
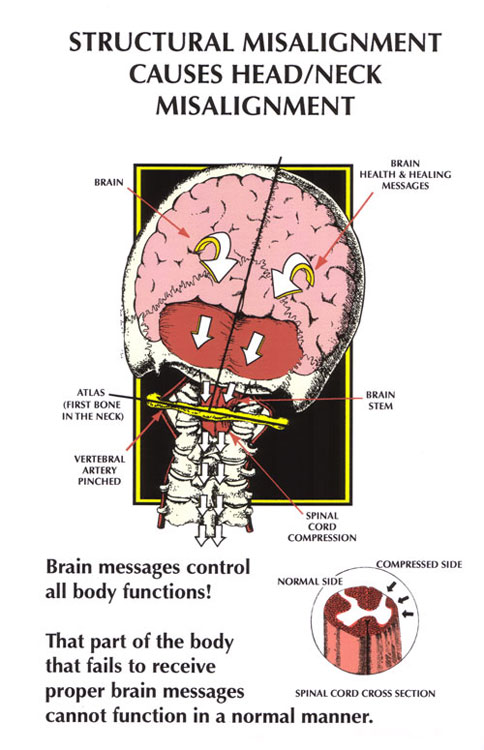
If you live in Sarasota and have been told your dizziness is "just anxiety," an inner-ear problem, or something you'll have to live with, but no treatment has actually resolved it — there's a mechanism worth understanding. For a meaningful number of people, the source of the spinning, swaying, and unsteadiness isn't the inner ear at all. It's the upper neck.
This form of dizziness is called cervicogenic vertigo (also called cervicogenic dizziness, or CGD). It happens when the joints, muscles, and sensory nerves of the cervical spine send faulty position information to the brainstem. The inner ear can be perfectly healthy, yet the brain still produces the experience of vertigo, because the neck signal it depends on to make sense of head position has become unreliable.
Schedule Your Appointment
Schedule appointmentAt Sarasota Upper Cervical, our care focuses on the function of the top two vertebrae of the neck, the atlas (C1) and axis (C2) — the exact region most densely wired for balance. Below, we'll walk through the neurology of why the neck can drive vertigo, why an injury to a single joint can set off a long cascade, and how a precise, well-held upper cervical correction fits into the picture.
The neck is a balance organ, not just a support structure
Most people think of balance as a job for the inner ear and the eyes. Those two systems matter enormously, but they are only two of three. The third is cervical proprioception: the constant stream of "where is my head in space" information generated by sensory receptors in the joints and muscles of the neck.
Your brainstem fuses these three inputs, vestibular (inner ear), visual (eyes), and proprioceptive (neck and body) — into a single, unified sense of orientation. When the three agree, you feel steady. When they conflict, the brain experiences a sensory mismatch, and the result can be dizziness, unsteadiness, visual disturbance, and a foggy, disoriented feeling.
What makes the upper neck special is its receptor density. The suboccipital region — the small muscles at the very base of your skull — contains a higher concentration of proprioceptors than almost any other region of the body, reflecting how critical it is for orienting the head. When that region stops moving and signaling correctly, the brain loses one of its most important balance references.
The proprioceptive pathway: a direct line from your neck to your balance centers
This isn't a vague, indirect relationship. There is a literal anatomical wiring diagram connecting the upper neck to the brain's balance machinery.
Sensory receptors in the upper cervical joints and deep neck muscles send signals through the upper cervical nerve roots into the brainstem, where they feed directly into the vestibular nuclei, the same cluster of cells that processes inner-ear signals. Research describes a cervico-vestibular pathway in which proprioceptive input from cervical receptors projects into the medial and inferior vestibular nuclei, the structures responsible for keeping the head and eyes oriented in space.
In other words, your neck and your inner ear pour their signals into the same processing hub. The brainstem cannot tell the difference between "my head turned" and "my neck sent a turning signal." If the neck sends a movement signal when the head didn't actually move, or fails to send one when it did, the brainstem registers a contradiction with the eyes and inner ear. That contradiction is felt as vertigo.
The simple version: Your brainstem expects the inner ear, the eyes, and the neck to all tell the same story about where your head is. When a damaged or restricted upper neck tells a different story, the brain can't reconcile it, and produces cervicogenic dizziness.
The muscle spindle problem: chronically unbalanced occipital muscles
The proprioceptive signal from the neck comes largely from muscle spindles — tiny stretch sensors woven into muscle that report length and change in length. The suboccipital muscles (rectus capitis posterior major and minor, obliquus capitis superior and inferior) are packed with a dense concentration of muscle spindles relative to their small size, which is precisely why they function as fine-tuning instruments for head position rather than as movers.
Here's where chronic dysfunction becomes a problem. When the upper cervical joints sit in a subtly rotated or laterally shifted position, the suboccipital muscles on one side are held in a shortened state and the muscles on the other side in a lengthened state. That asymmetry isn't just a posture issue — it is a sensory issue. The spindles on each side are now reporting from a chronically unbalanced baseline, feeding asymmetric and inaccurate length information into the vestibular nuclei.
The literature notes that even prolonged contraction of the neck muscles on one side can significantly alter the sensitivity of the neck's proprioceptors, and that muscle spasm, fatigue, and pain all distort spindle output. So a neck that is held off-center day after day doesn't just feel tight — it continuously feeds the brain a distorted map of where the head is pointing. The vestibular nuclei dutifully integrate that distorted map, and the person feels persistently "off."
The myodural bridge: when neck tension reaches the brainstem's doorstep
There's a second anatomical connection that makes the upper neck even more influential than its size suggests — the myodural bridge.
The myodural bridge is a band of connective tissue that physically links the deep suboccipital muscles — primarily the rectus capitis posterior minor, but also the rectus capitis posterior major and obliquus capitis inferior, to the dura mater, the membrane that surrounds the spinal cord and brainstem. It is a direct, hard-wired bridge between muscle and the covering of the central nervous system.
This connection matters in two ways. First, it is a tension-monitoring system: tone in these small muscles is mechanically transmitted to the dura, and sudden movements such as hyperflexion-extension (whiplash) injuries transmit traction forces straight through the bridge to the cervical dura. Second, research has shown the bridge plays a role in the normal pumping and circulation of cerebrospinal fluid with head movement.
The practical takeaway: chronically unbalanced suboccipital muscles don't just create faulty spindle signals, through the myodural bridge they create abnormal, asymmetric tension on the dura right at the level of the brainstem and the vestibular nuclei. The region driving the dizziness and the region housing the balance centers are mechanically and neurologically intertwined.
The real starting point: loss of joint motion after a capsule injury
So what sets this whole cascade in motion? In a large share of cases, it traces back to a single event: trauma to an upper cervical joint capsule that leaves the joint with reduced, altered motion.
Related article
Each spinal joint is wrapped in a capsule that is densely supplied with sensory nerve endings. Studies of human cervical facet capsules have identified multiple types of mechanoreceptors plus free nerve endings, proving these tissues are actively monitored by the central nervous system and confirming that input from the facets is important to both proprioception and pain sensation.
Now consider what a whiplash, fall, sports collision, or other trauma does to that capsule. Excessive stretch injures it. Research on cervical facet capsules has shown that the strain magnitudes associated with whiplash-like loading are the same magnitudes that injure the capsular ligament and trigger abnormal, prolonged firing in its sensory neurons, including afterdischarge, where the neurons keep firing even after the load is removed. The capsule's receptors, in other words, can be left in a chronically over-firing, miscalibrated state.
The cascade from one bad joint
This is the core of the upper cervical perspective. A single injured, motion-restricted joint capsule starts a self-reinforcing loop:
The capsule's mechanoreceptors give bad input. A damaged, restricted joint either under-reports or over-reports motion. The brainstem receives a corrupted signal about head position from that segment.
That bad input is sent straight to the vestibular nuclei. Through the cervico-vestibular pathway, the faulty joint signal conflicts with the eyes and inner ear — sensory mismatch — and dizziness results.
Reflex muscle responses follow. Capsule receptors have direct reflex connections to the surrounding neck muscles. Researchers have hypothesized that damage to the mechanoreceptors in the facet joint capsule can produce corrupted muscular activation patterns, meaning the injured capsule reflexively drives the suboccipital muscles into the chronically unbalanced, asymmetric state described earlier.
The muscle imbalance feeds back as more bad spindle input. Those now-asymmetric muscles send distorted spindle signals back into the same vestibular nuclei, and tug abnormally on the dura through the myodural bridge.
The loop sustains itself. Bad joint input drives muscle imbalance, muscle imbalance reinforces the bad input, and the brain stays locked in mismatch. Over time the brain can even "reweight" toward these faulty signals, which is part of why cervicogenic dizziness so often becomes chronic and resistant to inner-ear treatments.
This is why chasing the symptom rarely resolves it. Vestibular exercises, medications, and inner-ear maneuvers are all working downstream of the actual driver. If the upstream problem is a restricted, miscalibrated upper cervical joint feeding bad input into the system, the logical target is that joint.
The upper cervical approach: restore motion, restore the signal
Upper cervical chiropractic care focuses on the atlas (C1) and axis (C2) for a specific reason: this is where the proprioceptive density is highest, where the myodural bridge attaches, and where small misalignments have the largest neurological consequence. The goal is not to "pop" the neck or to chase a feeling. The goal is to restore normal motion and normal sensory input to the segment that has been driving the mismatch.
Why CBCT imaging comes first
Because the correction is precise, the analysis has to be precise. At Sarasota Upper Cervical we use cone beam computed tomography (CBCT) — a 3D imaging technology that shows the true, three-dimensional position of the upper cervical vertebrae far more accurately than a flat 2D X-ray can.
A misalignment that drives the cascade above may be a matter of a few degrees of rotation or a small lateral shift. CBCT lets us measure that misalignment in three dimensions and design a correction tailored to that individual's anatomy, rather than applying a generic, forceful manipulation. For a problem rooted in faulty signaling from a specific joint, knowing the precise geometry of that joint is the difference between guessing and correcting.
The principle of "holding" the adjustment
Here is a principle that sets upper cervical care apart, and it matters enormously for cervicogenic vertigo. The objective is not to get adjusted as often as possible, it's to hold the correction for as long as possible.
Think back to the cascade. The nervous system became locked into a faulty pattern over time. Once a precise correction restores normal joint position and motion, the brainstem finally starts receiving accurate input again — but the system needs time in that corrected state to recalibrate, for the muscle imbalance to settle, and for the sensory reweighting to reverse. Every time the segment slips back out, the clock resets.
This is why we measure how long a correction holds and adjust only when the objective findings show it's needed, rather than on a fixed repetitive schedule. A correction that holds for weeks gives the nervous system the stable, accurate signal it needs to unwind a chronic pattern. In our experience, the patients who do best are the ones whose corrections hold — because holding is what gives the brain the uninterrupted runway to recalibrate balance. (Individual responses vary, and this is a general description of how the approach works, not a promise of any specific outcome.)
Could your dizziness be coming from your neck?
Cervicogenic vertigo is worth considering — especially if some of these fit your history:
Your dizziness started after a car accident, fall, concussion, whiplash, or other head/neck trauma, even one from years ago.
Your dizziness and your neck pain or stiffness tend to come and go together, or worsen with certain neck positions.
Inner-ear testing came back normal, or inner-ear treatments didn't fully resolve your symptoms.
You feel "off," foggy, unsteady, or disoriented more than truly "spinning."
You've been told there's nothing structurally wrong, yet the dizziness persists.
Cervicogenic dizziness is a clinical evaluation, and other causes of dizziness, some of them serious, need to be ruled out by appropriate examination. A thorough upper cervical assessment is designed to determine whether your neck is a contributing factor and whether you're a candidate for this type of care.
Get a clear answer about your dizziness
If you're in the Sarasota area and your dizziness hasn't been explained, or hasn't responded to inner-ear-focused treatment, a focused upper cervical evaluation, including 3D CBCT analysis, can help identify whether your neck is part of the problem.
Schedule Your Consultation-941 259-1891
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization is made or implied. Dizziness and vertigo can have many causes, some of them serious, and should be evaluated by a qualified healthcare provider. Individual results vary, and no specific outcome is guaranteed. The mechanisms described reflect current scientific literature on cervicogenic dizziness and upper cervical neurology; they are explanatory and do not predict results in any particular case. Always consult your physician or a licensed healthcare professional regarding your symptoms.



Leave a comment