
You stepped off the cruise ship four days ago. Or you got home from that long flight last week. Or maybe it was a road trip months back. Whatever the trigger, your feet have been on solid ground for what feels like forever — and yet your body still feels like it is moving.
You feel like you are rocking. Swaying. Bobbing. Your floor seems to undulate beneath you. You lie down to sleep and the bed feels like it is gently rolling like a ship's cabin. You try to focus on your phone and the words shift. You walk through the grocery store and feel as if the floor is moving under your feet. The strange part is that when you actually get back in a car or on a boat, the sensation goes away — only to come back the moment you stop moving.
Schedule Your Appointment
Schedule appointmentIf this describes you, you are likely dealing with Mal de Débarquement Syndrome, commonly known as MdDS. It is a real condition. It is severely under-recognized. And there is a part of the underlying mechanism that very few specialists ever address: the structural relationship between your upper neck and the part of your brainstem that controls balance.
At Sarasota Upper Cervical Chiropractic, we focus on that exact relationship. This article explains what MdDS is, how the upper cervical spine and the vestibular nuclei communicate, why a misalignment at the top of the neck can perpetuate the sensation of motion long after the original trigger is gone, and what a precise, gentle structural correction may offer for patients searching for relief.
What MdDS Actually Is
MdDS is a central vestibular disorder. The name is French for "sickness of disembarkment," and it traditionally refers to the persistent sensation of motion that some people experience after stepping off a boat, plane, train, or car. Sailors have described "sea legs" for centuries — the brief feeling of still being on a rolling deck after returning to dry land. For most people, that feeling fades within hours. For some, it does not.
When the sensation persists for more than a month, it is classified as MdDS. The condition can last weeks, months, or in some cases years.
The primary symptom is a constant, low-frequency sensation of rocking, swaying, bobbing, or feeling pulled in a specific direction. Most patients describe it as feeling like they are on a boat, even when they are standing still on solid ground. Importantly, the sensation often briefly disappears when the person is back in passive motion — driving a car, riding in a boat, walking quickly — and then returns when they stop.
Associated symptoms can include:
- Imbalance and unsteadiness
- Brain fog and difficulty concentrating
- Visual motion sensitivity (busy patterns, scrolling screens, and crowds become overwhelming)
- Headaches and migraines
- Fatigue
- Anxiety and depression
- Sensitivity to fluorescent lights and sound
- Difficulty sleeping
- A feeling of "gravity pulling" in one direction
MdDS overwhelmingly affects women — roughly 85 to 90 percent of diagnosed patients are female — and onset typically occurs between the ages of 40 and 50. The condition is widely under-recognized; on average, MdDS patients see around 19 different physicians before receiving a correct diagnosis. Many are told it is anxiety, an inner ear problem, or "just stress."
The Vestibular Nuclei: Where Balance Lives
To understand why the upper neck matters in MdDS, you have to understand where balance is actually processed in the brain.

Your sense of balance does not live in your inner ear alone. It lives in a cluster of four cell bodies in the brainstem called the vestibular nuclei. These nuclei sit at the base of the brainstem, just behind the cerebellum and directly above the top of the spinal cord — almost exactly at the level of the atlas, the first vertebra of your neck.
The vestibular nuclei are the central processing center for everything related to balance, head position, and spatial orientation. They receive three main streams of input:
1. **Vestibular input** from the inner ear, which detects head rotation and acceleration.
2. **Visual input** from the eyes, which provides a frame of reference for the horizon and surroundings.
3. **Proprioceptive input** from the upper cervical spine, which tells the brain where the head is positioned relative to the body.
The vestibular nuclei integrate these three streams in real time and use the result to generate a coherent sense of motion and stability. When all three streams agree, you feel balanced. When they disagree — when one stream tells the brain "you are moving" and another says "you are still" — the result is sensory mismatch, the conflict that drives dizziness, vertigo, and disorders like MdDS.
This is exactly why MdDS feels the way it does. The brain has formed an internal model that you are still on a moving boat, even though your eyes and inner ear now disagree. The vestibular nuclei are stuck in an oscillating pattern, and the conflict produces the persistent sensation of rocking.
C1, C2, C3 and the Joint Input the Brainstem Depends On
Here is the piece that conventional vestibular care often misses: a large portion of the proprioceptive input the vestibular nuclei rely on comes from the upper three vertebrae of your neck.
The joints, muscles, and ligaments of the upper cervical spine are extraordinarily rich in nerve receptors. The joint capsules of C1, C2, and C3 alone contain roughly 50 percent of all proprioceptors in the entire cervical spine. The small suboccipital muscles at the base of the skull have some of the highest densities of muscle spindles found anywhere in the human body — up to 200 spindles per gram of muscle tissue (Kulkarni et al., 2001).
This is not an accident of anatomy. The upper neck is the structural hinge between the head and the body, and the brain depends on a constant, accurate stream of information from this region to know where the head is in space at every moment. That information travels directly into the vestibular nuclei and is integrated with the inner-ear and visual signals to produce your sense of balance.
In a healthy upper cervical spine, this proprioceptive input is clean. The vestibular nuclei receive accurate information about head position, and they can resolve any conflict between the inner ear and the eyes by checking it against the cervical signal.
When the upper cervical spine is misaligned, that proprioceptive signal becomes distorted. The joint receptors of C1, C2, and C3 send altered information to the brainstem. The vestibular nuclei receive a faulty third input, and the integration breaks down. The brain is left trying to reconcile streams of information that no longer agree.
How an Upper Cervical Misalignment Can Perpetuate MdDS
This is where the connection to MdDS becomes important.

MdDS is fundamentally a problem of vestibular maladaptation. The brain adapted to the rocking motion of a boat and then failed to readapt to stillness when you got off. The vestibular nuclei and their connections in the cerebellum settled into an oscillating pattern that the brain now treats as normal.
For the brain to break out of that pattern, every input feeding the vestibular nuclei needs to be accurate and consistent. If the upper cervical spine is delivering distorted proprioceptive input — because of an underlying atlas displacement complex, often the result of an old head or neck injury, a car accident, a fall, a concussion, or a difficult birth — the vestibular nuclei never get a clean reset.
Put another way: the trigger for MdDS may have been the cruise, but the reason the symptoms have not resolved may be that one of the three sensory streams feeding your balance system is structurally compromised. The brain cannot recalibrate properly when one of its reference signals is faulty.
This is why some MdDS patients improve with traditional vestibular rehabilitation, while others plateau or relapse repeatedly. The visual and inner-ear retraining addresses two of the three input streams. The cervical stream is rarely examined or corrected — even though it carries half of the cervical proprioceptive load directly into the brainstem.
What the Research Shows
A case report by Gleberzon and Arts, published in 2012 in the *Journal of Chiropractic Medicine*, documented the use of upper cervical chiropractic care for a patient with recurrent episodes of MdDS. The patient experienced meaningful improvement in symptoms with care directed at the upper cervical spine.
The relationship between cervical proprioception and the vestibular nuclei is well established in the broader neuroscience literature. Researchers have repeatedly demonstrated that proprioceptive signals from the upper cervical spine converge on the vestibular nuclei and the cerebellum, and that disruption of cervical proprioceptive input is associated with dizziness, balance disturbance, and disorientation. The clinical entity of "cervicogenic dizziness" — dizziness driven by altered cervical sensory input — is recognized in the medical literature and is increasingly understood to overlap with several other vestibular conditions.
None of this is a randomized controlled trial in MdDS specifically, and case reports are not the same as large-scale evidence. But the anatomical pathways are real, the mechanism is biologically plausible, and the clinical experience of upper cervical chiropractors is that many MdDS patients respond meaningfully to a precise structural correction of the upper neck.
The Role of CBCT Imaging
One of the reasons upper cervical care has become more precise over the past two decades is the availability of cone beam computed tomography, or CBCT. Standard two-dimensional X-rays can show the upper cervical spine but have significant limitations when the goal is to measure the precise three-dimensional relationship between the skull, the atlas, and the axis.
CBCT changes that. It produces a high-resolution three-dimensional image of the upper cervical region, allowing the doctor to measure exactly how the atlas is positioned relative to the skull above and the axis below. Angles, rotations, and lateral shifts that would be invisible or ambiguous on a standard X-ray become measurable to a fraction of a degree.
For a region where small structural changes have outsized effects on the nervous system, this precision matters. Every spine is unique, and the angle of an atlas misalignment in one patient is different from another. Without precise imaging, the correction becomes generalized. With CBCT, the correction can be calculated specifically for that patient's anatomy, delivered with the appropriate vector, and verified with post-correction imaging to confirm that the structural change actually occurred.
For MdDS patients in particular, this precision is important. The cervical proprioceptive signal is only as accurate as the structural alignment that produces it. A correction that returns the atlas to its proper position restores accurate joint mechanics — and accurate joint mechanics produce accurate proprioceptive input to the vestibular nuclei.
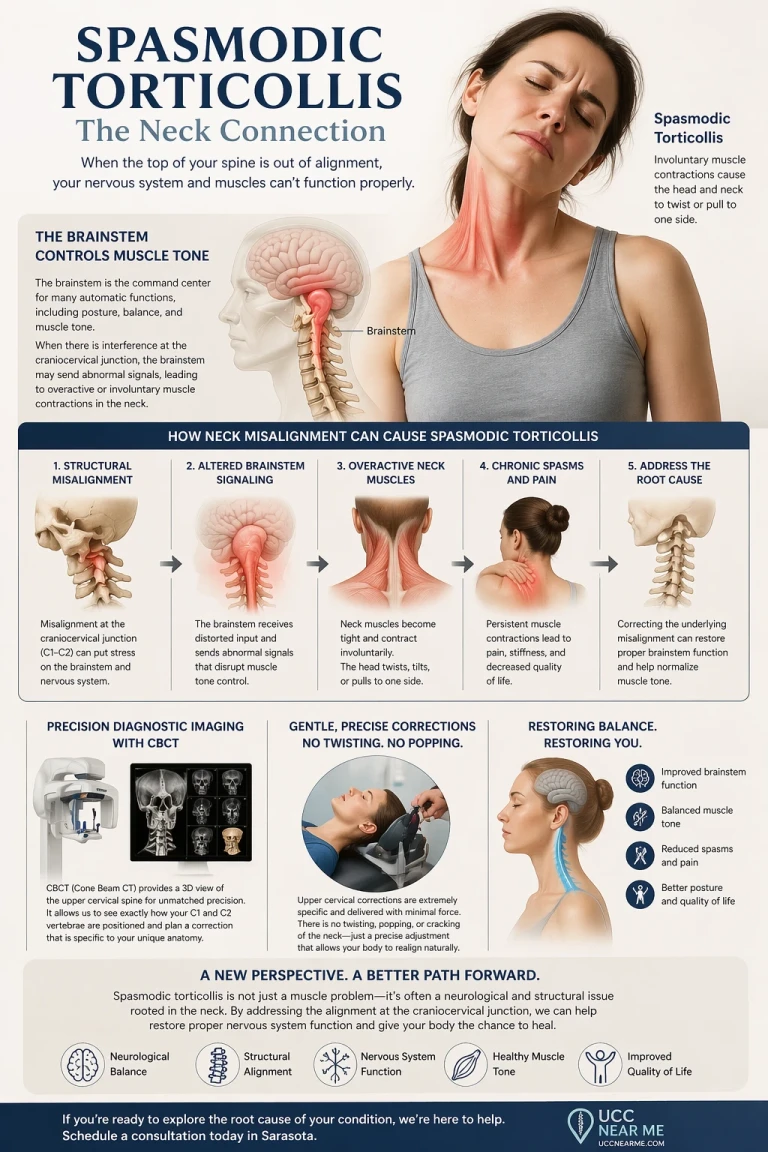
A Gentle Correction — No Popping, Twisting, or Pulling
Many MdDS patients are understandably cautious about anything involving the neck. The thought of a forceful manipulation is unsettling for someone whose nervous system already feels off balance. We want to be clear:
The upper cervical correction does not involve any popping, twisting, or pulling of the neck.
The correction is delivered with a gentle, precise, low-force impulse calculated specifically for the misalignment seen on your imaging. There is no cracking sound. There is no sudden rotation of the head. There is no manual traction. Most patients describe the correction as so light that they wonder whether anything happened at all — until they begin to notice changes in their symptoms in the hours and days afterward.
This is by design. The upper cervical region is too important and too delicate for force-based techniques. The goal is precision, not pressure.
What This Means for MdDS Patients in Sarasota
If you have been struggling with MdDS — whether for weeks, months, or years — there are several things worth considering.
First, a history of head or neck trauma may be playing a hidden role in why your symptoms have not resolved. Many MdDS patients can trace their lives back through a concussion, a car accident, a fall, or a sports injury that affected the upper cervical spine long before the cruise or flight that triggered their current symptoms. The trigger may have been the boat, but the vulnerability may have been in place for years.
Second, upper cervical chiropractic care does not claim to cure MdDS. What the underlying anatomy and the available case literature suggest is that for some MdDS patients, correcting a structural problem at the top of the neck restores accurate proprioceptive input to the vestibular nuclei — which is exactly the kind of input the brain needs to recalibrate out of the rocking pattern. Results vary from person to person.
Third, the kind of care we are describing is specific. It is not a general chiropractic adjustment. It focuses on the precise structural relationship at C1, C2, and C3, uses CBCT imaging to inform the correction, and avoids any high-force manipulation.
If you would like to learn whether your MdDS symptoms may be connected to an underlying upper cervical structural issue, the first step is a thorough evaluation including precision imaging of your craniocervical junction. From there, you and your doctor can discuss whether a structural correction is appropriate for your case.
You have spent enough time feeling like the ground is moving beneath you. There may be a part of your balance system that has never been examined — and addressing it may be the missing piece.
---
**References**
1. Kulkarni V, Chandy MJ, Babu KS. *Quantitative study of muscle spindles in suboccipital muscles of human foetuses.* Neurology India, 2001; 49(4): 355-359.
2. Gleberzon BJ, Arts J. *The use of upper cervical chiropractic management for a patient with recurrent episodes of Mal de Debarquement Syndrome.* Journal of Chiropractic Medicine, 2012; 11(4): 286-293.
3. Dai M, Cohen B, Smouha E, Cho C. *Readaptation of the vestibulo-ocular reflex relieves the Mal de Debarquement Syndrome.* Frontiers in Neurology, 2014; 5: 124.
4. Cha YH, Cui YY, Baloh RW. *Comprehensive Clinical Profile of Mal de Debarquement Syndrome.* Frontiers in Neurology, 2018; 9: 261.
5. Luxon LM. *Posttraumatic Vertigo.* In: Disorders of the Vestibular System, 1996.



Leave a comment