

The Complete Guide to How C1-C2 Affects Balance, Dizziness, and Brainstem Function
Table of Contents:
Schedule Your Appointment
Schedule appointment
1.The Problem Most Patients Are Stuck In
2.The Anatomy You Should Know
3.How Your Balance System Actually Works
4.Why C1-C2 Carries So Much Weight in Balance
5.Joint Afferentation and the Vestibular Nucleus
6.The Pressure Balance Problem: CSF, Venous Drainage, and the Brainstem
7.The Vestibular Disorders Under This Umbrella
8.How Our Practice Identifies the Structural Cause
9.CBCT Imaging: Three-Dimensional Precision
10.Objective Testing: When We Adjust and When We Do Not
11.What Healing Looks Like After Correction
12.When You Should Schedule an Evaluation
13.Frequently Asked Questions
The Problem Most Patients Are Stuck In
By the time most patients walk through our doors in Sarasota, they have been dealing with dizziness, vertigo, or balance problems for months or years. They have seen their primary care physician. They have been referred to ENT. They have had vestibular function testing, audiograms, MRIs of the brain, and sometimes cardiology evaluations. They have tried medications — meclizine, beta blockers, benzodiazepines, migraine prophylactics. They have been told, in various combinations, that they have BPPV, vestibular migraine, Meniere's disease, vestibular neuritis, anxiety, or simply that nothing is wrong.
And they are still dizzy.
There is a reason this happens so often. The body's balance system is not a single organ. It is a network — and one of the most critical nodes in that network sits at the very top of the spine, where the skull meets the first two vertebrae. The atlas (C1) and the axis (C2) form a structural and neurological relationship with the brainstem that influences vestibular function more powerfully than almost any other part of the body. When this relationship is misaligned, the body's entire balance system can produce symptoms that look like inner ear disease, look like migraine, look like a dozen other diagnoses — but originate in the neck.
This guide explains the science behind that connection. It walks through the anatomy, the research, the conditions involved, and the precise approach we use at Sarasota Upper Cervical Chiropractic to identify and correct the structural cause when it is present. If you have been dizzy for too long and the answers have not come together, this is the information you should have.
Ready to find out if your dizziness has a structural cause? Call Sarasota Upper Cervical Chiropractic at 941-259-1891 to schedule an evaluation.
The Anatomy You Should Know
Three bones define the craniocervical junction — the region where the skull meets the spine. The occiput, at the base of the skull. The atlas (C1), the first cervical vertebra, which sits directly underneath the skull and supports its full weight. The axis (C2), the second cervical vertebra, which provides the rotational pivot for the head.
What makes this region so consequential is what it contains and what passes through it.
The atlas: a ring with no body
Unlike every other vertebra in the spine, the atlas has no central body. It is essentially a ring of bone that cradles the base of the skull. It carries the full weight of the head — roughly 10 to 12 pounds — directly on top of the spine, with no intervertebral disc as a cushion. The structural integrity of this region depends entirely on the precision of bony articulation, the strength of ligaments, and the coordination of deep neck musculature.
The axis: the rotational pivot
The axis has a unique vertical bony peg called the odontoid process, or dens, that rises up into the ring of the atlas. The atlas rotates around this peg — that is what allows the head to turn left and right. Approximately half of the rotational motion of the entire cervical spine occurs at this single joint.
The corridor of critical structures
Inside the bony ring formed by the foramen magnum, the atlas, and the axis, several critical structures pass simultaneously. The spinal cord transitions into the brainstem here. The vertebral arteries pass through, supplying blood to the posterior brain — including the vestibular nuclei and the cerebellum. The cerebrospinal fluid pathways move between the cranial vault and the spinal canal through this corridor. The venous plexuses that drain blood from the skull pass through it. And the vestibular nuclei themselves — the brainstem structures that produce your sense of balance — sit just inside this region.
When the bones surrounding this corridor are precisely aligned, every structure inside operates in its natural geometry. When alignment shifts, the mechanical environment changes for everything inside.
Proprioceptive density that exceeds anywhere else in the spine
The upper cervical region contains the highest concentration of proprioceptive nerve endings found anywhere in the spinal column. The deep muscles at the base of the skull contain some of the densest networks of muscle spindles in the entire human body (Kulkarni et al., 2001). The fibrous capsules of the upper cervical joints are richly populated with mechanoreceptors (McLain, 1994). These receptors send a constant stream of information about head position and motion directly to the brainstem.
How Your Balance System Actually Works
Balance is not produced in the inner ear. The inner ear contributes to balance, but the actual sense of equilibrium is constructed inside the brainstem, in a cluster of cells called the vestibular nuclei. These nuclei receive, integrate, and weight three streams of sensory information in real time:
Visual input from the eyes — telling the brain where the horizon is and how the visual field is moving.
Vestibular input from the inner ear — the semicircular canals and otolith organs reporting acceleration of the head.
Proprioceptive input from the body, with a disproportionate contribution from the upper cervical spine — reporting the position and motion of the head relative to the body.
When these three streams agree, balance feels effortless. You do not consciously notice your balance system any more than you consciously notice your breathing. When the three streams disagree — when the eyes report one thing, the inner ear another, and the neck a third — the integration breaks down. What patients experience is the sensation of dizziness, vertigo, unsteadiness, disorientation, or visual motion sensitivity.
This is the central insight that ties upper cervical care to vestibular health. The system cannot distinguish between an accurate cervical signal and a distorted one. It can only detect whether the three streams agree. If the cervical input is wrong, the output is dizziness — even when the inner ear is perfectly healthy and every other test comes back normal.
Your balance system is a three-way integration. When the inner ear is fine and the brain is fine but you are still dizzy, the third input — the neck — is where the answer usually lies.
If your inner ear and brain have already been cleared but you are still experiencing symptoms, the cervical contribution may be what has been missed.
Call 941-259-1891 to schedule a consultation.
Why C1-C2 Carries So Much Weight in Balance
Not every part of the spine contributes equally to vestibular function. The upper cervical region carries disproportionate weight, for three reasons established in the research.
Receptor density that is biologically extraordinary
The concentration of mechanoreceptors in the upper cervical joints and the muscle spindle density in the suboccipital muscles is among the highest documented anywhere in the human body (Kulkarni et al., 2001; McLain, 1994). These receptors are not just signaling joint position. They are signaling the fine-grained, moment-to-moment data the brainstem needs to know exactly where the head is and how it is moving.
Direct neural projections into the vestibular nuclei
Upper cervical proprioceptive nerve fibers project directly into the vestibular nuclei in the brainstem. This connection has been demonstrated in neuroanatomical research. Gdowski and McCrea's 2000 study in Experimental Brain Research showed that neck proprioceptive inputs reach primate vestibular nucleus neurons through direct neuroanatomical pathways, integrating in real time with vestibular and visual signals (Gdowski & McCrea, 2000). The cervical signal is not an afterthought in vestibular processing. It is a direct sensory feed.
The apex of the postural chain
The upper cervical spine sits at the top of the body's postural chain. When alignment is altered here, the entire postural strategy of the body compensates downward — shoulders shift, hips rotate, leg length functionally changes. These compensations create additional distorted proprioceptive signals from below, all of which feed into the same vestibular integration. The further the body compensates, the more confused the brainstem becomes.
Joint Afferentation and the Vestibular Nucleus
Related article
Dystonia, Proprioception, and the Upper Cervical Spine | Dystonia relief and treatment sarasota
Jul 07, 2026The technical term for the sensory signal that travels from a joint to the brain is afferentation. In the upper cervical spine, this afferentation is the primary information stream the brainstem uses to know where the head is. When that afferentation is normal, balance works. When it is abnormal, balance fails.
The mechanism by which upper cervical misalignment produces abnormal afferentation follows a clear, sequential pathway documented in the peer-reviewed literature.
Step 1: The joint stops moving normally
A misaligned vertebra sits slightly off neutral. When the head moves, the affected joint cannot glide and rotate the way it was designed to. Some directions of motion become restricted. Others become compensatorily hypermobile. The smooth, coordinated motion of the upper cervical spine is disrupted.
Step 2: The joint capsule is mechanically stressed
The fibrous capsule surrounding the joint — which houses the mechanoreceptors — is now placed under abnormal mechanical strain. The receptors that should be firing in clean, predictable patterns during normal joint motion begin firing in distorted patterns. The deep suboccipital muscles, also affected by the misalignment, contribute their own distorted spindle signals to the mix.
Step 3: The brain receives erroneous data
A 2022 narrative review in the Journal of Clinical Medicine described this directly, noting that dysfunctional cervical joints produce "erroneous proprioceptive afferents" — sensory signals that no longer accurately reflect what the joints are actually doing (Peng et al., 2022). The information arriving at the brainstem is no longer correct.
Step 4: The vestibular nuclei cannot integrate
The erroneous afferents travel up to the vestibular nuclei alongside the accurate signals from the inner ear and visual system. The brainstem faces an integration problem. The eyes report one reality. The inner ear reports another. The neck contradicts both. The result of trying to integrate contradictory sensory streams is the experience of vertigo, unsteadiness, fogginess, or visual motion sensitivity.
Step 5: The body compensates, at a cost
Over time, the body adapts. Postural patterns shift. Muscle tone changes. The brain begins to over-rely on visual and inner ear signals to compensate for the unreliable cervical input. This adaptation costs energy — energy that should be spent on healing and routine function gets routed into compensating for the sensory mismatch. Patients describe this as fatigue, brain fog, reduced exercise tolerance, and a general sense of operating below their baseline.
The Pressure Balance Problem: CSF, Venous Drainage, and the Brainstem
Joint afferentation is only one pathway by which upper cervical misalignment affects the vestibular system. A second pathway, equally important and less well known, involves the mechanical environment of the brainstem itself — and the flow of fluid in and out of the skull.
In 2015, chiropractic neurologist Michael F. Flanagan published a peer-reviewed review article in Neurology Research International titled "The Role of the Craniocervical Junction in Craniospinal Hydrodynamics and Neurodegenerative Conditions" (Flanagan, 2015). The paper described the craniocervical junction as a potential choke point for craniospinal hydrodynamics. The argument has anatomical force behind it.
Cerebral blood flow into the brainstem
The vertebral arteries pass through small openings in the transverse foramina of the upper cervical vertebrae before joining to form the basilar artery, which supplies the brainstem — including the vestibular nuclei — and the cerebellum, the brain region responsible for balance coordination. Misalignment at the upper cervical level can alter the mechanical environment of these arteries, contributing to reduced posterior circulation flow.
Venous drainage out of the skull
The venous plexuses around the upper cervical spine are responsible for draining blood from the cranial vault. When craniocervical alignment is altered, these venous pathways can become congested. The downstream consequence is increased intracranial pressure and disrupted fluid balance — a mechanism with direct relevance to inner ear fluid disorders like Meniere's disease, where the question of what initially drives the fluid imbalance has been unanswered for decades.
Cerebrospinal fluid drainage and circulation
Cerebrospinal fluid circulates between the cranial vault and the spinal canal through the corridor at the craniocervical junction. When this corridor is geometrically compromised, CSF flow can be impeded. The downstream effects include altered pressure dynamics in the brain and inner ear, which shares fluid communication with the cerebrospinal system. This is the brain's pressure balance system, and it depends on craniocervical alignment to function as designed.
Direct mechanical irritation of the brainstem
The brainstem itself sits inside this corridor. Mechanical irritation of the brainstem and its surrounding structures, caused by craniocervical misalignment, can produce both afferent disruption (sensory signals coming up) and efferent disruption (motor and autonomic signals going down). The vestibular nuclei are inside this same anatomical environment and are subject to the same mechanical conditions.
The craniocervical junction is a potential choke point for blood and CSF flow between the cranial vault and spinal canal that can cause faulty craniospinal hydrodynamics. (Flanagan, 2015)
Understanding these mechanisms is the first step. Identifying whether they apply to your case requires a precise structural evaluation.
Call 941-259-1891 to schedule a free consultation
The Vestibular Disorders Under This Umbrella
Upper cervical misalignment does not produce a single vestibular diagnosis. It contributes — to varying degrees — to a range of conditions across the vestibular spectrum. Each condition below has been associated in the research literature with cervical or craniocervical mechanisms. For some, the cervical contribution is the primary driver. For others, it is one of several factors that, when addressed, can substantially improve outcomes.
Cervicogenic dizziness
Cervicogenic dizziness is the condition most directly tied to upper cervical dysfunction. It is defined by dizziness or imbalance caused by abnormal sensory input from the cervical spine, with the hallmark of dizziness reliably triggered by specific head or neck movements. Treleaven et al. (2003) demonstrated that patients with whiplash-associated dizziness showed significantly greater cervical joint position errors than healthy controls, with the proprioceptive dysfunction directly linked to symptoms (Treleaven et al., 2003). For these patients, structural upper cervical evaluation is the most direct path to the answer.
Vestibular migraine
Vestibular migraine is defined by episodes of moderate-to-severe vertigo lasting 5 minutes to 72 hours, with migraine features in at least half of the episodes (Lempert et al., 2022). The cervical contribution is significant but often overlooked. The upper cervical region shares neuroanatomy with the trigeminocervical complex — the brainstem area where cervical and trigeminal sensory inputs converge — making cervical irritation a recognized migraine driver. Patients with vestibular migraine who have a co-existing cervical contribution often experience reduced attack frequency and severity when the structural component is addressed alongside migraine-specific care.
Meniere's disease
Meniere's disease is characterized by episodic vertigo, fluctuating hearing loss, eustachian tube dysfunction, tinnitus, and aural fullness. The traditional mechanistic explanation focuses on endolymphatic hydrops — excess fluid in the inner ear — but the question of what drives the fluid imbalance has remained open for decades. Dr. Michael Burcon's 2016 study in the Journal of Upper Cervical Chiropractic Research reported on 300 patients with diagnosed Meniere's disease, all of whom had a documented history of prior whiplash or head trauma — on average, fifteen years before symptom onset (Burcon, 2016). Burcon's proposed mechanism aligns with Flanagan's hydrodynamic model: craniocervical misalignment compromises venous drainage and CSF flow, producing the inner ear fluid imbalance that defines Meniere's.
BPPV that does not respond to the Epley maneuver
True benign paroxysmal positional vertigo — caused by displaced otoconia in the semicircular canals — typically resolves with one or two correctly performed Epley maneuvers. Patients who continue to experience positional vertigo after multiple maneuvers very often do not have BPPV. They may have what the literature calls pseudo-BPPV, or they may have vestibular migraine, PPPD, or cervicogenic dizziness producing a positional pattern. Repeating Epley maneuvers in these patients can worsen symptoms. A structural evaluation of the upper cervical spine often reveals the underlying driver that the maneuver could not address.
Vestibular neuritis and persistent post-event dizziness
Vestibular neuritis is an acute condition involving inflammation of the vestibular nerve, usually attributed to viral infection. The acute phase is real and self-limited. However, a meaningful percentage of patients continue to experience chronic dizziness long after the inflammatory phase has resolved. Approximately 25 percent develop persistent postural-perceptual dizziness within 3 to 12 months following an acute vestibular event (Popkirov et al., 2018). Many of these chronic cases involve a cervical proprioceptive component that was not addressed during acute care.
Related article
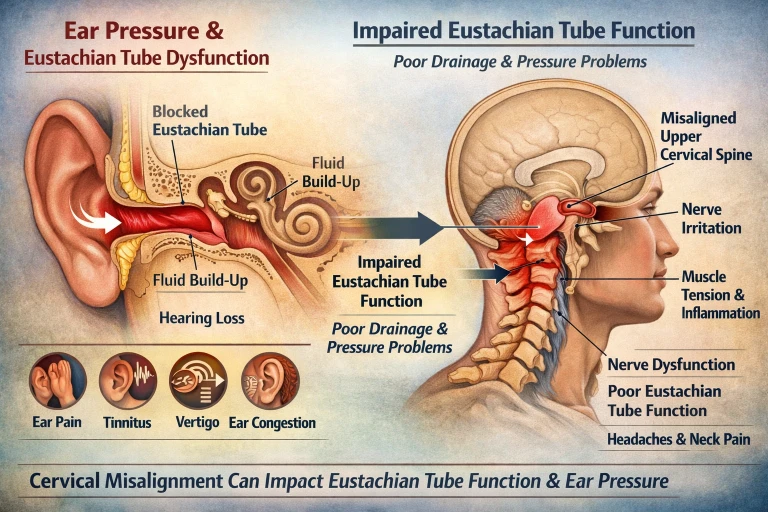
Why Won’t My Ear Pop? Eustachian Tube Dysfunction Relief in Sarasota and Bradenton
Mar 14, 2026Persistent postural-perceptual dizziness (PPPD)
PPPD is a chronic functional vestibular disorder characterized by non-spinning dizziness and unsteadiness lasting three months or longer. The Barany Society formalized diagnostic criteria for PPPD in 2017. The condition involves a failure of normal sensory reweighting after an initial event — the brain continues to over-rely on visual and somatosensory input, including cervical input. When the cervical input is itself distorted by upper cervical misalignment, the central reweighting process cannot complete. Addressing the structural input often allows the central pathways to recalibrate.
Mal de Debarquement Syndrome (MdDS)
MdDS produces a persistent sensation of rocking or swaying, typically triggered by extended passive motion such as a cruise or long flight. The condition involves chronic sensory mismatch with strong central involvement. Patients with MdDS frequently report a history of head or neck trauma preceding the motion exposure, and a cervical proprioceptive contribution is plausible and worth evaluating in any patient with persistent symptoms.
Cervicogenic headache with associated dizziness
Cervicogenic headache, defined by pain referred from the cervical spine, frequently co-exists with dizziness. A 2024 study in The Journal of Turkish Spinal Surgery demonstrated that patients with cervicogenic headache had measurably worse cervical joint position error and postural control than healthy controls, with proprioceptive abnormalities specifically driving the dizziness component (Vural et al., 2024). When headache and dizziness occur together with neck involvement, the cervical spine is implicated in both.
Post-traumatic vertigo from whiplash and head injury
Post-traumatic vertigo is one of the clearest examples of upper cervical misalignment as a direct cause of vestibular dysfunction. Whiplash injuries place the upper cervical spine under extreme mechanical load, frequently producing joint capsule injuries, ligamentous laxity, and persistent C1-C2 misalignment. The mechanism connecting the injury to the dizziness is the same proprioceptive distortion described earlier. For these patients, upper cervical evaluation is not optional — it is the most likely path to identifying the underlying structural driver.
Tinnitus and aural fullness
Tinnitus is not classified as a vestibular disorder, but it frequently co-occurs with vestibular complaints and often shares the same underlying mechanism — particularly when tinnitus is unilateral and accompanies a documented craniocervical misalignment on the same side. Tinnitus has been observed to resolve or substantially improve in patients receiving upper cervical correction when the structural component is addressed.
How Our Practice Identifies the Structural Cause
At Sarasota Upper Cervical Chiropractic, we use a structured assessment process to determine whether the upper cervical spine is contributing to a patient's vestibular symptoms. This process has three layers: a comprehensive history, a focused physical examination, and precise objective measurement.
The history conversation
Most of what we need to know surfaces in the first conversation. We ask about the character of the dizziness — spinning, floating, lightheaded, off-balance. We ask about triggers — what makes it worse, what makes it better, whether specific head positions reliably reproduce the symptom. We ask about the timeline — when it began, what was happening in your life at the time, what other symptoms came with it. And we ask carefully about injury history, including events that may not have seemed connected at the time. A whiplash from college. A fall off a bicycle in childhood. A sports concussion. A difficult birth. These often turn out to be the precipitating event for symptoms that developed years later.
The examination
A focused physical examination assesses cervical range of motion, the mobility of the upper cervical segments, the tone and tenderness of the suboccipital musculature, and any reproducible relationship between specific cervical positions and the dizziness symptoms. Findings consistent with upper cervical involvement include reduced upper cervical range of motion, palpable joint restriction, suboccipital tension, and provocation of symptoms with specific cervical maneuvers.
The structural measurement
Where upper cervical chiropractic differs most clearly from general chiropractic and from medical imaging is in the precision of the structural measurement we use. The next two sections explain that in detail.
CBCT Imaging: Three-Dimensional Precision
Cone beam computed tomography, or CBCT, is a low-dose three-dimensional imaging technology originally developed for dental and maxillofacial applications and now used in upper cervical practice for the same reason it was adopted in dentistry: it produces a true 3D reconstruction of complex anatomy in a region where two-dimensional imaging is unreliable.
The upper cervical region is geometrically complex. Misalignments can occur in multiple planes simultaneously — rotation, lateral tilt, anterior-posterior translation. Standard two-dimensional X-rays of this region are subject to projectional distortion and cannot reliably capture this three-dimensional information. Small but mechanically significant misalignments are simply not visible on conventional imaging.
CBCT eliminates that limitation. From a CBCT scan, we can measure the precise angle and direction of misalignment between the occiput, atlas, and axis to within fractions of a degree. Every patient's anatomy is unique. The exact correction that one patient needs is different from what another patient needs, and CBCT is what allows us to calculate the specific correction each individual requires.
Importantly, in upper cervical practice CBCT is used as a measurement tool, not a diagnostic tool. We are not looking for pathology — fractures, tumors, herniated discs. Those would be evaluated by other imaging if clinically indicated. CBCT in our office is what allows us to map the patient's structural anatomy with the precision needed to deliver a calculated, specific correction.
Objective Testing: When We Adjust and When We Do Not
This is one of the most important principles in upper cervical chiropractic, and it is one of the principles that distinguishes our approach most clearly from routine chiropractic care. We do not adjust on a schedule. We adjust only when objective testing indicates the upper cervical spine has shifted out of its corrected position.
Two assessments are performed at every visit.
Leg length analysis
Leg length analysis is a postural test in which the patient is examined for asymmetry in functional leg length. Upper cervical misalignment produces measurable functional leg length inequality through the compensatory postural changes it triggers below the neck. When the upper cervical correction is holding, leg length normalizes. When the correction has shifted, leg length asymmetry returns. The test takes seconds and provides an objective check before any decision to adjust is made.
Paraspinal infrared thermography
Paraspinal infrared thermography is a non-invasive scan that measures heat patterns along the cervical spine. Asymmetric autonomic nervous system activity, driven by upper cervical irritation, produces measurable temperature differentials along the neck. A consistent thermal pattern indicates the spine is out of alignment. A neutral pattern indicates the correction is holding.
The decision the testing makes
If both tests indicate the upper cervical spine is in alignment, we do not adjust. The body is doing the work. If the tests indicate the spine has shifted, we deliver a precise correction along the vector calculated from the CBCT analysis. This is the opposite of routine, schedule-based adjusting. The principle is restraint guided by data. We adjust when adjusting is warranted, and we leave the body alone when it is not.
For patients with chronic vestibular symptoms — whose nervous systems are often already sensitized by years of symptoms — this matters significantly. Unnecessary manipulation aggravates a sensitive system. The precision-and-restraint approach respects the sensitivity of the nervous system you bring to the office.
We do not adjust because it is Tuesday. We adjust because the measurements indicate an adjustment is needed. If they do not, we do not. The body is doing the work, and our job is to support that — not to interfere with it.
If you want a structural evaluation that uses 3D imaging and objective testing rather than guesswork, Sarasota Upper Cervical Chiropractic is the place to start.
Call 941-259-1891 to schedule a FREE consultation
What Healing Looks Like After Correction
Upper cervical correction does not heal the body. It removes the structural obstacle that has been preventing the body from healing itself. Once the correction is established and the joint is in its proper position, a sequence of changes begins.
The joint capsule is no longer held in an abnormal position. The mechanical strain on surrounding ligaments and muscles is reduced. Local inflammation decreases. Blood flow and lymphatic drainage improve as the mechanical environment normalizes. The mechanoreceptors in the joint capsules begin to fire in a more accurate, less chaotic pattern. As the proprioceptive input cleans up, the input to the vestibular nuclei cleans up with it. The brainstem integration problem resolves gradually.
Related article

Upper Cervical Chiropractor Sarasota, Bradenton, Venice and Tampa Bay Area
Nov 15, 2021Patients typically describe the improvement as gradual rather than instantaneous. The intensity of vestibular episodes tends to decrease first. The frequency drops next. The provocative head positions that used to reliably trigger symptoms stop producing them. Confidence with movement returns. Over a longer time frame — typically several months — the surrounding soft tissues continue to remodel. Ligaments tighten where they had become lax. Joint capsules heal more completely. Muscle patterns reorganize away from the protective guarding the body had been doing.
Care at our practice generally proceeds in two phases. The first is a corrective phase, during which the alignment is established and the body is given time to stabilize in the corrected position. Visit frequency is higher early on and tapers as the correction begins to hold. The second is a maintenance phase, during which we monitor the alignment at longer intervals and adjust only when objective testing indicates a shift. Most patients eventually settle into monthly or less-frequent maintenance, similar in concept to a periodic dental cleaning — a check-up, a measurement, a correction if needed.
When You Should Schedule an Evaluation
An upper cervical evaluation is worth scheduling when any of the following are true:
You have chronic dizziness, vertigo, or imbalance that has not been adequately explained by other workups. You have a history of whiplash, concussion, sports injury, or other neck trauma — even years or decades ago. Your dizziness is reliably triggered by specific head or neck movements. You have been diagnosed with a vestibular condition but have not had lasting relief from standard treatment. You have persistent neck pain or stiffness alongside the dizziness. You experience associated symptoms like brain fog, fatigue, suboccipital headache, or visual disturbance that point collectively toward a cervical contribution. You have completed extensive medical testing and been told nothing is wrong despite ongoing symptoms.
None of these alone is diagnostic. Several of them together are a strong signal that the upper cervical spine deserves to be evaluated as part of your workup. For most patients, that evaluation has not yet been done with the precision needed to identify the structural component.
Sarasota Upper Cervical Chiropractic serves patients from across the Sarasota and Bradenton areas. To schedule your free evaluation, call 941-259-1891.
Frequently Asked Questions
How is upper cervical chiropractic different from regular chiropractic?
Upper cervical chiropractic focuses exclusively on the precise structural relationship between the skull, atlas (C1), and axis (C2). We use 3D CBCT imaging to measure misalignment with high precision, objective testing before every adjustment to determine whether correction is needed, and specific low-force corrections delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The principle is precision over volume — fewer, better-targeted adjustments rather than more frequent, generalized ones.
Is upper cervical correction safe for patients with chronic dizziness?
The low-force, precision nature of upper cervical correction makes it particularly well suited for patients with sensitized nervous systems, which is common in chronic vestibular conditions. Because we only adjust when objective testing indicates a misalignment is present, patients are not subjected to unnecessary manipulation. The corrections themselves are small and specific.
How long does it take to see results?
Improvement is typically gradual rather than instantaneous. Some patients notice early changes within the first few weeks. Others require longer as the soft tissues heal and proprioceptive signaling normalizes. Outcomes vary by individual, by the severity and chronicity of the underlying injury, and by overall health factors. We discuss realistic expectations with every patient based on their specific case.
Do I need to stop my other medical treatments?
No. Upper cervical care is complementary to, not a replacement for, other medical care. For patients with vestibular migraine, Meniere's disease, or other diagnosed conditions, continuing appropriate medical management alongside structural care is the typical approach. Many patients find their best symptom control comes from addressing both the structural and the medical aspects of their condition.
What if I have not had any neck trauma I remember?
The precipitating event is often distant in time and not consciously connected to current symptoms. Many patients cannot recall the original event, particularly when it occurred in childhood, in sports, or in minor accidents that did not require medical attention. The absence of a remembered trauma does not rule out an upper cervical contribution. A structural evaluation can identify misalignment regardless of whether you can recall how it began.
How do I schedule an evaluation?
Call our office at 941-259-1891. We will schedule a consultation that includes a thorough history, focused examination, and if appropriate, CBCT imaging and objective baseline testing.
Take the Next Step
Chronic dizziness deserves a thorough evaluation that includes a precise structural assessment of the upper cervical spine. For most patients, this assessment has not yet been part of their workup. It often becomes the step that opens the answer they have been searching for.
Sarasota Upper Cervical Chiropractic serves patients throughout the Sarasota and Bradenton areas.
To schedule your FREE evaluation, call 941-259-1891.
References
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions.
Neurology Research International, 2015, Article 794829.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses.
Neurology India, 49(4), 355–359.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Gdowski, G. T., & McCrea, R. A. (2000). Neck proprioceptive inputs to primate vestibular nucleus neurons. Experimental Brain Research, 135(4), 511–526.
Peng, B., Yang, L., Yang, C., Pang, X., Chen, X., & Wu, Y. (2022). Proprioceptive cervicogenic dizziness: A narrative review of pathogenesis, diagnosis, and treatment. Journal of Clinical Medicine, 11(21), 6293.
Treleaven, J., Jull, G., & Sterling, M. (2003). Dizziness and unsteadiness following whiplash injury: Characteristic features and relationship with cervical joint position error. Journal of Rehabilitation Medicine, 35(1), 36–43.
Burcon, M. T. (2016). Health outcomes following cervical specific protocol in 300 patients with Meniere's followed over six years. Journal of Upper Cervical Chiropractic Research, June 2, 2016.
Popkirov, S., Staab, J. P., & Stone, J. (2018). Persistent postural-perceptual dizziness (PPPD): A common, characteristic and treatable cause of chronic dizziness. Practical Neurology, 18(1), 5–13.
Lempert, T., Olesen, J., Furman, J., et al. (2022). Vestibular migraine: Diagnostic criteria (Update). Journal of Vestibular Research, 32(1), 1–6.
Vural, M., Karan, A., Albayrak Gezer, İ., et al. (2024). Cervical proprioception and vestibular functions in patients with neck pain and cervicogenic headache: A comparative study. The Journal of Turkish Spinal Surgery.
Reiley, A. S., Vickory, F. M., Funderburg, S. E., Cesario, R. A., & Clendaniel, R. A. (2017). How to diagnose cervicogenic dizziness. Archives of Physiotherapy, 7, 12.\
Yacovino, D. A., & Hain, T. C. (2009). Clinical characteristics of cervicogenic-related dizziness and vertigo. Seminars in Neurology, 33(3), 244–255.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with chronic dizziness or vestibular symptoms should pursue appropriate medical evaluation alongside any structural assessment. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment