

"Three of the most common headache types have distinct diagnostic features but share a critical anatomical convergence in the trigeminocervical complex. Understanding how each one differs — and how craniocervical structural problems can affect all three through the brainstem neuroanatomy that connects them — clarifies why upper cervical evaluation may matter regardless of which headache type you have"
Headaches are one of the most common medical complaints, but the term 'headache' covers conditions with very different underlying mechanisms, presentations, and appropriate treatments. Migraine, tension-type headache, and cervicogenic headache are three of the most common chronic headache patterns, and they are frequently confused with one another. Many patients who have been told they have 'just tension headaches' actually have migraine. Many patients diagnosed with migraine have substantial cervicogenic contribution that has never been identified. Many patients with cervicogenic headache have been treated for years as primary migraine without ever having the cervical source of their pain addressed. Accurate identification matters because the treatments differ substantially across types, and chronic headache patients managed for the wrong condition often have years of inadequate results before the actual diagnosis is established. This article will discuss the connection between upper cervical spine misalignment and how it can be at the root cause of many types of headaches.
Schedule Your Appointment
Schedule appointmentWhat makes diagnostic clarity particularly challenging is that these three conditions share a critical anatomical structure in the brainstem — the trigeminocervical complex. This region, where sensory input from the trigeminal nerve and the upper cervical nerves converges, is fundamental to all three headache types but operates differently in each. The 2003 paper by Bartsch and Goadsby in Current Pain and Headache Reports established the trigeminocervical complex as the anatomical link explaining how cervical structures interact with headache mechanisms across multiple headache types (Bartsch & Goadsby, 2003). For migraine, the trigeminocervical complex is part of the migraine activation pathway. For tension-type headache, it processes the input from the cervical musculature that contributes to the pain pattern. For cervicogenic headache, it is the central pathway through which cervical structural problems produce head pain that gets perceived as headache.
This article walks through how to distinguish migraine, tension-type headache, and cervicogenic headache by their specific features, the underlying neuroanatomy that each one involves, the shared anatomical convergence in the trigeminocervical complex that affects all three, and why craniocervical structural problems can contribute to all three conditions through the brainstem neurology that connects them — though to different degrees and through different specific mechanisms. The article emphasizes the neurology because the neurology is what determines how cervical structural problems can affect each headache type, which clarifies why upper cervical evaluation may matter for headache patients regardless of which specific type they have.
To schedule an evaluation, call 941-259-1891.
Listen to one of our patient's headache recovery story in our office. Click here to watch.
The Three Headache Types: Diagnostic Features That Distinguish Them
Each headache type has specific diagnostic features that distinguish it from the others. The International Classification of Headache Disorders (ICHD-3) provides the framework for these distinctions, and clinical features generally allow accurate identification when carefully evaluated.
Migraine: features and presentation
Migraine is a primary headache disorder with specific characteristic features. The pain is typically unilateral (one-sided), throbbing or pulsating in quality, moderate to severe in intensity, and worsened by routine physical activity. Episodes typically last 4 to 72 hours when untreated. Migraine attacks are characteristically accompanied by associated features that distinguish them from other headache types: nausea or vomiting, photophobia (sensitivity to light), and phonophobia (sensitivity to sound). Some patients experience aura — typically visual phenomena like zigzag lines, blind spots, or shimmering — that precedes or accompanies the headache. Many patients have prodromal symptoms (fatigue, mood changes, food cravings) hours to days before attacks. The pattern is episodic for most patients, with discrete attacks separated by symptom-free periods, though chronic migraine (more than 15 headache days per month) develops in some patients.
Tension-type headache: features and presentation
Tension-type headache (TTH) typically presents differently from migraine. The pain is most often bilateral (both sides), pressing or tightening in quality (often described as a band around the head), mild to moderate in intensity, and NOT worsened by routine physical activity. Episodes can last 30 minutes to several days. Tension-type headaches typically do NOT have the prominent associated features that characterize migraine — significant nausea is uncommon, and patients may have mild photophobia or phonophobia but not both. Many patients have prominent neck or shoulder muscle tension associated with attacks. The pattern can be episodic (infrequent or frequent) or chronic (more than 15 days per month). The 2000 review by Bendtsen in Cephalalgia documented the pathophysiology framework for tension-type headache (Bendtsen, 2000).
To schedule an evaluation, call 941-259-1891.
Cervicogenic headache: features and presentation
Cervicogenic headache is distinct from both migraine and tension-type. The pain originates from structures in the cervical spine and typically presents with specific features. The pain is usually unilateral and side-locked (does not switch sides between attacks). It often begins at the base of the skull or in the neck and spreads forward and upward into the head, reaching the forehead, temple, or behind the eye on the affected side. The pain quality is typically deep, dull, or pressing rather than throbbing. Episodes can last hours to days, and many patients have chronic continuous pain with periodic exacerbations rather than discrete attacks. Cervical features are characteristic — neck pain accompanying the headache, restricted cervical range of motion, pain triggered or worsened by specific neck movements or sustained positions, tender points in the suboccipital region, and pain reproduced by pressure on cervical structures. The 2009 paper by Bogduk and Govind in The Lancet Neurology provided the comprehensive clinical review (Bogduk & Govind, 2009), and the 1998 criteria developed by Sjaastad and colleagues provide additional clinical features useful for diagnosis (Sjaastad et al., 1998).
Where confusion happens
Confusion between these conditions happens for several reasons. The conditions can have overlapping features — a unilateral throbbing headache could be migraine or could be cervicogenic. The conditions can coexist in the same patient — many patients have both migraine and tension-type, or both migraine and cervicogenic. The features may evolve over time within an individual patient, with chronic patterns developing characteristics that mix elements of multiple types. And the diagnostic systems themselves require careful application — patients may not have all the features needed for clean diagnosis, leading to default labeling that may not capture the actual mechanism. Despite these complications, careful clinical evaluation generally allows accurate identification of which type predominates in a given patient.
The Trigeminocervical Complex: The Anatomical Convergence That Connects All Three
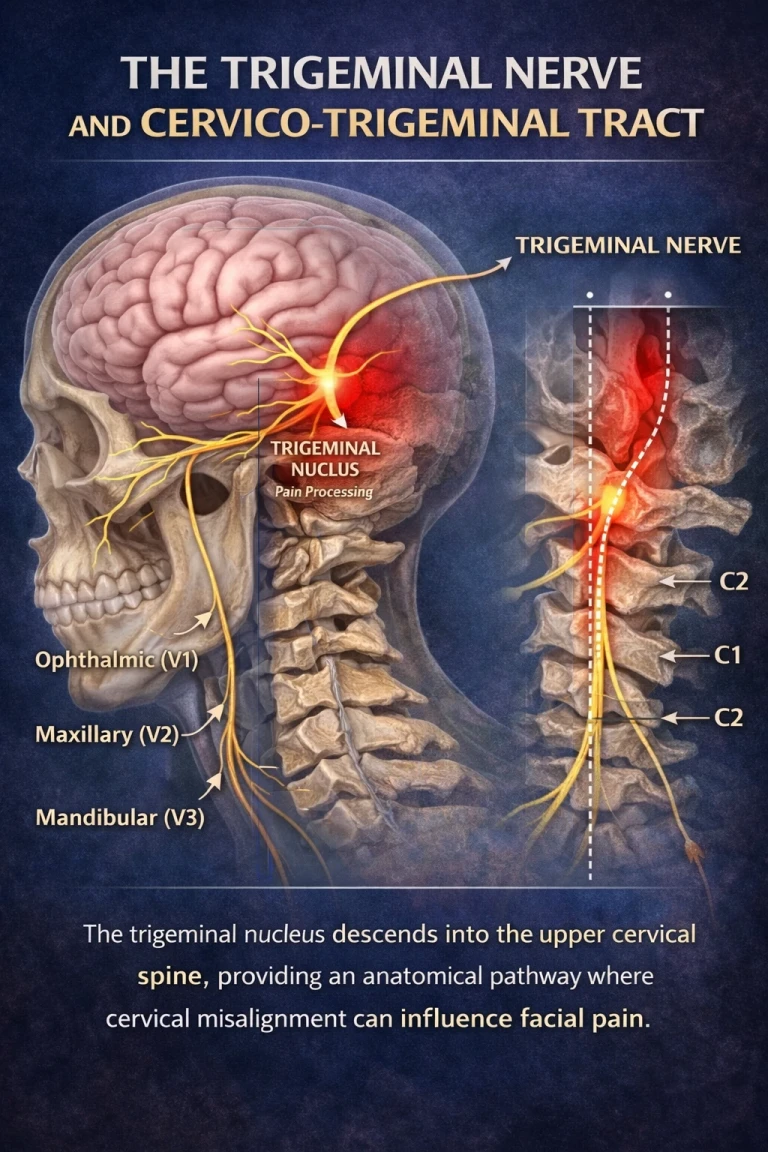
Understanding why craniocervical structural problems can affect all three headache types requires understanding the trigeminocervical complex — the brainstem region where sensory input from the trigeminal nerve and upper cervical nerves converges. This anatomical structure is fundamental to all three headache types and provides the mechanism by which cervical structural problems contribute to each.

What the trigeminocervical complex actually is
The trigeminocervical complex refers to a region in the lower brainstem and upper cervical spinal cord where neurons receive convergent input from two sensory systems. The trigeminal nerve provides sensation to the face, scalp, the dura mater covering the brain, and most other structures in the head. The upper cervical nerves (C1, C2, and C3) provide sensation to the back of the head, the upper neck, and structures in the upper cervical region. These two systems converge in the trigeminocervical complex such that single neurons receive input from both trigeminal and cervical sources. The 2003 paper by Bartsch and Goadsby in Current Pain and Headache Reports established this convergence as the anatomical foundation for understanding how cervical structures can affect headache mechanisms (Bartsch & Goadsby, 2003).
The functional consequence of convergence
The functional consequence of this convergence is that the brain cannot perfectly distinguish whether a signal in these convergent neurons came from trigeminal sources or cervical sources. Input from cervical structures can be interpreted as pain coming from trigeminal-innervated areas of the head — a phenomenon called referred pain. Conversely, activation of the trigeminal system can sensitize the cervical input pathways. The convergence creates bidirectional influence between the cervical and trigeminal systems, with implications for all headache types that involve trigeminal mechanisms.
Why this matters for migraine
Migraine is fundamentally a trigeminal disorder — the trigeminovascular system that produces migraine attacks operates through the trigeminal nerve and its central connections. When cervical input converges on the same neurons that process migraine-related trigeminal signals, cervical structural problems can affect migraine activation. The cervical input does not cause primary migraine, but it can lower the threshold for migraine activation, contribute to attack triggers, and worsen the central sensitization that develops in chronic migraine. This is why migraine patients with cervical structural problems often have more frequent or severe attacks than they would with optimal cervical function.
Why this matters for tension-type headache
Tension-type headache involves pericranial muscle tenderness and central sensitization of pain processing. The cervical muscular and structural component is substantial — many tension-type headache patients have prominent suboccipital muscle involvement, and the myodural bridge mechanism (discussed below) provides a direct mechanical pathway from cervical muscle tension to dural sensitivity. The trigeminocervical complex processes the cervical input that contributes to tension-type pain patterns. The 2011 review by Bendtsen and Fernández-de-las-Peñas in Current Pain and Headache Reports discussed the cervical contribution to tension-type headache (Bendtsen & Fernández-de-las-Peñas, 2011). For many tension-type patients, the cervical component is not just associated finding but central mechanism.
Why this matters for cervicogenic headache
Cervicogenic headache, by definition, originates from cervical structures. The trigeminocervical complex is the direct mechanism — pain from cervical structures (joints, muscles, ligaments) reaches the trigeminocervical complex through C1-C3 afferents, then is referred to head regions through the trigeminal projections. The patient feels headache, but the actual pain generator is in the cervical region. Of the three headache types, cervicogenic headache has the most direct dependence on the trigeminocervical complex for its pain mechanism.
To schedule an evaluation, call 941-259-1891.
The Craniocervical Anatomy That Affects All Three Headache Types
Several specific anatomical structures in the upper cervical region contribute to the trigeminocervical complex input that affects all three headache types. Understanding these structures clarifies how craniocervical structural problems can affect headache mechanisms across different headache types.
The atlanto-occipital and atlanto-axial joints
The joints between the skull and atlas (atlanto-occipital) and between the atlas and axis (atlanto-axial) contain dense populations of mechanoreceptors. The 1994 paper by McLain in Spine documented dense mechanoreceptor innervation in cervical facet joints, with particularly rich receptor populations in the upper cervical levels (McLain, 1994). These receptors report joint position and movement to the brainstem, providing the integration centers with detailed information about head position and motion. When upper cervical structural problems are present — misalignment between the skull, atlas, and axis from trauma, postural problems, or other causes — the receptors report signals reflecting abnormal joint positions. The brainstem receives accurate information about an abnormal state, and this distorted input feeds into the trigeminocervical complex and broader brainstem processing.
The suboccipital muscles
The four suboccipital muscles — rectus capitis posterior major and minor, obliquus capitis superior and inferior — connect the skull to the atlas and axis. These muscles are not ordinary muscles. The 2001 study by Kulkarni and colleagues in Neurology India quantified muscle spindle density in the suboccipital muscles and found substantially higher density than in most other muscles in the body (Kulkarni et al., 2001). Muscle spindles report muscle length and rate of length change. The exceptional density of receptors in this small region means the suboccipital muscles generate disproportionately rich proprioceptive output. When these muscles are chronically tense from compensating for craniocervical structural problems, the proprioceptive signal becomes distorted. The brainstem receives signals about head position that don't match what other sensory channels report, contributing to the kind of sensory mismatch that affects the broader processing including the trigeminocervical complex.
The myodural bridge
The 1995 paper by Hack and colleagues in Spine documented direct connective tissue continuity between the rectus capitis posterior minor muscle and the spinal dura mater — the myodural bridge (Hack et al., 1995). This bridge provides a direct mechanical pathway from suboccipital muscle tension to the dura. The dura is one of the most pain-sensitive structures in the head, with extensive trigeminal innervation. When suboccipital muscles are chronically tense, mechanical force transmits through the myodural bridge to the dura, contributing to dural sensitivity. This mechanism is particularly relevant for tension-type headache and cervicogenic headache, though it can also contribute to the dural sensitivity component of chronic migraine.
The C2-C3 facet joint and third occipital nerve
The C2-C3 facet joint and its innervation by the third occipital nerve is one of the most documented anatomical sources of cervicogenic headache. The third occipital nerve emerges from the medial branch of the C3 dorsal ramus and innervates both the C2-C3 facet joint and a region of the suboccipital area. Pain from this joint can be referred to the occipital, parietal, and frontotemporal regions through trigeminocervical complex convergence. Diagnostic blocks of the third occipital nerve can confirm cervicogenic origin when they relieve the typical pain pattern.
To schedule an evaluation, call 941-259-1891.
Related article
Trigeminal Neuralgia: The Anatomy of the “Suicide Disease” Sarasota Trigeminal Neuralgia Relief
Apr 10, 2026The cumulative effect of craniocervical structural problems
When craniocervical structural problems are present, the cumulative effect of these multiple mechanisms is substantial. Distorted joint mechanoreceptor input from C0-C1 and C1-C2 joints feeds into brainstem processing through the trigeminocervical complex. Distorted muscle spindle output from chronically tense suboccipital muscles adds to the distorted input. The myodural bridge transmits mechanical force from tense suboccipital muscles directly to the dura, contributing to dural sensitivity. The C2-C3 facet joint may produce direct cervicogenic pain referred through the trigeminocervical complex. The combined effect can contribute to all three headache types through the shared brainstem anatomy that connects them.
How Craniocervical Structural Problems Affect Each Headache Type Differently
While craniocervical structural problems can affect all three headache types through the trigeminocervical complex, the specific role differs across types. Understanding these differences clarifies what role cervical evaluation may play for each condition.
For cervicogenic headache: direct causal role
For cervicogenic headache, craniocervical structural problems are typically the direct cause. The cervical structural problems produce the pain that is then referred to head regions through the trigeminocervical complex. Without the cervical structural source, the cervicogenic headache pattern would not exist. Addressing the cervical structural problems addresses the actual source of the pain. This is the strongest case for cervical evaluation across the three headache types — the cervical role is not contributory but causal.
To schedule an evaluation, call 941-259-1891.
For tension-type headache: substantial mechanistic role
For tension-type headache, craniocervical structural problems often have a substantial mechanistic role even when not the sole cause. The chronic compensatory suboccipital tension that develops with craniocervical misalignment is part of the pericranial muscle tension that characterizes tension-type headache. The myodural bridge transmits this tension to the dura, contributing to the dural sensitivity component. The distorted proprioceptive input contributes to central sensitization of pain processing. For many tension-type headache patients, addressing the cervical structural component addresses the major mechanism producing their pain. The cervical role is contributory but often substantial.
For migraine: threshold and trigger contribution
For migraine, craniocervical structural problems typically contribute to threshold and triggering rather than being the primary cause. The cervical input through the trigeminocervical complex can lower the threshold for migraine activation, contribute to specific attack triggers, and worsen the central sensitization in chronic migraine. The patient still has primary migraine biology (cortical hyperexcitability, trigeminovascular system involvement), but the cervical contribution may be making the migraine more frequent or severe than it would be with optimal cervical function. Addressing the cervical component may raise the threshold and reduce attack frequency without curing the underlying migraine biology.
Why this gradient matters
Recognizing this gradient — direct causal role in cervicogenic, substantial mechanistic role in tension-type, threshold contribution in migraine — clarifies what to expect from cervical evaluation across the three headache types. Cervicogenic headache patients may have substantial direct response to cervical correction when it's appropriate. Tension-type patients may have meaningful improvement as the cervical mechanism is addressed. Migraine patients may have reduction in attack frequency or severity as cervical contribution to threshold improves, but the underlying migraine biology continues. Setting appropriate expectations for each headache type protects patients from inflated or deflated expectations.
To schedule an evaluation, call 941-259-1891.
Pattern Recognition: How to Tell Which Type You Have
While accurate diagnosis requires clinical evaluation, several pattern features can help patients identify which headache type predominates in their situation.
Features pointing to migraine
Migraine features include throbbing or pulsating pain quality, moderate to severe intensity, unilateral pain location (though it can be bilateral), pain worsening with physical activity, presence of nausea or vomiting, sensitivity to both light AND sound during attacks, presence of aura (visual phenomena, sensory changes, speech disturbances) in some patients, prodromal symptoms hours to days before attacks, attack duration 4-72 hours when untreated, distinct attacks with symptom-free periods between, family history of migraine, and onset typically in adolescence or young adulthood. Multiple migraine features pointing in the same direction make migraine more likely.
Features pointing to tension-type headache
Tension-type features include bilateral pain location, pressing or tightening pain quality (band-like sensation), mild to moderate intensity, lack of worsening with physical activity, absence of nausea (mild only), mild photophobia OR phonophobia but not both, prominent neck or shoulder muscle tension associated with episodes, pain that often develops during or after periods of stress or sustained postures, and attack duration 30 minutes to several days.
To schedule an evaluation, call 941-259-1891.
Features pointing to cervicogenic headache
Cervicogenic features include unilateral side-locked pain (always the same side), pain beginning at the base of the skull or in the neck and spreading forward, deep dull or pressing pain quality, neck pain accompanying the headache, restricted cervical range of motion, pain triggered or worsened by specific neck movements or sustained positions, tender points in the suboccipital region, ipsilateral arm or shoulder discomfort, and onset after head or neck trauma. The cervical features distinguish cervicogenic headache from the other types.
Related article
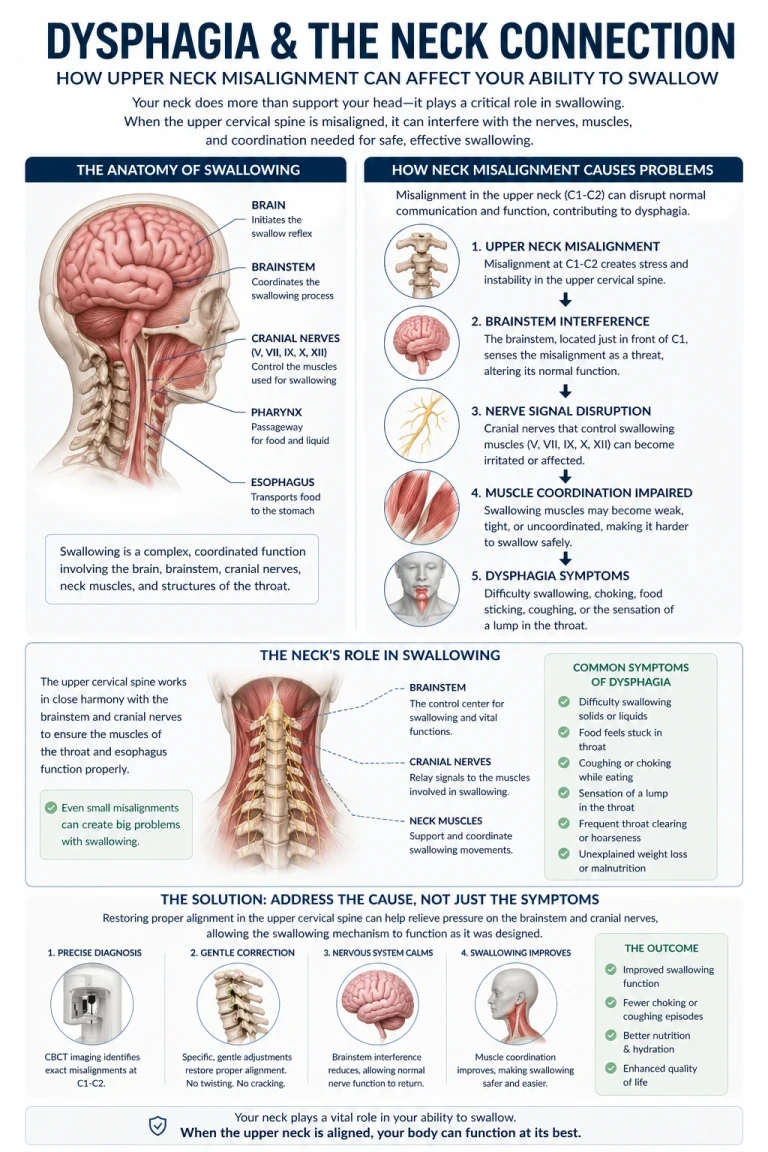
Why am I having difficulty swallowing ? | Dysphagia relief and treatment Sarasota
Apr 24, 2026When features overlap
Many patients have features pointing to more than one headache type. This may indicate true coexisting conditions (both migraine and tension-type, or both migraine and cervicogenic). It may indicate one condition with atypical features. It may indicate evolution from one pattern to another over time. Patients with mixed features benefit from comprehensive clinical evaluation rather than self-diagnosis, and comprehensive treatment that addresses the multiple components is often appropriate.
To schedule an evaluation, call 941-259-1891.
When to Consider Upper Cervical Evaluation Regardless of Headache Type
Given that craniocervical structural problems can contribute to all three headache types — direct causal role in cervicogenic, substantial mechanistic role in tension-type, threshold contribution in migraine — upper cervical evaluation may be worth considering across headache types when specific features suggest cervical involvement.
Features suggesting cervical involvement may include: pain beginning at the base of the skull or upper neck regardless of where it spreads; persistent cervical symptoms (chronic neck pain, suboccipital tension, restricted range of motion) alongside the headaches; onset or worsening after head or neck trauma; pain triggered or worsened by sustained postures or specific neck movements; tender points in the suboccipital region; treatment-resistant patterns despite adequate trials of headache-specific medical management; prior concussions, whiplash, or significant neck trauma in your history; multiple coexisting symptoms suggesting craniocervical involvement (headaches plus dizziness, plus ear pressure, plus jaw symptoms).
Sarasota Upper Cervical provides three-dimensional CBCT imaging and objective testing to evaluate whether craniocervical structural factors are present that may be contributing to your headache pattern. The evaluation identifies the structural picture and determines whether correction may be appropriate. Precision-based corrections, when indicated by objective findings, address the structural component as one part of comprehensive headache care.
To schedule an evaluation, call 941-259-1891.
Upper cervical chiropractic uses precision-based low-force corrections rather than aggressive manipulation, but patients should ensure any provider they see uses appropriate gentle techniques.
Where to Go From Here
Migraine, tension-type headache, and cervicogenic headache are three distinct headache types with different specific features, different mechanisms, and different appropriate treatments. Migraine involves primary trigeminal pathology with throbbing pain and characteristic associated features. Tension-type headache involves pericranial muscle tension and central sensitization with band-like pressing pain. Cervicogenic headache originates from cervical structures with unilateral pain spreading from neck to head and prominent cervical features. Accurate identification of which type predominates in a given patient directs appropriate treatment and avoids the years of inadequate results that often follow misdiagnosis.
Despite their differences, all three headache types share an anatomical convergence in the trigeminocervical complex — the brainstem region where trigeminal and upper cervical input combines. Craniocervical structural problems can affect all three through this convergence, though to different degrees. Cervicogenic headache has direct causal dependence on cervical structures. Tension-type headache has substantial mechanistic involvement through the suboccipital muscle and myodural bridge pathways. Migraine has threshold and trigger contribution through cervical input on the trigeminal system. Recognizing this gradient clarifies that upper cervical evaluation may be relevant across headache types, with the role and expected response varying by type.
For patients whose headaches have not responded adequately to type-specific medical management, whose headaches have cervical features regardless of primary diagnosis, or whose presentations suggest multiple coexisting headache types with cervical involvement, comprehensive evaluation including craniocervical structural assessment may be relevant. At Sarasota Upper Cervical, we focus specifically on the precise structural relationship between the skull, atlas, and axis — the region most directly relevant to the trigeminocervical complex and the cervical mechanisms affecting all three headache types. Our approach uses three-dimensional CBCT imaging and objective testing to identify whether structural problems are present, with precision-based corrections when indicated as part of comprehensive headache care.
To schedule an evaluation at Sarasota Upper Cervical, call 941-259-1891.
References
Headache Classification Committee of the International Headache Society (IHS). (2018). The International Classification of Headache Disorders, 3rd edition. Cephalalgia, 38(1), 1–211.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Bogduk, N., & Govind, J. (2009). Cervicogenic headache: An assessment of the evidence on clinical diagnosis, invasive tests, and treatment. The Lancet Neurology, 8(10), 959–968.
Sjaastad, O., Fredriksen, T. A., & Pfaffenrath, V. (1998). Cervicogenic headache: Diagnostic criteria. The Cervicogenic Headache International Study Group. Headache, 38(6), 442–445.
Goadsby, P. J., Holland, P. R., Martins-Oliveira, M., Hoffmann, J., Schankin, C., & Akerman, S. (2017). Pathophysiology of migraine: A disorder of sensory processing. Physiological Reviews, 97(2), 553–622.
Bendtsen, L. (2000). Central sensitization in tension-type headache—possible pathophysiological mechanisms. Cephalalgia, 20(5), 486–508.
Bendtsen, L., & Fernández-de-las-Peñas, C. (2011). The role of muscles in tension-type headache. Current Pain and Headache Reports, 15(6), 451–458.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Treleaven, J., Jull, G., & Sterling, M. (2003). Dizziness and unsteadiness following whiplash injury: Characteristic features and relationship with cervical joint position error. Journal of Rehabilitation Medicine, 35(1), 36–43.
Bogduk, N. (2001). Cervicogenic headache: Anatomic basis and pathophysiologic mechanisms. Current Pain and Headache Reports, 5(4), 382–386.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with persistent or significant headaches should pursue appropriate medical evaluation to establish accurate diagnosis and rule out serious underlying causes. Standard evidence-based headache treatments should form the foundation of care. Upper cervical evaluation should be considered as a complementary approach for appropriate patient subsets rather than a primary treatment for headache disorders. Patients with sudden severe headache, new headache patterns, headaches with neurological symptoms, or other red flag features should seek urgent medical evaluation. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment