
Facial pain is one of the hardest things in medicine to diagnose correctly, and trigeminal neuralgia is one of the most commonly misidentified conditions within it. People spend months, sometimes years, being treated for the wrong problem: a TMJ disorder, a dental issue, a sinus infection, or a headache disorder, when the real culprit is a different condition entirely. That delay matters, because the treatments are completely different. This guide lays out how trigeminal neuralgia is distinguished from the conditions it's most often confused with, and where the upper cervical spine fits into the picture.
A boundary first: these are medical diagnoses that require evaluation by qualified providers, and the distinctions here are educational, not a substitute for a proper workup. Upper cervical chiropractic does not diagnose or cure trigeminal neuralgia. What it focuses on is a possible cervical contributor to facial-pain sensitivity, addressed alongside medical care.
Schedule Your Appointment
Schedule appointmentWhat trigeminal neuralgia actually is
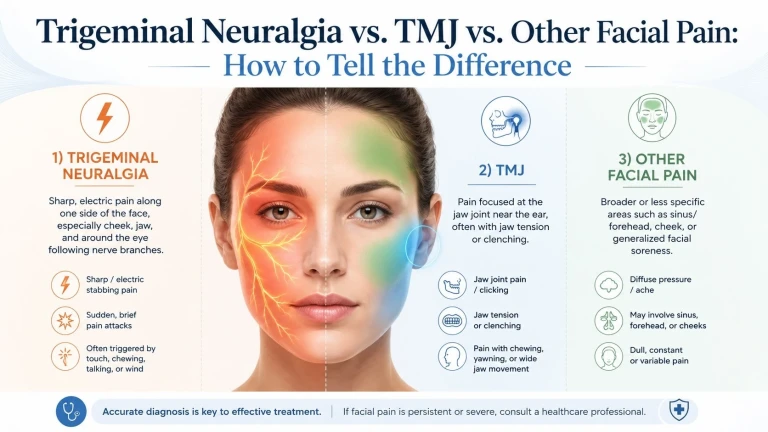
Trigeminal neuralgia (TN) is a disorder of the trigeminal nerve — the fifth cranial nerve, which carries sensation from the face. Its signature is unmistakable once you know it: sudden, severe, electric-shock-like pain in short bursts, usually on one side of the face, in the cheek, jaw, or around the lips. Classically, patients present with 10/10 facial pain triggered by teeth brushing, shaving, talking, or chewing, within the distribution of the maxillary (V2) or mandibular (V3) branches. Most cases are caused by a blood vessel compressing the nerve near the brainstem, which is why the physical exam is typically normal and diagnosis rests on the pattern of the pain.
That "electric, brief, triggered by light touch" signature is the anchor for telling TN apart from everything else. Here's how the main mimics differ.
A few distinctions are worth spelling out, because they're the ones that most often get missed:
TN vs. TMJ. This is the most common mix-up. TMJ disorders produce persistent, more constant pain related to jaw movement, often with localized tenderness and jaw abnormalities, unlike TN, where the pain is short and stabbing. If your pain is a dull ache that worsens when you chew and comes with jaw clicking or tenderness, that points toward TMJ. If it's a brief electric jolt set off by a light touch to the face, that points toward TN. (Importantly, the two can also coexist, more on that below.)
Related article

Why Is My Face Drooping on One Side? | Natural Bell’s Palsy Treatment and Relief in Sarasota
Apr 26, 2026TN vs. cluster/TAC headaches. Both are one-sided and severe, but cluster headaches linger and occur behind the eye, whereas TN feels more like a shocking, electric pain that comes in short bursts. The dead giveaway for a trigeminal autonomic cephalalgia is prominent autonomic symptoms on the same side, tearing, a red eye, a runny or congested nostril. TN generally doesn't come with those.
TN vs. post-herpetic neuralgia. Post-herpetic neuralgia is a complication of shingles causing constant, burning pain, unlike the episodic nature of trigeminal neuralgia. The distinguishing clue is history: a prior shingles rash in the painful area, most often on the forehead or around the eye.
The quick filter: Brief electric shocks triggered by light touch → think TN. Dull ache worse with chewing, plus jaw clicking → think TMJ. One-sided pain behind the eye with tearing and a stuffy nostril → think cluster/TAC. Constant burning where a shingles rash used to be → think post-herpetic neuralgia. These overlap and can coexist, so this narrows the field rather than settling it — a clinical diagnosis is essential.
How TN is diagnosed
Because TN is defined by its clinical features, the diagnosis rests on the history and pain pattern, with the physical exam typically normal. Imaging plays a specific role: MRI is recommended to rule out secondary causes like multiple sclerosis, tumors, or neurovascular compression, and is particularly useful for visualizing the trigeminal nerve and adjacent structures. Examining the ears, mouth, teeth, and jaw joint helps identify the mimics, dental pain and TMJ disorders in particular. This is why an accurate diagnosis usually involves a physician or neurologist, not self-diagnosis.
Where the upper cervical spine fits in the facial-pain picture
Here's the connection that's relevant to all of this, and it's specific neuroanatomy, not a vague claim. The trigeminal nerve (the face) and the upper cervical nerve roots (the neck) don't stay separate in the brainstem. They converge on the same pool of neurons, an integrated structure often called the trigeminocervical complex. The upper cervical segments, especially C2 and C3, are a primary source of input into the spinal trigeminal nucleus, and cervical and trigeminal signals become functionally intertwined there.
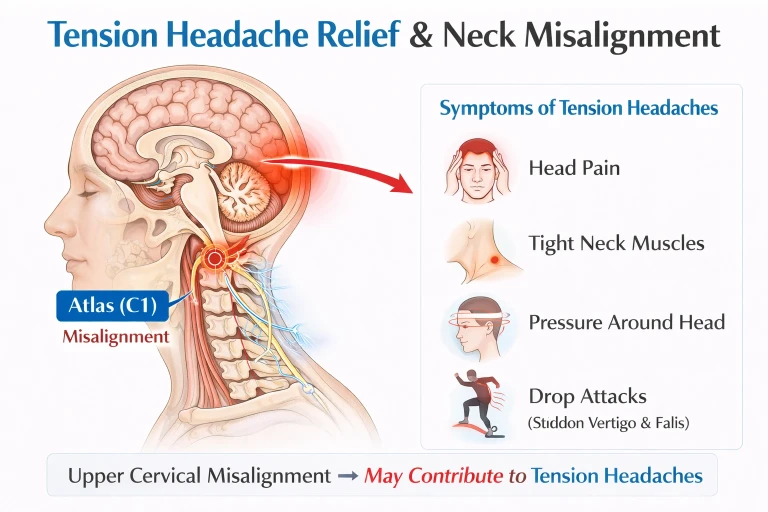
The practical implication: input from the upper neck can influence how the trigeminal system processes and amplifies pain. This doesn't mean a neck misalignment causes classic trigeminal neuralgia, classic TN is driven by neurovascular compression of the nerve, and that's a medical/neurosurgical matter. But it does mean the upper cervical spine is a plausible contributor to facial-pain sensitivity and to the overall load on the trigeminal system, and that a dysfunctional craniocervical junction can add aberrant input into a circuit that's already irritated. For some patients — particularly those with a neck component to their symptoms, a history of head or neck trauma, or overlapping TMJ and neck dysfunction, that contributor is worth evaluating.
Upper cervical care focuses on restoring normal alignment and input at the atlas and axis to reduce that aberrant cervical input into the trigeminocervical complex — as a complement to medical care, not as a treatment for the underlying nerve compression of classic TN. It works best as one coordinated part of a plan led by your physician or neurologist.
Where medical treatment leads — and why the right diagnosis matters
The reason the differential matters so much is that the treatments don't overlap. Trigeminal neuralgia responds to specific anticonvulsant medications (carbamazepine is the long-established first-line drug) and, in appropriate cases, to neurosurgical procedures like microvascular decompression — treatments that do nothing for TMJ, cluster headache, or post-herpetic neuralgia, and vice versa. Being treated for the wrong condition is the single biggest source of delay in getting facial pain under control. That's the whole reason to sort out which condition you actually have, early, with a qualified provider — and it's why an accurate diagnosis, not a guess, is the first step.
Questions and Answers
How do I know if my facial pain is trigeminal neuralgia or TMJ?
The pain pattern usually tells them apart. Trigeminal neuralgia is brief, electric-shock-like pain triggered by light touch — brushing teeth, shaving, a breeze, talking. TMJ disorder is a more constant, dull ache or pressure that worsens with chewing or jaw clenching, often with jaw clicking or tenderness. If it's a lightning jolt from a gentle touch, think TN; if it's an ache that worsens when you use your jaw, think TMJ. They can also coexist, so a clinical evaluation is needed to be sure.
What's the difference between trigeminal neuralgia and a cluster headache?
Both are severe and one-sided, but the pattern differs. Cluster (and related TAC) headaches linger — minutes to hours — and center around or behind the eye, usually with autonomic symptoms on the same side like tearing, redness, and nasal congestion. Trigeminal neuralgia is a brief, shock-like pain in short bursts across the cheek or jaw, generally without those eye and nose symptoms. The autonomic features are the biggest clue toward a cluster/TAC headache.
Could my facial pain be from shingles?
It's possible if you've had a shingles rash. Post-herpetic neuralgia is a complication of shingles that causes constant, burning pain in the area where the rash occurred — commonly the forehead or around the eye when the trigeminal nerve is involved — unlike the brief, episodic shocks of trigeminal neuralgia. A history of a shingles outbreak in the painful area is the distinguishing clue, and a new rash near the eye needs prompt medical care.
Can a neck problem cause trigeminal neuralgia?
Classic trigeminal neuralgia is caused by a blood vessel compressing the nerve, not by the neck — so a neck misalignment doesn't cause it. But the trigeminal nerve and the upper cervical nerve roots (C1–C3) converge on the same brainstem neurons, the trigeminocervical complex, so upper cervical input can influence how the trigeminal system processes pain. That makes the upper neck a plausible contributor to facial-pain sensitivity worth evaluating — especially with a neck component or trauma history — alongside medical care, not as a cause or cure of classic TN.
Why does getting the right diagnosis matter so much?
Because the treatments are completely different and don't cross over. Trigeminal neuralgia responds to specific anticonvulsant medications and, in some cases, neurosurgery — treatments that do nothing for TMJ, cluster headache, or post-herpetic neuralgia. Being treated for the wrong condition is the biggest source of delay in getting facial pain controlled, which is why an accurate diagnosis from a qualified provider is the essential first step.
When should I see a doctor urgently?
Seek prompt care for jaw or temple pain with scalp tenderness and any vision change (possible giant cell arteritis, which can threaten sight), a new shingles rash near the eye or forehead, facial pain with numbness, weakness, or other neurological changes, or a sudden worst-ever headache. These can signal serious conditions that need medical evaluation right away, not conservative care.
Facial pain evaluation in Sarasota — the upper cervical connection
If you have facial pain that hasn't been clearly diagnosed, or trigeminal neuralgia with a neck component or trauma history — a focused upper cervical evaluation can help determine whether a cervical contributor is part of your picture, working alongside your medical care.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Trigeminal neuralgia, TMJ disorders, cluster and other headache disorders, and post-herpetic neuralgia are medical conditions that must be diagnosed and managed by qualified medical providers; classic trigeminal neuralgia is typically caused by neurovascular compression and is managed with medication and, in some cases, neurosurgery. Upper cervical chiropractic does not diagnose or cure trigeminal neuralgia and is not a substitute for medical care; it focuses on possible cervical contributors to facial-pain sensitivity via the trigeminocervical complex, as a complement to appropriate medical management. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization or superiority is made or implied. Cone beam CT is used as a precision measurement and analysis tool, not as a diagnostic device for facial pain. The mechanisms described are presented for education, not as proof of causation or treatment outcomes; individual results vary, and no specific outcome is guaranteed. Seek prompt medical attention for vision changes with jaw/temple pain, a shingles rash near the eye, facial pain with neurological changes, or a sudden severe headache. Always consult a qualified healthcare provider regarding diagnosis and treatment of facial pain.



Leave a comment