
Trigeminal Neuralgia Treatment and Relief in Sarasota — Understanding the Upper Cervical Connection
Trigeminal neuralgia (TN) is one of the most severe pain conditions in all of medicine — sudden, electric, stabbing pain in the face that can be triggered by something as light as a breeze, a touch, chewing, or brushing your teeth. It is sometimes called the “suicide disease” because of how relentless and life-altering it can be. If you are living with it, you already know that, and you are likely searching for any avenue of trigeminal neuralgia relief that conventional approaches haven’t fully provided.
Schedule Your Appointment
Schedule appointmentThis guide explores a connection that is often overlooked: the relationship between the upper neck and trigeminal pain. There is genuine neuroanatomy linking the two, real published case reports describing improvement with upper cervical care, and a logical, candidate-appropriate role for evaluating the neck in some people with facial pain. We’ll also be honest about what the evidence does and doesn’t yet show, because you deserve straight information, not hype.
Wondering whether the upper neck could be part of your facial pain? Schedule a free consultation to find out whether you are a candidate for care. Call 941-259-1891.
Listen to one of our pateint's recovery stories from trigeminal neuralgia in our office. Click here.
What Is Trigeminal Neuralgia?
The trigeminal nerve is the fifth cranial nerve, and it is the main sensory nerve of the face. It has three branches that supply sensation to the forehead and eye region (the ophthalmic branch), the cheek and upper jaw (the maxillary branch), and the lower jaw (the mandibular branch). When this nerve misfires, the result is trigeminal neuralgia: episodes of intense facial pain, usually on one side, often described as electric shocks, stabbing, or burning.
The pain frequently has “trigger zones” — specific spots or activities that set off an attack, such as talking, eating, shaving, applying makeup, or even a light wind on the face. Between attacks there may be no pain at all, or, in some forms, a constant background ache. Because the pain can mimic dental problems, many people undergo dental procedures before TN is correctly identified.
The Types of Trigeminal Neuralgia
“Trigeminal neuralgia” is not a single uniform condition. Understanding which type you may be dealing with matters, because the types differ in their pain pattern, their likely cause, and how they respond to various approaches.
Type 1 (Classic / Typical TN)
Type 1, or classic trigeminal neuralgia, is the most recognizable form: sudden, sharp, electric-shock-like jolts of pain that come in episodes lasting seconds to a couple of minutes, often in clusters, with pain-free intervals in between. In classic TN, the underlying cause is frequently a blood vessel compressing the trigeminal nerve where it exits the brainstem, which over time wears on the nerve’s protective coating. This is important context: when the cause is true vascular compression at the brainstem, that specific problem is a medical and sometimes surgical matter, not something the neck creates.
Type 2 (Atypical TN)
Atypical trigeminal neuralgia involves a more constant, burning, aching, or throbbing pain, often with a lower-grade background pain present much of the time, sometimes alongside the sharper electric episodes. Atypical TN is generally considered more difficult to treat than the classic form, and it tends to respond less predictably to the standard approaches. This is one of the forms where a broader look at all contributing factors — including the neck — can be especially worth considering, precisely because conventional treatment so often falls short.
Symptomatic / Secondary TN
Symptomatic (secondary) trigeminal neuralgia is facial pain caused by an identifiable underlying condition affecting the nerve, such as multiple sclerosis or a tumor pressing on the nerve. This is why proper medical evaluation is essential: it ensures that a serious secondary cause is identified or ruled out before anything else is considered.
Pre-Trigeminal Neuralgia and TN Mimics
Some people experience a “pre-trigeminal” phase — a dull, aching, or toothache-like discomfort that precedes the development of classic shooting pain. Just as importantly, several other conditions can mimic TN, including cervicogenic facial pain referred from the neck, dental conditions, TMJ disorders, and occipital neuralgia. Distinguishing true TN from its mimics is a critical step, and it is one place where the neck connection becomes directly relevant — because some facial pain attributed to the trigeminal nerve is actually being driven or amplified by the upper neck.
Is it tmj or is it Tn? How to tell the difference click here.
The Neck Connection: Why the Upper Cervical Spine Matters
Here is the central idea of this guide, and it rests on real, well-documented neuroanatomy rather than speculation. The trigeminal nerve and the upper cervical nerves do not operate in isolation — they are wired together in the brainstem. Understanding that wiring explains how a problem in the neck can influence pain in the face.
The Trigeminocervical Complex (The Master Mechanism)
Deep in the lower brainstem and upper spinal cord lies a region where the sensory fibers of the trigeminal nerve and the upper cervical nerves (C1, C2, and C3) converge onto the same neurons. This integrated region is called the trigeminocervical complex (or trigeminocervical nucleus). It is, in effect, a shared switchboard for sensation from the face and the upper neck.
This convergence was first demonstrated experimentally decades ago, and it is now well established that it allows the bidirectional referral of pain between the neck and the face. In plain terms: because face signals and neck signals plug into the same neurons, the brain can misinterpret a problem originating in the upper neck as pain in the face. This is the same mechanism that explains cervicogenic headaches — and it provides a direct anatomical pathway by which upper cervical dysfunction could contribute to trigeminal pain.
Critically, this system can become sensitized. Research notes that neck trauma, whiplash, strain, or chronic muscle spasm can increase the sensitivity of this region, lowering the pain threshold so that the system fires more easily and pain becomes more severe. A sensitized trigeminocervical complex is a plausible amplifier of facial pain — and the upper neck is a key input into it.
Additional Pathways: Why Several Routes Point to the Upper Neck
The trigeminocervical complex is the primary mechanism, but it is not the only proposed pathway. Part of what makes the upper cervical connection compelling is that several plausible routes all converge on the same region. These are proposed mechanisms grounded in anatomy, presented as such rather than as proven cause-and-effect:
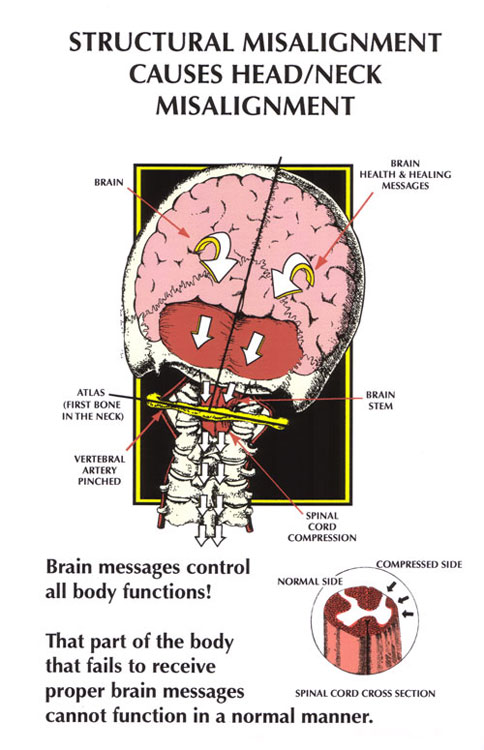
Brainstem Irritation
The trigeminal nerve’s sensory nucleus extends down into the brainstem and upper cervical cord — the very region the atlas (C1) and axis (C2) surround. When the upper cervical spine is misaligned, it has been proposed that abnormal mechanical stress in this area can irritate the brainstem region where trigeminal signals are processed, contributing to the hypersensitivity that characterizes the condition.
The Myodural Bridge
The myodural bridge is a dense band of connective tissue that physically connects the deep suboccipital muscles at the base of the skull to the dura mater, the membrane surrounding the brainstem and spinal cord. When upper cervical misalignment produces chronic tightness in these suboccipital muscles, that tension can be transmitted through the myodural bridge to the dura around the brainstem — another proposed route by which upper neck dysfunction may create irritation in the region where trigeminal pain is generated and modulated.
Aberrant Proprioceptive Input
The upper cervical spine contains an exceptionally high density of proprioceptors — position and movement sensors that continuously inform the brainstem about head position. When the upper cervical joints are misaligned, this input becomes distorted. Because that faulty proprioceptive stream feeds into the same brainstem regions that process and modulate pain, aberrant input from the neck may contribute to the abnormal pain processing seen in trigeminal neuralgia, effectively turning up the system’s sensitivity.
Altered Vascular and Cerebrospinal Fluid Dynamics
Finally, the upper cervical region is a critical junction for blood flow and cerebrospinal fluid movement around the brainstem. It has been proposed in the upper cervical literature that misalignment may contribute to altered vascular and cerebrospinal fluid flow in this region, adding to the abnormal neurological environment around the trigeminal pathway. This pathway is more speculative than the others, and we present it as a proposed contributor under continued study.
The throughline across all of these: the upper neck is anatomically positioned, through multiple routes, to influence the brainstem region where trigeminal pain lives. That convergence of mechanisms is exactly why correcting upper cervical alignment is worth evaluating in the right candidate.
What the Research and Case Reports Show — Honestly
This is where it is important to be straight, because your decisions deserve accurate information. The neuroanatomy above is well-established. The clinical evidence for upper cervical care specifically resolving trigeminal neuralgia is more preliminary — it consists primarily of case reports and small case series, which are encouraging but are the early, hypothesis-generating end of the evidence spectrum, not large randomized trials.
Within that honest framing, the published reports are genuinely interesting. A peer-reviewed case series examined five people with chronic, severe, daily trigeminal neuralgia who received a low-force upper cervical technique (Atlas Orthogonal) over an eight-week period. Of the five, four reported reduced trigeminal neuralgia pain, two experienced complete cessation of their pain, and three were able to reduce their medication dosage. Separately, a published case report documented a 62-year-old woman with two years of facial pain diagnosed as trigeminal neuralgia who received a low-force upper cervical technique (NUCCA), with significant reductions in the frequency, duration, and affected area of her pain.
Related article
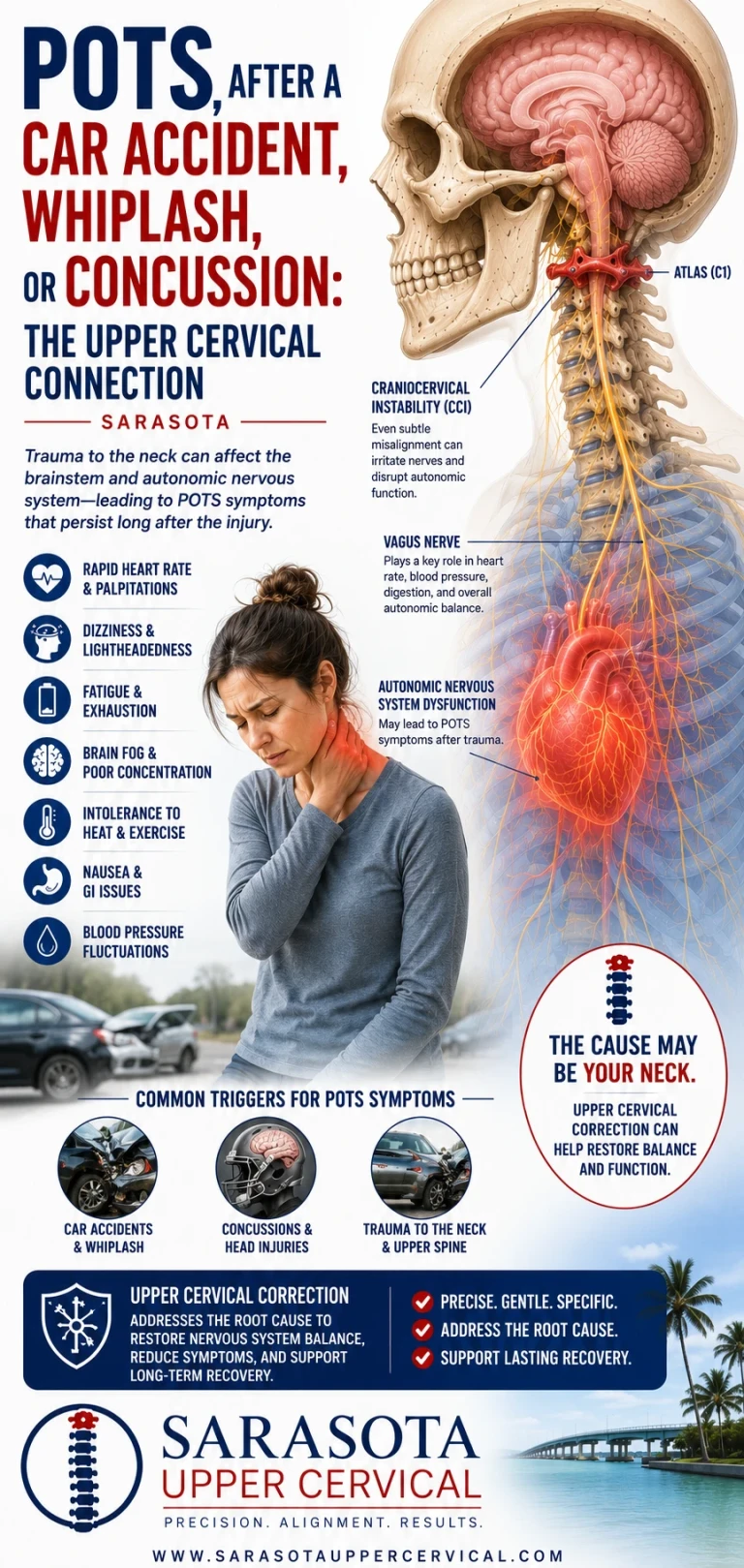
POTS After a Car Accident, Whiplash, or Concussion: The Upper Cervical Connection | Sarasota
Jul 28, 2026The authors of this work propose that some trigeminal neuralgia sufferers may have an upper cervical misalignment that creates a brainstem-related combination of abnormal neurological tone and altered vascular and cerebrospinal fluid flow, producing heightened pain sensitivity — and that gentle, low-force methods aimed at normalizing head position may help ease those changes. That is a reasonable hypothesis consistent with the anatomy. What it is not, yet, is proof that upper cervical care reliably resolves TN for everyone. Anyone promising guaranteed resolution is overstating the evidence. The honest position is this: there is a credible mechanism and encouraging early reports, which together make upper cervical evaluation a reasonable option to consider — especially for those whom conventional care hasn’t fully helped.
How Upper Cervical Care Approaches Facial Pain
Upper cervical chiropractic focuses on the alignment of the atlas (C1) and axis (C2) — the region most intimately connected, through the pathways above, to the trigeminal system. The goal is not to claim a cure, but to determine whether a correctable upper cervical component is contributing to your pain, and if so, to address it as part of your broader care.
Precision Through 3D Imaging
Before any correction, detailed 3D imaging (CBCT) is used as a precision measurement tool to analyze your individual anatomy and measure the exact position of the atlas. Given how small and critical this region is, and how individual each person’s structure is, this precision is essential to a tailored, appropriate correction.
Gentle Corrections — No Twisting, Popping, or Yanking
Corrections are gentle and specific, with no twisting, popping, or yanking of the neck. This is particularly relevant for people in severe pain and with a sensitized nervous system. Notably, the published reports describing benefit used exactly these kinds of low-force methods. Precision is what allows a light, specific correction rather than force.
Candidacy First — and Working Alongside Your Doctors
Not everyone with facial pain has an upper cervical component, and not everyone is a candidate. A thorough evaluation determines whether the structural signs are present, and will tell you honestly if they are not. Upper cervical care is intended to work alongside your neurologist and medical team — not to replace medication, and never to delay evaluation of a serious underlying cause. For classic TN driven by true vascular compression, medical and surgical options remain central; the upper cervical role is complementary and candidate-specific.
Who Might Consider an Upper Cervical Evaluation?
It may be worth evaluating the upper neck if you:
• Have facial pain that began or worsened after head or neck trauma, whiplash, or a concussion
• Have atypical TN or facial pain that hasn’t responded well to conventional treatment
• Notice neck pain, headaches, or tension accompanying your facial pain
• Have been told your imaging doesn’t show clear vascular compression
• Suspect your “TN” may actually be, or be mixed with, neck-referred facial pain
A proper evaluation — always after appropriate medical assessment — can determine whether the upper neck is part of your picture.
Wondering whether the upper neck could be part of your facial pain? Schedule a free consultation to find out whether you are a candidate for care. Call 941-259-1891.

Frequently Asked Questions
Can a problem in my neck really cause facial pain?
Yes, through well-documented anatomy. The trigeminal nerve (face) and the upper cervical nerves (neck) converge on the same neurons in a brainstem region called the trigeminocervical complex. This convergence allows pain to be referred between the neck and the face, which is how upper cervical dysfunction can contribute to or amplify facial pain, and why some facial pain is actually neck-referred.
What are the types of trigeminal neuralgia?
The main forms are Type 1 (classic/typical), with sudden electric-shock-like episodes; Type 2 (atypical), with more constant burning or aching pain that is harder to treat; and symptomatic/secondary TN, caused by an identifiable condition such as MS or a tumor. There is also a pre-trigeminal phase of dull, toothache-like pain, and several mimics including cervicogenic facial pain, TMJ disorders, and occipital neuralgia.
Does upper cervical care cure trigeminal neuralgia?
No one should promise that. The evidence for upper cervical care in TN consists of encouraging case reports and small case series, not large clinical trials. They describe real people whose facial pain improved — in one series, four of five improved and two had complete cessation of pain — but this is preliminary evidence. Upper cervical care is best understood as a candidate-appropriate, complementary approach that addresses a potential neck-based contributor, alongside your medical care.
What does the research actually say?
The neuroanatomy linking the upper neck and the trigeminal system is well established. The clinical evidence for upper cervical correction in TN is early-stage: published case reports and a small case series using gentle, low-force techniques describe meaningful pain reduction in several patients, including some complete resolutions and medication reductions. The honest summary is a credible mechanism plus encouraging early reports, which makes evaluation reasonable — not a guarantee of results.
Is the care safe if I’m already in severe pain?
Upper cervical corrections are gentle and specific, with no twisting, popping, or yanking, and they are guided by detailed 3D imaging of your anatomy. The published reports describing benefit used exactly these low-force methods. Care begins with a thorough evaluation, works alongside your medical treatment, and never delays assessment of a serious underlying cause.
How do I find out if I’m a candidate?
Start with a consultation and evaluation, which may include 3D imaging to assess your upper cervical alignment. This determines whether a neck-based component may be contributing to your facial pain. If it isn’t, you’ll be told so. Call 941-259-1891 to schedule a free consultation.
This content is for informational purposes only and does not constitute medical advice. Trigeminal neuralgia requires medical evaluation, and serious underlying causes must be assessed by a physician. Upper cervical care does not cure trigeminal neuralgia; it addresses a potential structural contributor in appropriately screened candidates, alongside medical care. Individual results vary, and the clinical evidence is currently limited to case reports and small case series.



Leave a comment