
"Why patients with systemic lupus erythematosus have measurably reduced vagal tone, what the research says about restoring autonomic balance, and how upper cervical care addresses the structural piece of the puzzle"
Systemic lupus erythematosus, or SLE, is one of the most complex autoimmune diseases in modern medicine. The body produces antibodies that target its own tissues, and the resulting inflammation can affect virtually every organ system — joints, skin, kidneys, heart, lungs, brain, and blood. Patients describe lupus as exhausting, unpredictable, and isolating. The disease has periods of flare and periods of remission, but for many patients, true remission feels elusive even with aggressive medical management.
Schedule Your Appointment
Schedule appointmentConventional treatment focuses on immunosuppression — antimalarials like hydroxychloroquine, corticosteroids, immunosuppressants, and biologics. These can effectively reduce disease activity, but they do not restore the body's natural ability to regulate its own immune response. Patients are often left managing a chronic condition rather than recovering from it.
Over the last two decades, the science of neuroimmunology has begun to change how researchers understand lupus. A growing body of peer-reviewed evidence shows that patients with SLE have measurable autonomic dysfunction — specifically, reduced vagal tone and elevated sympathetic activity — and that this autonomic imbalance is connected to the inflammatory state that drives the disease. At Neckwise in Sarasota, we focus on a specific, structural contributor to that autonomic imbalance: the position of the upper cervical spine and its direct effect on the brainstem and vagus nerve.
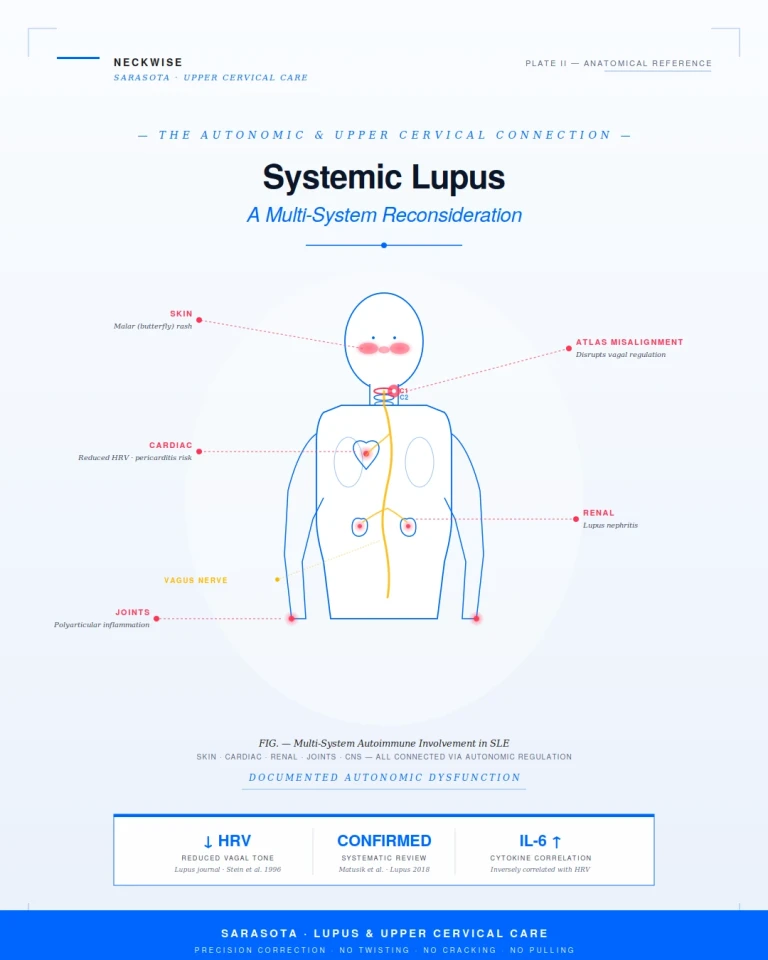
Documented Autonomic Dysfunction in Lupus
The connection between lupus and autonomic dysfunction is not speculative. It has been documented across multiple peer-reviewed studies over the past three decades, using a measurement called heart rate variability (HRV). HRV is a non-invasive index of autonomic balance, and the high-frequency component specifically reflects vagal (parasympathetic) activity. Lower HRV indicates reduced vagal tone.
A foundational study published in the journal Lupus found that lupus patients had significantly reduced heart rate variability compared to age- and gender-matched controls — and that this reduction was present whether or not the patients were receiving corticosteroid therapy. The finding suggested that autonomic dysfunction is intrinsic to the disease rather than a side effect of treatment.
Stein KS, McFarlane IC, Goldberg N, Ginzler EM. Heart rate variability in patients with systemic lupus erythematosus. Lupus, 1996. Time and frequency domain heart rate variability indices were significantly reduced in SLE patients compared to controls, with or without corticosteroid treatment.
A 2018 systematic review published in the journal Lupus consolidated decades of research and concluded that patients with systemic lupus erythematosus consistently demonstrate abnormal heart rate variability that reflects cardiac autonomic dysfunction, and that this dysfunction is correlated with inflammatory cytokines including interleukin-6 and C-reactive protein.
Matusik PS, Matusik PT, Stein PK. Heart rate variability in patients with systemic lupus erythematosus: a systematic review and methodological considerations. Lupus, 2018. Patients with SLE consistently show abnormal heart rate variability reflecting cardiac autonomic dysfunction, which may be related to inflammatory cytokines.
Related article
Whiplash and Neck Pain After a Car Accident: What Sarasota Drivers Should Know
Jul 19, 2026More recent work has continued to build on this. A 2022 study published in Sensors directly compared autonomic function in healthy individuals and in patients with rheumatoid arthritis or systemic lupus erythematosus, and concluded that both autoimmune populations have impaired vagus nerve function and that this impairment is a potential target for therapeutic intervention.
Liboriussen CH, et al. Sensors, 2022. Rheumatoid arthritis and systemic lupus erythematosus are associated with impaired autonomic nervous system and vagus nerve function. Both deep breathing and transcutaneous vagus nerve stimulation produced measurable improvements in vagal tone.
These findings, taken together, establish a clear pattern: lupus patients carry a measurable, persistent reduction in vagal tone, and this reduction is connected to the chronic inflammation that defines the disease. Restoring vagal tone has therefore become an active target of research.
How the Upper Cervical Spine Affects Vagal Function
If reduced vagal tone is part of the lupus picture, then anything that mechanically supports or compromises vagus nerve function is clinically relevant. The vagus nerve emerges from the brainstem at the level of the medulla and exits the skull through the jugular foramen — an opening located immediately adjacent to the atlas vertebra at the very top of the spine. From there it descends through the neck in close proximity to the cervical spinal cord and the deep neck muscles.
When the atlas is misaligned, the geometry of this entire region changes. The brainstem can be subjected to sustained mechanical stress. The jugular foramen narrows. The deep neck muscles hold compensatory contractions that compress the soft tissue corridor through which the vagus nerve descends. The autonomic regulation that the brainstem governs — including the cholinergic anti-inflammatory pathway through the vagus nerve — degrades under these conditions.
Research on upper cervical spinal manipulation has demonstrated measurable shifts in autonomic balance following correction. The 2015 Win et al. randomized cross-over study showed that upper cervical manipulation specifically — not general cervical manipulation — produced significant increases in time-domain heart rate variability indices, indicating enhanced parasympathetic (vagal) activity. The Bakris et al. 2007 randomized controlled trial published in the Journal of Human Hypertension demonstrated that a single precise atlas correction produced clinically significant blood pressure reductions sustained over time, an effect attributed to improved brainstem-mediated autonomic regulation.
Bakris G, et al. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: a pilot study. Journal of Human Hypertension, 2007. Restoration of atlas alignment was associated with marked and sustained reductions in blood pressure, attributed to improved autonomic regulation.
These findings do not establish upper cervical care as a treatment for lupus. They establish that the structural conditions at the upper cervical spine measurably influence the autonomic nervous system — the same autonomic nervous system documented as dysregulated in lupus across multiple decades of research. Addressing one of the structural factors that supports vagal function is a reasonable, mechanistically grounded piece of a broader care plan.
Related article
Common Symptoms in Lupus Patients We See
Patients with systemic lupus erythematosus who come to Neckwise typically present with a wide-ranging combination of symptoms that touch nearly every system in the body. The pattern often points back to autonomic dysregulation and chronic neuroinflammation in addition to the disease-specific symptoms. Common patterns include:
• Joint pain, particularly in the hands, wrists, and knees
• Profound, persistent fatigue that is not relieved by rest
• Brain fog and difficulty with memory and concentration ('lupus fog')
• Photosensitivity and the characteristic facial rash
• Heart palpitations, lightheadedness on standing, and other autonomic symptoms
• Heightened sensitivity to stress, light, and exertion
• Sleep disturbance and unrefreshing sleep
• Headaches and migraines, particularly during flares
Related article
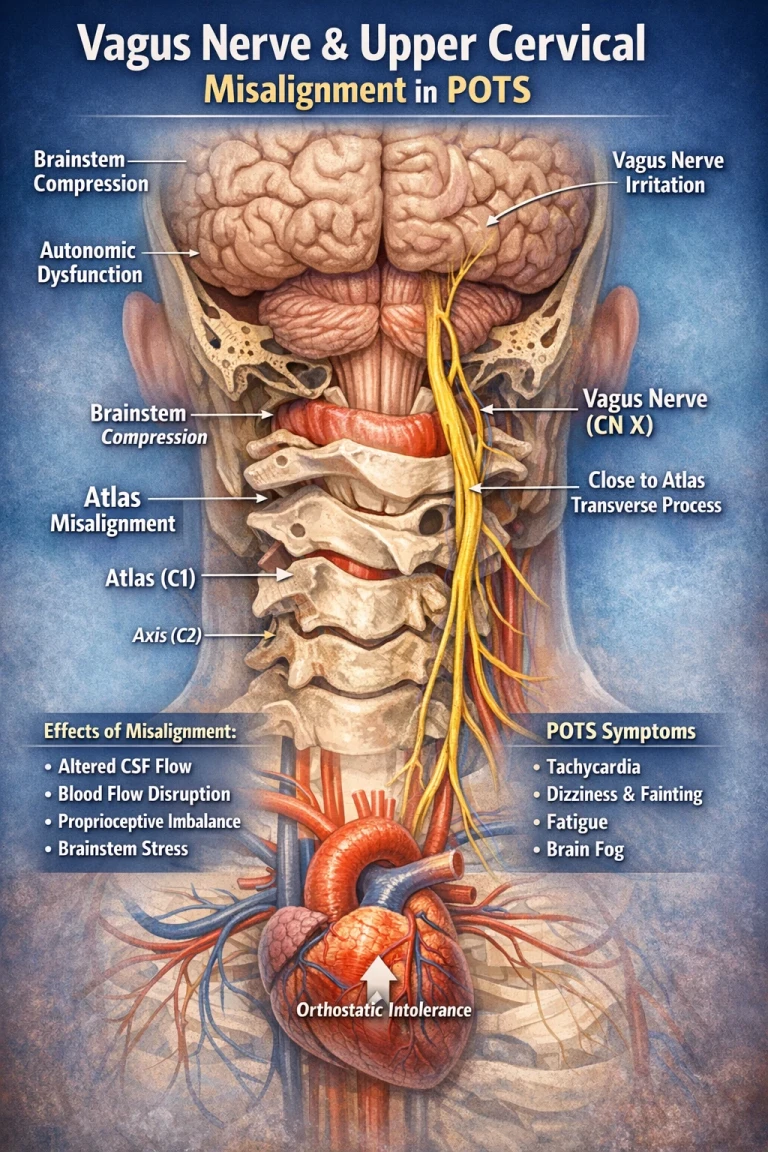
How the Vagus Nerve Drives POTS Symptoms: The Brainstem and Atlas Connection
Apr 09, 2026• Digestive symptoms and altered gut motility
• Neck pain, neck stiffness, or tension at the base of the skull
• A history of head or neck trauma — sometimes recent, often years or decades old
How Neckwise Approaches Lupus Patients
The Neckwise evaluation begins with a comprehensive consultation, objective testing using leg balance and infrared thermography, and CBCT 3D imaging if the screens point toward upper cervical involvement. The CBCT produces a true three-dimensional model of the atlas and axis, quantifying any misalignment in degrees and millimeters across all axes of motion.
The correction itself involves no twisting of the neck, no cracking or popping sound, and no forceful pulling. This is particularly important for patients with lupus, who often have heightened tissue sensitivity, possible joint involvement, and an autonomic nervous system that is already in a state of heightened reactivity. The correction is delivered as a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place but to give the body a precise mechanical input that allows it to release the misalignment on its own terms.
Upper cervical care is not a cure for lupus, and it is not a substitute for rheumatology care, hydroxychloroquine, biologics, or any other component of the conventional treatment plan. It is a structural intervention designed to support a specific, documented piece of the disease picture: the autonomic regulation of the immune response.
Finding Natural Support for Lupus in Sarasota
If you are living with lupus and searching for natural support in Sarasota, an upper cervical evaluation may be a meaningful piece of your overall care. The connection between vagal tone, autonomic dysfunction, and lupus disease activity is well-documented in peer-reviewed research, and the structural conditions at the head-neck junction directly influence the nerve at the center of that connection.
To learn more or schedule a consultation, contact Neckwise
Sarasota. Lupus is multifactorial, and recovery is rarely the result of any single intervention. What upper cervical care offers is a structured, evidence-based way to address one of the upstream factors that may be limiting the body's ability to regulate its own immune response.



Leave a comment