function.
The cumulative effect on recovery capacity
The cumulative effect of these multiple mechanisms is that craniocervical structural problems can affect the system's overall capacity to recover from insults that healthy systems handle routinely. When an infection produces acute inflammation and Eustachian tube dysfunction, a system with optimal underlying function returns to baseline as inflammation resolves. A system with compromised underlying function from craniocervical structural problems may not return to baseline because the capacity for recovery has been reduced. The infection serves as a stress that exposes the underlying compromise, and the inability to recover is the visible expression of what was operating more subtly before the infection.
Related article
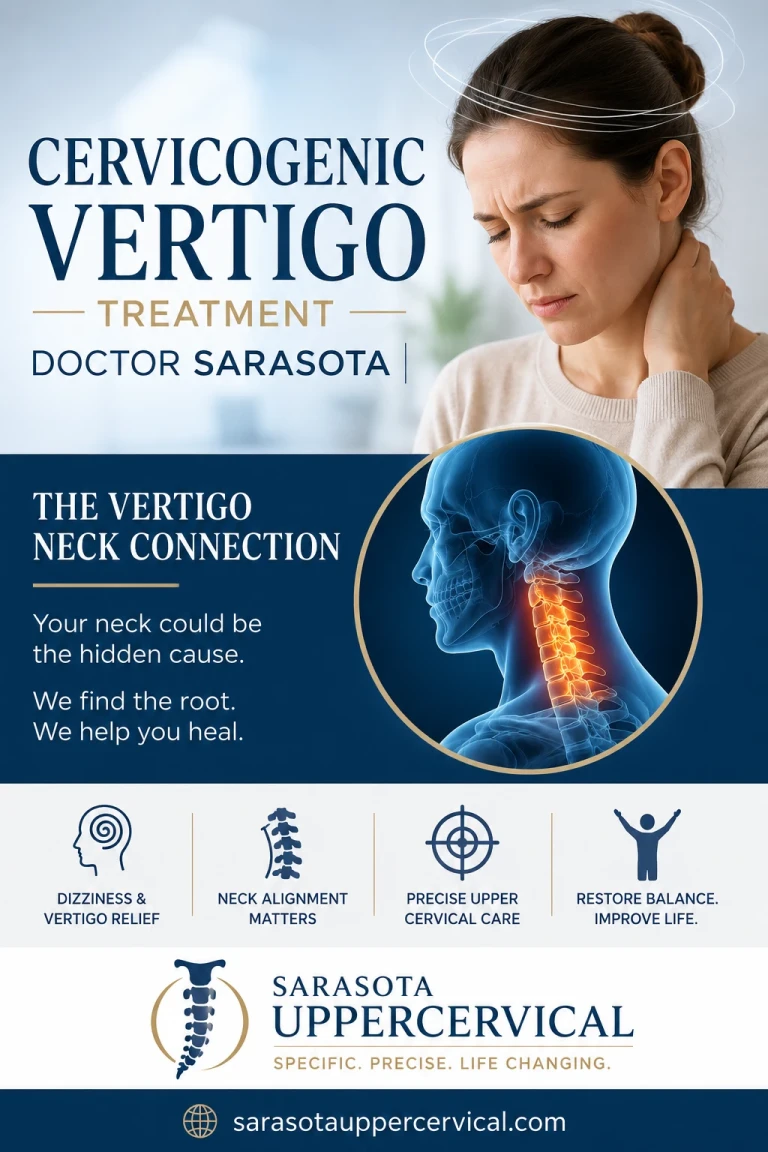
Cervicogenic vertigo treatment and Doctor in Sarasota | The vertigo Neck connection
Jun 25, 2026Why Some Patients Recover and Others Don't: The Structural Hypothesis
The patient with chronic post-infectious ETD often asks why their experience differs from family members or coworkers who had the same cold and recovered fully. The structural hypothesis provides one answer: underlying baseline differences in the systems supporting Eustachian tube function.
Patients with prior trauma history
Patients who developed persistent post-infectious ETD often have prior history of head or neck trauma. The trauma may have been years or decades earlier — a car accident in their twenties, a sports injury in college, a fall, a workplace injury, a whiplash from a minor fender-bender. The 2005 study by Kaale and colleagues in the Journal of Neurotrauma documented that whiplash mechanisms produce upper cervical ligamentous injuries at forces below those required for diagnosable concussion (Kaale et al., 2005). The cervical structural injury from these events often persists for years without producing prominent standalone symptoms but creates the underlying compromise that makes recovery from other insults difficult.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Patients with chronic postural factors
Modern life produces sustained postural challenges to the upper cervical region. Hours of screen time with forward head posture, sustained desk work, phone use producing constant downward head position, sleeping positions that compromise cervical alignment, and various other postural factors create chronic compensatory tension in cervical structures. The cumulative effect over years builds up to the kind of subtle structural problems that compromise underlying function without producing dramatic symptoms. When infection hits, the compromised baseline limits recovery capacity.
Patients with multiple cervical-region symptoms
Patients with persistent post-infectious ETD often have other symptoms suggesting cervical involvement. Chronic neck pain. Suboccipital tension. Headaches that center at the base of the skull. Restricted cervical range of motion. Cervicogenic dizziness features. These symptoms point to the underlying cervical structural picture that may also be compromising Eustachian tube recovery. The pattern of multiple cervical-region symptoms alongside the persistent ETD suggests they share a common contributing factor.
Why family members recovered
Family members who had the same infection and recovered fully typically did not have the same underlying cervical compromise. Their baseline function supported full recovery. The patient with persistent ETD had the same exposure but a different baseline. This is not a moral or behavioral difference — it's a structural and neurological difference in the systems that determine recovery capacity. Recognizing this clarifies that persistent post-infectious ETD reflects something specific about the individual patient's underlying state rather than something they did wrong or are doing wrong now.
What Upper Cervical Evaluation Involves at Sarasota Upper Cervical
For patients whose post-infectious ETD has stalled and who suspect underlying cervical factors may be involved, upper cervical evaluation provides specific assessment of the structural picture.
Three-dimensional CBCT imaging
The evaluation begins with three-dimensional cone beam computed tomography of the upper cervical region. This imaging produces a true 3D reconstruction of the craniocervical anatomy and measures alignment with precision to within fractions of a degree. Standard X-rays cannot visualize this region with the detail needed to identify subtle structural problems. The 3D imaging reveals the actual relationships between the skull, atlas (C1), and axis (C2) and identifies whether structural problems are present at this critical anatomical level.
Objective testing before any intervention
Beyond imaging, objective testing including leg length analysis and paraspinal infrared thermography is performed before any adjustment is considered. The principle is that corrections should be delivered only when objective findings indicate a structural shift is present. Patients without objective findings indicating need for correction do not receive corrections. This restraint guided by data is particularly important — interventions are evidence-based rather than performed routinely on assumption that problems must be present.
Precision-based corrections when indicated
When objective findings indicate a structural shift, corrections are delivered specific to the upper cervical segment and along a calculated vector based on the imaging measurements. There is no twisting. There is no popping. There is no full-spine manipulation. The force is low and the precision is high. The approach is designed for the kind of careful structural correction that the upper cervical region requires, not the aggressive manipulation that some chiropractic approaches use.
What correction may accomplish for post-infectious ETD
When upper cervical structural correction is appropriate and effective, the various downstream factors discussed earlier may begin to normalize over time. The compensatory muscle tension may decrease, allowing the broader neural environment to improve. The distorted proprioceptive input to brainstem processing may normalize. The cervical sympathetic chain function may improve as surrounding mechanical and inflammatory factors resolve. The cumulative effect on the system's recovery capacity may improve. For appropriate patients, this may translate to the stalled recovery from post-infectious ETD finally moving forward. For other patients, the effect may be smaller or take longer. Either outcome provides useful clinical information about what the cervical contribution was to the broader picture.
Related article
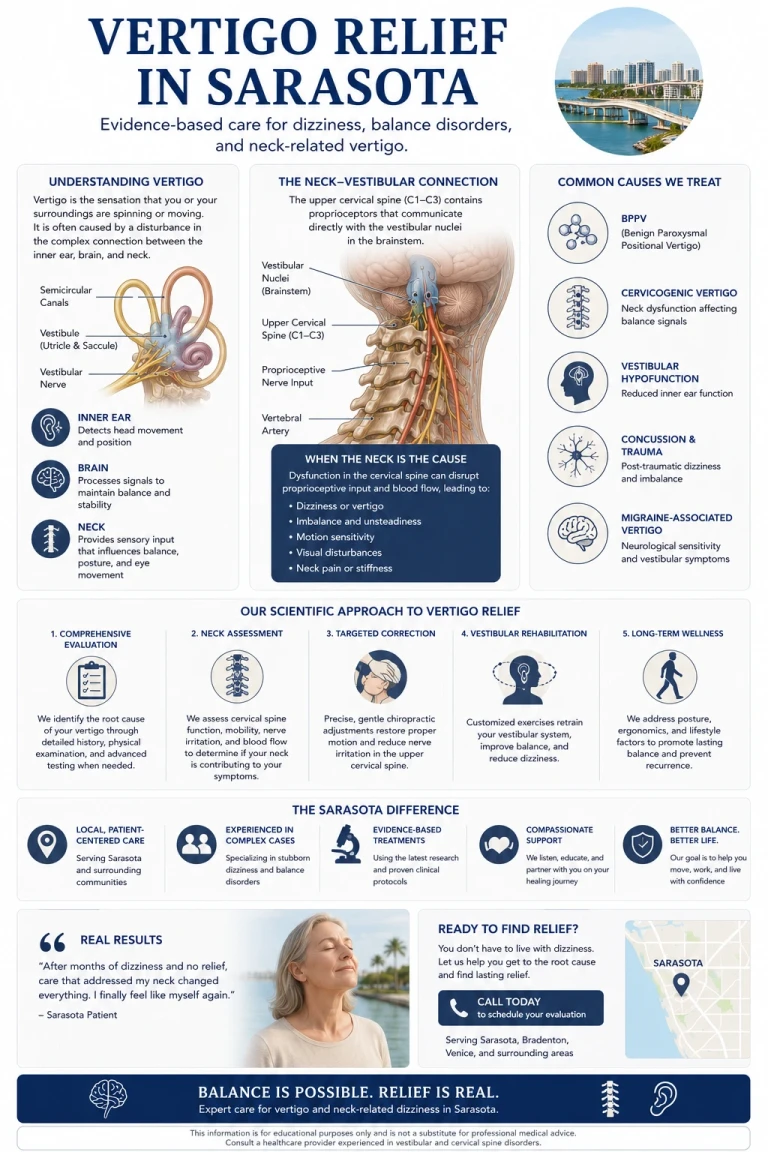
Find Vertigo Relief in Sarasota | How Your Neck Can Be at the Root Cause of Vertigo
May 13, 2026The timeline of response
Patients should set realistic expectations about timeline. Structural correction does not produce immediate ETD resolution. The system needs time to adapt to the corrected structural picture, for compensatory muscle patterns to normalize, for inflammatory and mucosal factors to resolve, and for the cumulative effect to translate into symptomatic improvement. Response typically develops over weeks to months when it occurs. Multiple corrections over the course of care may be needed. Patience with the process matters because the underlying changes take time to translate into functional improvement.
When to Consider Upper Cervical Evaluation for Persistent Post-Infectious ETD
Upper cervical evaluation at Sarasota Upper Cervical may be worth considering for persistent post-infectious ETD when:
Your ETD symptoms have continued more than three to four weeks after the acute infection cleared. You have associated cervical symptoms — chronic neck pain, suboccipital tension, restricted cervical range of motion, cervicogenic headache. You have prior head or neck trauma in your history — concussion, whiplash, sports injury, fall. You have other conditions that may share cervical structural contributions — tinnitus, vestibular symptoms, TMJ dysfunction, chronic headaches. You have postural factors suggesting chronic cervical compromise — long hours of computer use, forward head posture, chronic muscle tension. You feel your recovery has stalled and standard approaches haven't moved it forward.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
Important Considerations
Patients with persistent post-infectious ETD should also pursue appropriate medical evaluation. ENT or primary care evaluation establishes the diagnosis, rules out conditions that may mimic ETD, identifies any specific factors requiring medical intervention, and provides medical management as appropriate. Upper cervical evaluation complements rather than replaces medical care.
Severe symptoms, sudden hearing loss, severe pain, vertigo with associated neurological symptoms, or other concerning features require prompt medical evaluation rather than chiropractic care.
Patients should ensure any chiropractic provider they see uses precision-based low-force techniques rather than aggressive cervical manipulation. The approach matters — the precision-based protocols used at Sarasota Upper Cervical are fundamentally different from aggressive manipulation, and the difference matters for safety and effectiveness.
Where to Go From Here
Persistent post-infectious ETD reflects underlying factors compromising the system's capacity to recover from insults that should resolve normally. For many patients, the underlying compromise involves the upper cervical spine and the structural, neurological, and vascular factors that depend on it. The trigeminal control of the tensor veli palatini muscle that opens the Eustachian tube, the cervical sympathetic regulation of mucosal recovery, the broader brainstem environment shaped by cervical proprioceptive input, and the fascial continuities connecting cervical structures to the upper aerodigestive region all create pathways by which craniocervical structural problems may compromise the recovery the system should be capable of.
Patients whose ETD has been stuck in the post-infection state for weeks or months, particularly those with associated cervical symptoms, prior trauma history, or other features suggesting cervical involvement, may benefit from comprehensive evaluation including upper cervical structural assessment. The evaluation identifies whether structural cervical factors are present and addressable. When they are present and corrected through precision-based intervention, the system's underlying capacity for recovery may begin to restore — and the stalled post-infectious ETD may finally start to move forward.
At Sarasota Upper Cervical, we focus specifically on the precise structural relationship between the skull, atlas, and axis. Our approach uses three-dimensional CBCT imaging and objective testing to identify whether structural problems are contributing to your persistent ETD, with precision-based corrections delivered only when objective findings indicate they are appropriate. We work alongside your medical providers rather than replacing them, providing a specific component of comprehensive evaluation that may be the missing piece for your recovery.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
Kaale, B. R., Krakenes, J., Albrektsen, G., & Wester, K. (2005). Head position and impact direction in whiplash injuries: Associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. Journal of Neurotrauma, 22(11), 1294–1302.
Schilder, A. G., Bhutta, M. F., Butler, C. C., Holy, C., Levine, L. H., Kvaerner, K. J., Norman, G., Pennings, R. J., Poe, D., Silvola, J. T., Sudhoff, H., & Lund, V. J. (2015). Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clinical Otolaryngology, 40(5), 407–411.
Bluestone, C. D. (2005). Eustachian Tube: Structure, Function, Role in Otitis Media. PMPH-USA.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Gdowski, G. T., & McCrea, R. A. (2000). Neck proprioceptive inputs to primate vestibular nucleus neurons. Experimental Brain Research, 135(4), 511–526.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with persistent post-infectious ETD should pursue appropriate medical evaluation by ENT, otolaryngology, or primary care specialists. Upper cervical evaluation is considered a complementary approach rather than a primary treatment for ETD. Patients with sudden hearing loss, severe pain, vertigo with associated neurological symptoms, or other concerning features should seek prompt medical evaluation. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment