
Trigeminal neuralgia (TN) is often referred to as the “suicide disease” because of the intensity and unpredictability of the pain it produces. Patients describe it as electric, stabbing, or shock like,often triggered by simple activities like talking, chewing, brushing teeth, or even a light breeze across the face. For many, it becomes debilitating.
While traditional medical approaches often focus on medications or surgical decompression, there is a critical anatomical and neurological component that is frequently overlooked—one that involves not just the trigeminal nerve itself, but its deep connection to the upper cervical spine through what is known as the cervico-trigeminal tract.
Schedule Your Appointment
Schedule appointmentUnderstanding this relationship can be a game-changer for those seeking answers and long-term relief.
Click here to listen to one of our pateints recovery story from trigeminal neuralgia.
Book a FREE consult by clicking here.
What Is the Trigeminal Nerve?
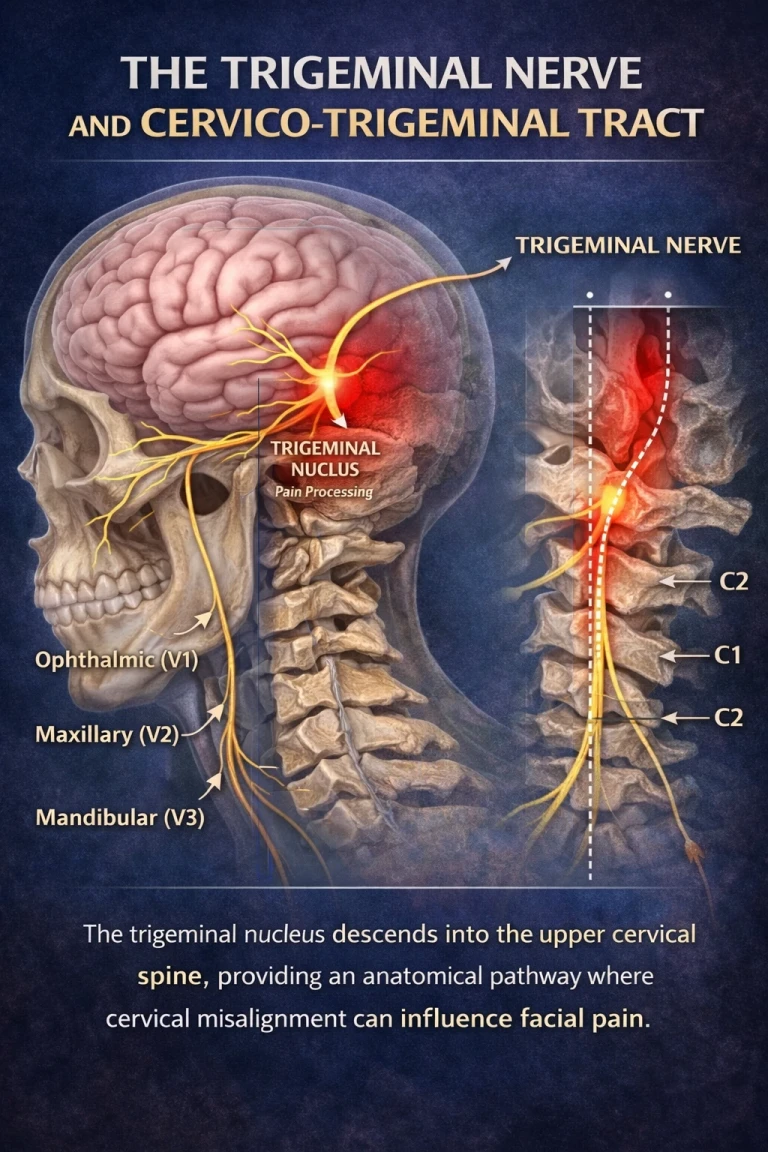
The trigeminal nerve (cranial nerve V) is the largest cranial nerve and is responsible for sensation in the face and motor functions such as chewing. It has three primary branches:
Ophthalmic (V1) – forehead, eyes
Maxillary (V2) – cheeks, upper jaw
Mandibular (V3) – lower jaw, muscles of mastication
In trigeminal neuralgia, one or more of these branches becomes irritated or hypersensitive, leading to severe pain episodes.
But the key question is: why does this irritation occur?
The Trigeminal Nucleus: More Than Just the Brain
Most people think of the trigeminal nerve as existing only in the face and brain. However, its processing center—the trigeminal nucleus—is far more extensive than commonly understood.
The trigeminal nucleus begins in the brainstem but extends downward into the upper cervical spinal cord—reaching as low as the third cervical vertebra (C3). This descending pathway is known as the spinal trigeminal tract, or more clinically relevant in this context, the cervico-trigeminal tract.
This anatomical connection is critical.
It means that sensory information from the face and input from the upper cervical spine converge and interact within the same neurological pathways.
The Cervico-Trigeminal Connection: Where the Neck Meets the Face
The cervico-trigeminal tract creates a bridge between:
The trigeminal nerve (face sensation)
The upper cervical nerves (C1, C2, C3)
Because of this overlap, dysfunction in the upper cervical spine can directly influence how the brain processes facial pain.
How Does This Lead to Trigeminal Neuralgia?
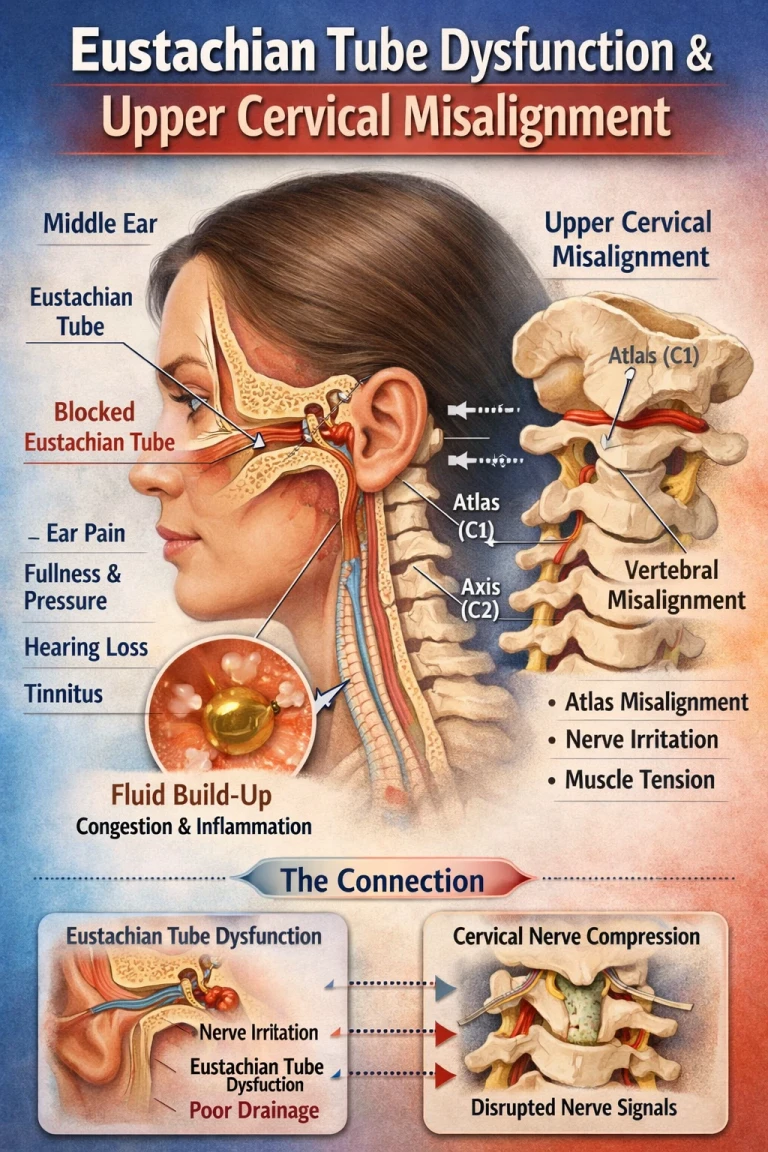
When there is misalignment or dysfunction in the upper cervical spine—particularly at the atlas (C1) and axis (C2)—it can lead to:
Related article

Tinnitus Relief: Understanding the Upper Cervical Connection to Ear Ringing
Jan 26, 2026Abnormal afferent input from cervical joints
Irritation of the spinal trigeminal nucleus
Sensitization of trigeminal pathways
Cross-talk between cervical and facial pain signals
This phenomenon is known as convergence—where multiple sources of input feed into the same neural pathway.
As a result, a problem in the neck can manifest as pain in the face.
Book a FREE consult by clicking here.
Upper Cervical Misalignment: A Hidden Contributor
The atlas (C1) and axis (C2) sit directly beneath the skull and surround the brainstem. This region is the most neurologically dense and mechanically vulnerable part of the spine.
When misalignment occurs—whether from trauma, poor posture, or repetitive stress—it can create a cascade of effects:
1. Altered Joint Mechanics
Misaligned joints change how the spine moves and how forces are distributed.
2. Distorted Proprioceptive Input
The upper cervical spine contains a high concentration of mechanoreceptors. When these joints are off, the brain receives faulty information.
3. Irritation of Neural Pathways
Because of the proximity to the brainstem and cervico-trigeminal tract, even subtle misalignments can affect nerve signaling.
4. Central Sensitization
Over time, the nervous system can become hypersensitive, amplifying pain signals—even in the absence of ongoing injury.
Why Many Treatments Fall Short
Traditional approaches to trigeminal neuralgia often include:
Anticonvulsant medications (like carbamazepine)
Nerve blocks
Microvascular decompression surgery
While these may provide relief for some, they often focus on managing symptoms rather than addressing underlying neurological interference.
If the root cause involves abnormal input from the upper cervical spine, these approaches may miss a key piece of the puzzle.
A Different Approach: Evaluating the Upper Cervical Spine

Upper cervical chiropractic care focuses on identifying and correcting structural misalignments that may be interfering with the nervous system—particularly in the brainstem and cervico-trigeminal pathways.
1. Functional Leg Balance Assessment
This assessment evaluates how the nervous system is regulating postural tone.
Subtle differences in leg length when lying down can reflect:
Neurological imbalance
Altered muscle tone
Brain-body communication issues
Changes in leg balance before and after a correction can provide immediate feedback on neurological improvement.
2. Infrared Thermography
Thermography measures heat patterns along the spine, which are regulated by the autonomic nervous system.
Consistent asymmetries in temperature can indicate:
Nervous system dysfunction
Areas of irritation or imbalance
When a patient is out of alignment
This allows for objective, non-invasive monitoring of progress.
The Role of 3D CBCT Imaging: Precision Matters
One of the most advanced tools used in upper cervical care is Cone Beam Computed Tomography (CBCT).
CBCT provides a three-dimensional view of the atlas and axis, allowing for:
Exact measurement of misalignment
Visualization in all three planes (rotation, tilt, translation)
Individualized analysis for each patient
No two people misalign the same way. This level of detail ensures that care is specific, targeted, and reproducible.
Book a FREE consult by clicking here.
Precision Corrections—Without Twisting or Popping
A major concern for many patients—especially those with trigeminal neuralgia—is the fear of forceful neck manipulation.
Upper cervical care is fundamentally different.
Corrections are:
Gentle and precise
Based on CBCT measurements
Delivered with minimal force
No twisting, popping, or pulling of the neck
The goal is not to repeatedly adjust the spine, but to make a precise correction and allow the body to stabilize.
When alignment is restored, it can reduce abnormal input into the cervico-trigeminal tract—allowing the nervous system to calm down and function more normally.
Connecting the Dots: Why the Neck Matters in Facial Pain
The key takeaway is this:
The trigeminal system does not operate in isolation.
Because the trigeminal nucleus extends into the upper cervical spine, dysfunction in this region can directly influence facial pain pathways.
This means that for many patients:
The source of trigeminal neuralgia may not be solely in the face
The neck—specifically the upper cervical spine—may be a contributing factor
Addressing structural misalignment can reduce neurological irritation
Who Should Consider This Approach?
You may want to explore an upper cervical evaluation if you:
Have been diagnosed with trigeminal neuralgia
Have not found lasting relief with medication
Have a history of neck injury, whiplash, or concussion
Experience neck stiffness along with facial pain
Notice symptoms triggered by head or neck movement
Sarasota Trigeminal Neuralgia Relief: A Hopeful Perspective
For patients in Sarasota suffering from trigeminal neuralgia, understanding the connection between the upper cervical spine and the trigeminal system offers a new perspective—one focused on root cause, not just symptom control.
By combining:
Objective testing (leg balance, thermography)
Advanced imaging (CBCT)
Precise, gentle corrections
Upper cervical care aims to restore proper neurological function and reduce interference within the cervico-trigeminal tract.
Final Thoughts
Trigeminal neuralgia is one of the most painful conditions known—but it is not without hope.
By looking beyond the face and into the deeper neurological connections between the brainstem and upper cervical spine, we uncover a powerful insight:
Structure influences function.
When the atlas and axis are properly aligned, the nervous system has the opportunity to regulate itself more effectively—potentially reducing the intensity and frequency of trigeminal neuralgia symptoms.
If you or someone you love is struggling with TN, it may be time to ask a different question:
Is the problem only in the nerve—or could it be influenced by the structure surrounding it?



Leave a comment