
"Why the craniocervical junction is the choke point for cerebrospinal and venous drainage — and how upper cervical correction can help open it back up"
Idiopathic intracranial hypertension, often abbreviated as IIH and sometimes called pseudotumor cerebri, is a condition in which the pressure inside the skull is elevated without an obvious cause. The word idiopathic means without known origin, and that label captures the central frustration of this diagnosis. Patients are told their pressure is high, that the symptoms are real, and that the cause cannot be identified. Treatment typically focuses on lowering the pressure with medication, repeated lumbar punctures, weight management, or in more severe cases, surgical shunting of the cerebrospinal fluid.
Schedule Your Appointment
Schedule appointmentThese approaches can offer relief, but they share a common limitation. They manage the consequences of elevated intracranial pressure without fully answering the underlying mechanical question: why is the pressure rising in the first place, and what is preventing it from regulating itself the way it should?
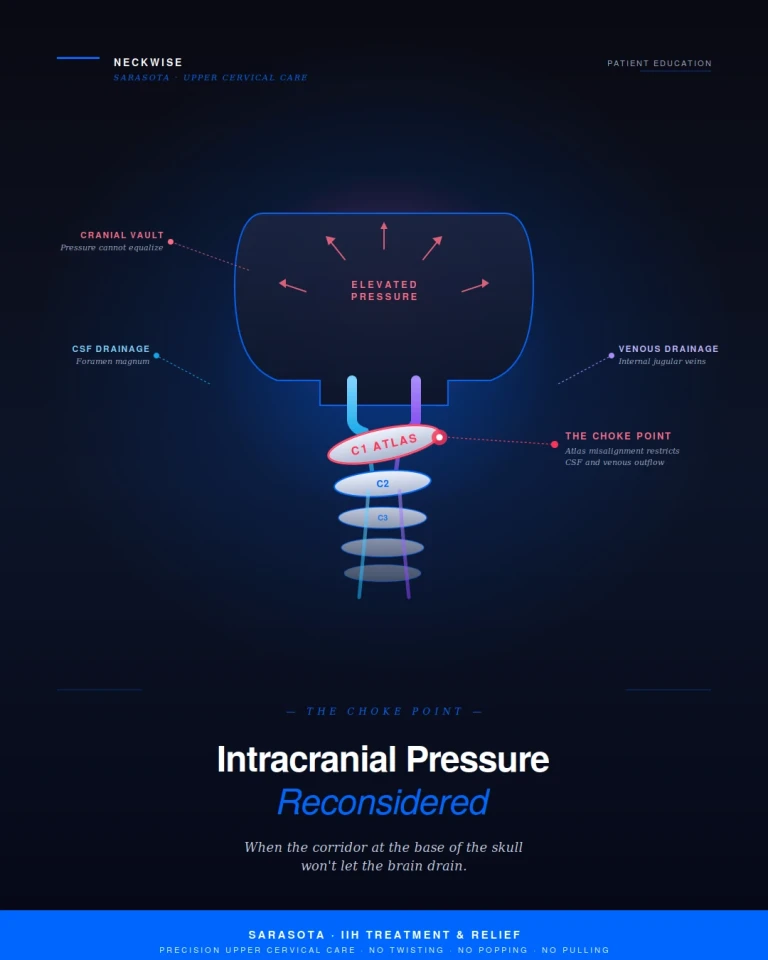
At Sarasota upper cervical, we focus on a part of the picture that the conventional workup rarely investigates. The fluids and vessels that govern intracranial pressure — cerebrospinal fluid and the venous drainage system — both pass through a single anatomical corridor at the base of the skull. That corridor is the craniocervical junction. When the atlas is misaligned, this corridor functions as a choke point, restricting the very drainage mechanisms responsible for keeping intracranial pressure in balance. For many patients carrying an idiopathic diagnosis, the cause is not unknown. It is simply being looked for in the wrong place.
What Idiopathic Intracranial Hypertension Is
The skull is a closed container. Inside it sit the brain, the cerebrospinal fluid that bathes and protects the brain, and the blood that supplies and drains it. The volume of these three components must remain in balance, because the skull cannot expand to accommodate excess. When any of these volumes increases without a corresponding decrease in the others, intracranial pressure rises.
Cerebrospinal fluid, or CSF, is produced continuously in the ventricles of the brain. It circulates around the brain and spinal cord and is reabsorbed primarily through specialized structures called arachnoid granulations and through cervical lymphatics. Venous blood drains from the brain through a network of dural sinuses that ultimately empty into the internal jugular veins, which carry the blood out of the skull and back to the heart. As long as production and drainage stay balanced, intracranial pressure remains within a narrow physiological range.
In idiopathic intracranial hypertension, that balance is lost. CSF production may be normal, but reabsorption or outflow is restricted. Venous drainage may be partially obstructed, raising back-pressure throughout the system. The pressure inside the skull rises, the brain is compressed against its own container, and the optic nerves — which are direct extensions of the brain itself — bear the visible consequences. This is why papilledema, swelling of the optic disc, is the classic clinical sign that confirms the diagnosis.
The Craniocervical Junction as a Choke Point
To understand why the upper cervical spine matters in this condition, it helps to look at where the drainage actually happens. The cerebrospinal fluid that circulates around the brain must move freely through the foramen magnum — the large opening at the base of the skull — to communicate with the spinal compartment. The internal jugular veins, which carry the majority of venous blood out of the cranial vault, exit the skull through a small opening called the jugular foramen, located just lateral to the foramen magnum and immediately adjacent to the atlas vertebra.
This is a tightly engineered space. The brainstem, the upper portion of the spinal cord, the vertebral arteries, the internal jugular veins, the dural sinuses near their exit points, and the cerebrospinal fluid pathway all share the same narrow corridor — measured in millimeters, not inches. When this corridor is anatomically clear and mechanically balanced, fluid moves through it as designed. When it is compromised, the consequences propagate upward into the cranial vault.

The atlas (C1) is the vertebra most directly involved. It surrounds the brainstem and the upper spinal cord, sits immediately below the jugular foramina, and is the structural foundation on which the skull rests. Unlike the rest of the spine, the atlas has no disc above or below it. It depends on a delicate balance of ligaments and small muscles to remain properly aligned. When the atlas shifts even a fraction of a millimeter out of its ideal position, the geometry of the entire craniocervical junction changes. The vessels and fluid pathways that pass through this corridor can be mechanically compromised — not occluded outright, but narrowed, kinked, or held under sustained pressure that limits free flow.
This is the choke point. CSF that should circulate freely between the cranial vault and the spinal canal encounters resistance at the foramen magnum. Venous blood that should drain out through the internal jugular veins encounters resistance at the jugular foramen. Pressure that should equalize cannot equalize. The system loses its ability to self-regulate, and the pressure inside the skull begins to rise.
Why the Diagnosis Is Often Called Idiopathic
Standard imaging used to evaluate IIH is generally focused on the brain itself, the ventricles, and the major dural sinuses. MRI and MR venography can identify large-vessel obstructions, tumors, or hydrocephalus. These are essential studies and they appropriately rule out serious pathology. What standard imaging is not designed to evaluate is the precise three-dimensional position of the atlas relative to the skull and the resulting mechanical impact on the structures passing through the craniocervical junction.
In other words, the conventional workup is excellent at answering the question, is there a tumor, a clot, or a structural lesion causing this. It is not designed to answer the question, is the upper cervical spine mechanically positioned in a way that restricts CSF and venous outflow. When that question is never asked, the cause appears to be unknown, and the case is labeled idiopathic. For a meaningful subset of patients, the cause is not unknown — it has simply not been measured.
Common Symptoms Associated with IIH
Patients with idiopathic intracranial hypertension typically present with a combination of pressure-driven and neurological symptoms. The pattern is recognizable, and the overlap with what we see in upper cervical dysfunction is significant. Common symptoms include:
• Severe headaches, often described as a deep pressure behind the eyes or at the base of the skull, frequently worse in the morning or after lying flat
• Visual disturbances, including blurred vision, transient visual obscurations, or temporary blackouts that last seconds at a time
• Pulsatile tinnitus, a rhythmic whooshing or pulsing sound in one or both ears that follows the heartbeat
• A sense of head fullness, head heaviness, or pressure that feels as if the head might burst
Related article
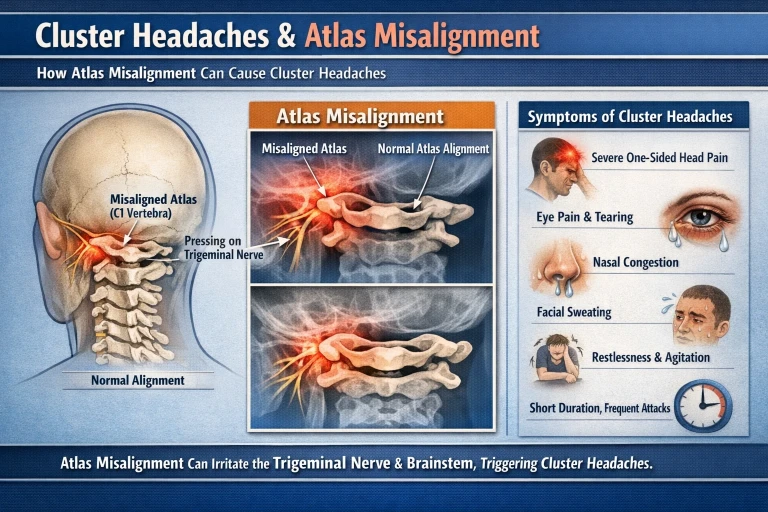
Cluster Headache Treatment in Sarasota & Bradenton | Upper Cervical Chiropractor Near Me
Mar 02, 2026• Neck pain, neck stiffness, or tension at the base of the skull
• Dizziness, brain fog, and difficulty concentrating
• Nausea, particularly in the morning or with positional changes
• Photophobia and phonophobia, a heightened sensitivity to light and sound
• Diplopia, or double vision, when the elevated pressure affects the cranial nerves controlling eye movement
• Papilledema identified on a dilated eye exam, which is the hallmark objective finding
Many of these symptoms are also classic markers of upper cervical dysfunction. Patients with atlas misalignment routinely describe the same head pressure, pulsatile tinnitus, neck-base tension, and brain fog — even in the absence of measurably elevated intracranial pressure on a lumbar puncture. This overlap is not coincidental. It reflects the shared underlying mechanism: a craniocervical junction that is not allowing the cranial vault to drain the way it should.
How Atlas Correction Helps Open the Choke Point
The logic of upper cervical care in this condition is mechanical and direct. If the geometry of the craniocervical junction is restricting CSF and venous outflow, then restoring the geometry should reduce that restriction and allow the drainage mechanisms to function more normally.
When the atlas is brought back toward its ideal position, several changes begin to occur. The space around the foramen magnum normalizes, allowing CSF to circulate more freely between the cranial vault and the spinal compartment. The mechanical stress on the jugular foramina eases, allowing the internal jugular veins to drain at their full capacity. The dural sinuses that empty into the jugular system are no longer working against an artificially raised back-pressure. The suboccipital muscles that have been holding a sustained, asymmetric contraction begin to release, removing additional mechanical compression from the surrounding structures.
As the system regains its ability to drain, intracranial pressure has the opportunity to recalibrate. The pressure-driven symptoms — head fullness, pulsatile tinnitus, behind-the-eye pressure, morning headaches, brain fog — often diminish in parallel because they share the same upstream cause. The improvements typically build in steps over weeks to months, not in a single visit, because the body needs time for inflammation to resolve, for the muscles to adapt to the new position, and for the entire fluid system to equilibrate around the restored geometry.
Related article
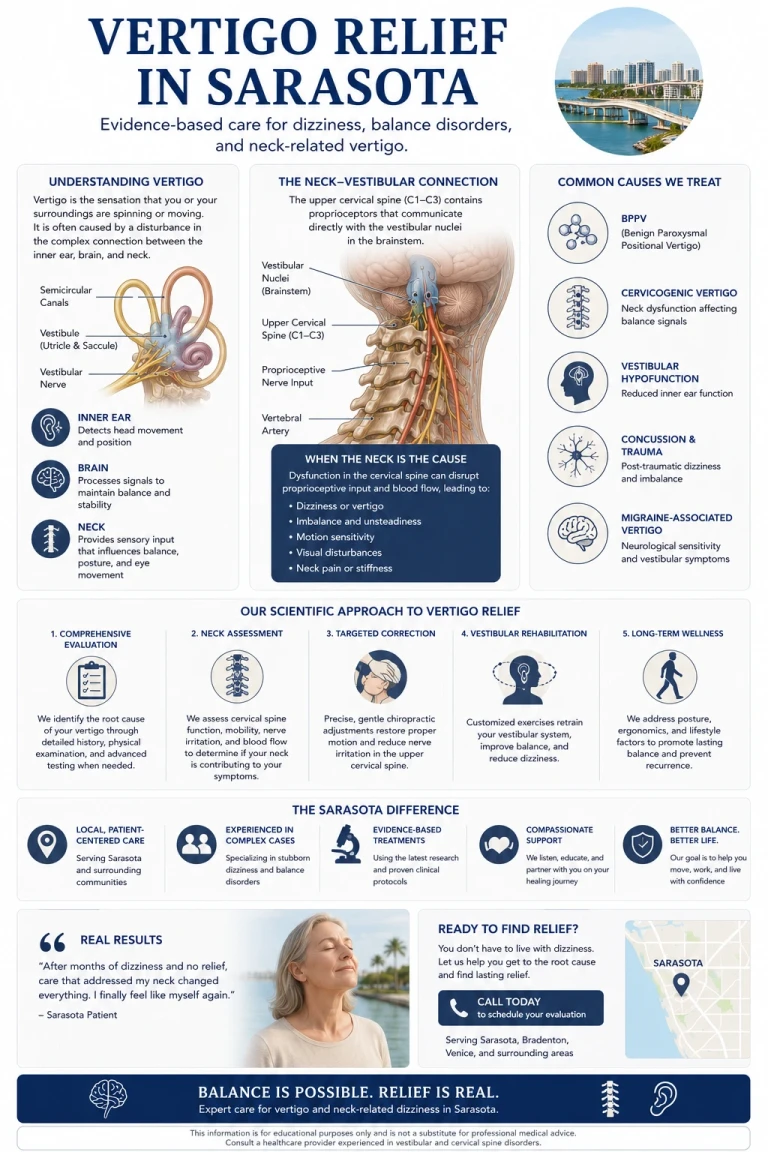
Find Vertigo Relief in Sarasota | How Your Neck Can Be at the Root Cause of Vertigo
May 13, 2026It is important to be honest about what this approach is and is not. Upper cervical care is not a replacement for medical management of IIH, particularly in patients with significant papilledema, threatened vision, or severely elevated pressure. The goal is not to compete with neurology or ophthalmology — it is to address a specific mechanical contributor that is consistently overlooked, and to do so in a way that integrates with the rest of the patient's care.
How We Evaluates and Corrects
The upper cervical chiropractic process is built around objectivity. We do not guess at whether a misalignment is present and we do not adjust based on how the neck feels to the touch. We measure.
The evaluation begins with a comprehensive consultation and history, with particular attention to prior trauma, the timeline of symptoms, prior imaging and treatments, and the full pattern of pressure-driven complaints. We then use objective testing — including a leg balance test and infrared thermography — to determine whether the nervous system is showing measurable signs of upper cervical involvement. These screens are repeatable, evidence-based, and provide a clear go or no-go signal for whether the upper cervical spine is part of the picture.
If the screens point toward upper cervical involvement, we move to imaging. Neckwise uses CBCT 3D imaging as a precision tool to visualize the atlas and axis in three dimensions. Unlike a flat X-ray, CBCT produces a true three-dimensional model of the upper cervical region, and the misalignment can be quantified in degrees and millimeters across all axes of motion. This level of precision is essential because the atlas does not misalign in just one direction. It can shift forward or backward, rotate, and tilt — often in combination — and addressing one component without the others does not fully resolve the underlying mechanical compromise.
The Correction: No Twisting, No Popping, No Pulling
The Neckwise correction is not what most people picture when they hear the word chiropractic. There is no twisting of the neck, no cracking or popping sound, and no forceful pulling or sudden movement of the head. This is particularly important for patients with elevated intracranial pressure, because forceful manipulation in this population is appropriately avoided.
Instead, the patient lies on their side on a precisely engineered table. The doctor uses the measurements taken from the CBCT imaging to determine the exact angle and direction needed to guide the atlas back toward its ideal position. The correction is delivered as a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place. The intent is to give the body a precise mechanical input that allows it to release the misalignment on its own terms.
Because the correction is so specific and so gentle, it is appropriate for patients who are managing IIH alongside their neurologist or ophthalmologist, patients with prior neck injuries, and patients who have been told they are not candidates for traditional chiropractic care. The system is fragile when intracranial pressure is elevated, and the approach is built around that reality.
Finding Real Answers in Sarasota
If you have been diagnosed with idiopathic intracranial hypertension and are searching for treatment and relief in Sarasota, an upper cervical evaluation may be a meaningful next step in your care. The word idiopathic does not mean the cause is permanently unknown. It means the cause has not yet been identified by the tests that have been ordered. The relationship between the atlas, the craniocervical junction, and the drainage mechanisms of the cranial vault is anatomical, measurable, and addressable — and for many patients, it represents the missing piece of a picture that has remained incomplete for years.
Neckwise focuses on patients who have not found lasting answers in the conventional system. Objective testing, CBCT 3D imaging, and a precise correction with no twisting, popping, or pulling offer a structured, evidence-based path to determine whether the upper cervical spine is contributing to your intracranial pressure — and if it is, to address it at the source so the body has the chance to drain, equalize, and recover.
To learn more or schedule a consultation, contact Neckwise Sarasota. The pressure inside your head is real, the symptoms are real, and the cause is rarely as unknown as the diagnostic label suggests. Often, the answer begins with looking at the corridor that everything has to pass through — the top of the neck.



Leave a comment