

If you have been diagnosed with postural orthostatic tachycardia syndrome — more commonly known as POTS — you already know how disruptive this condition can be. What used to be simple tasks like standing up from a chair, taking a shower, or walking through a grocery store can suddenly become exhausting, dizzying, and frightening. Your heart races for no clear reason. Your vision tunnels. Your legs feel weak. You may have spent months or years moving between specialists, trying medications, increasing salt and fluids, and wearing compression garments — and still feel like no one has explained why your body is doing this.
At Sarasota Upper Cervical Chiropractic, we focus on a part of POTS that conventional cardiology and neurology often overlook: the structural relationship between the upper neck and the brainstem. There is a growing body of research suggesting that a misalignment at the top of the spine — specifically at the atlas (C1) and axis (C2) — can interfere with the brainstem's ability to regulate the autonomic nervous system, and that correcting this structural problem may meaningfully improve POTS symptoms.
Schedule Your Appointment
Schedule appointmentThis article explains what POTS is, the full range of symptoms it can produce, how the upper cervical spine connects to brainstem function, what the research shows, and what a precision-based structural correction actually looks like.
What POTS Is....
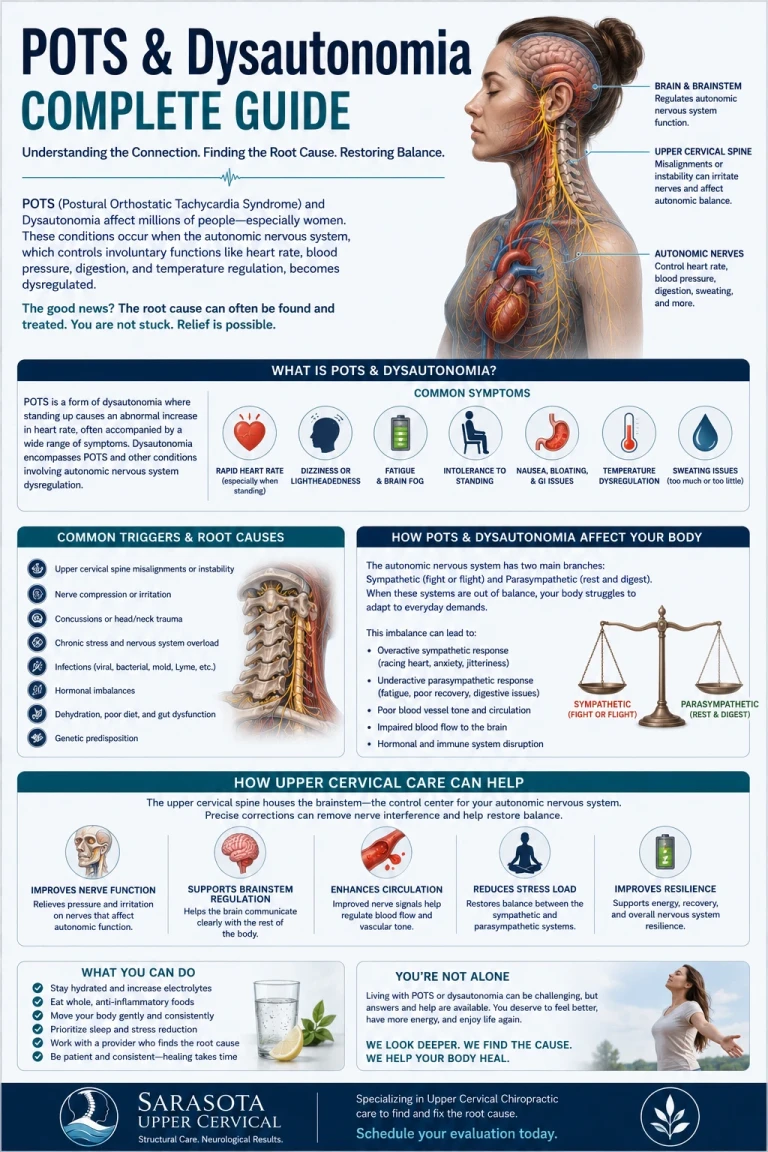
POTS is a form of dysautonomia, which means a disorder of the autonomic nervous system. The autonomic nervous system is the part of your nervous system that regulates the functions you don't consciously control — heart rate, blood pressure, digestion, sweating, body temperature, breathing rate, and pupil response, among others.
In POTS, this regulatory system fails to respond properly when you change position. The clinical definition is straightforward: a sustained heart rate increase of at least 30 beats per minute in adults (or 40 bpm in adolescents) within 10 minutes of standing, without a significant drop in blood pressure, and accompanied by symptoms of orthostatic intolerance.
But the heart rate spike is only the diagnostic marker. The lived experience of POTS extends far beyond a fast pulse.
The Full Range of POTS Symptoms
POTS produces a remarkably wide array of symptoms, and patients are often surprised to learn how many seemingly unrelated issues can be traced back to autonomic dysfunction. Common symptoms include:
- Lightheadedness and dizziness, especially when standing
- Rapid or pounding heart rate
- Heart palpitations
- Fainting or near-fainting episodes (syncope and presyncope)
- Chronic fatigue, often severe
- Brain fog and cognitive difficulty
- Difficulty concentrating
- Exercise intolerance
- Headaches and migraines
- Nausea and digestive issues
- Bloating, constipation, or diarrhea
- Blurred or tunnel vision
- Shortness of breath
- Chest discomfort
- Tremors and shakiness
- Excessive sweating, or the inability to sweat normally
- Cold hands and feet, or poor temperature regulation
- Sleep disturbances
- Anxiety-like symptoms (often mistaken for an anxiety disorder)
- Weakness in the legs
- Blood pooling in the lower extremities, sometimes visible as purple or red discoloration
- Bladder dysfunction
The most common symptom is lightheadedness, reported by nearly 98 percent of POTS patients, followed closely by brain fog, fatigue, and palpitations. Most patients experience several of these symptoms simultaneously, and the combination can severely affect quality of life — many POTS patients report losing multiple days of productivity per week.
POTS is roughly five times more common in women than in men, and most patients are diagnosed between the ages of 15 and 50. It frequently begins after a triggering event: a viral illness (including Long COVID-19), a concussion or head injury, a car accident, surgery, pregnancy, or a period of prolonged stress.
The Brainstem: The Control Center for Autonomic Function
Related article
How the Vagus Nerve Drives POTS Symptoms: The Brainstem and Atlas Connection
Apr 09, 2026To understand why POTS often connects to the upper neck, you need to understand what the brainstem does.
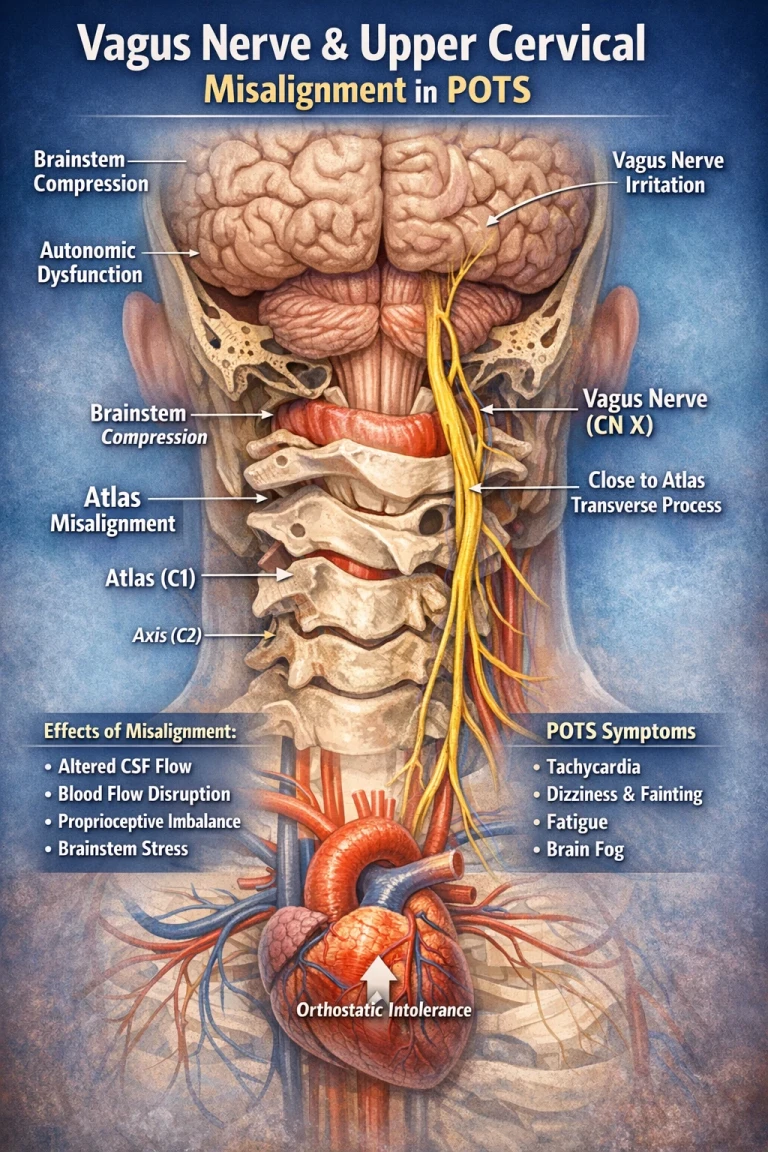
The brainstem is the structure that connects your brain to your spinal cord. It sits at the very base of the skull, directly behind and just above the atlas vertebra. It is small — roughly the size of your thumb — but it controls almost everything about how your body regulates itself moment to moment.
Within the brainstem are clusters of neurons that govern heart rate, blood pressure, respiration, swallowing, balance, and the sympathetic and parasympathetic branches of the autonomic nervous system. The vagus nerve — the longest cranial nerve and the primary parasympathetic pathway in the body — emerges from the brainstem and travels down through the neck to influence heart rate, gut function, and inflammation throughout the body.
In short, the brainstem is the command center for the very functions that go wrong in POTS. If brainstem function is disrupted — even subtly — the consequences cascade through the entire autonomic nervous system. Heart rate regulation becomes unreliable. Blood pressure responses lag or overshoot. Digestion slows. Temperature regulation falters. The whole system loses its ability to adapt smoothly to changes in posture and demand.
How the Upper Cervical Spine Affects the Brainstem
The atlas (C1) is the top vertebra of the spine and the one that supports the skull. Just below it sits the axis (C2). Together these two vertebrae form a region unlike any other in the spinal column. There are no discs between them, the brainstem passes directly through the opening they create, and the vertebral arteries thread through specific channels in the bone before entering the skull.
When the atlas shifts even slightly out of its proper position — usually as the result of a head or neck injury, a fall, a car accident, a sports concussion, or a difficult birth — it creates what upper cervical chiropractors call an atlas displacement complex. This is not a typical neck ache. It is a structural shift that can affect the brainstem in several ways:
It can create mechanical irritation of the brainstem and surrounding neural tissue. It can disrupt cerebrospinal fluid flow around the brain and upper cord. It can compromise venous drainage from the skull, leading to subtle changes in intracranial pressure. And — critically for POTS patients — it can disrupt the proprioceptive information that the brainstem relies on to know where the head is positioned in space.
Nerve Sensors and Brainstem Communication
There is something else that makes this region special: it is incredibly rich in nerve sensors.
The joints, muscles, and ligaments in your upper neck contain thousands of tiny receptors that constantly send information to your brain about where your head is positioned, how it is moving, and what the muscles around it are doing. In fact, this region has more of these sensors per square centimeter than almost anywhere else in your body (Kulkarni et al., 2001). The small suboccipital muscles at the base of the skull have some of the highest densities of muscle spindles found anywhere in the human body — up to 200 spindles per gram of muscle tissue.
These sensors feed directly into the brainstem and have powerful reflex connections to the vestibular system (your balance system), the visual system, and the autonomic control centers. When the upper cervical spine is misaligned, the information flowing from these sensors becomes distorted. The brainstem receives faulty input about head position and movement. It then issues faulty output to the systems it controls — including heart rate, blood pressure, and balance.

This is one reason POTS patients so often also experience dizziness, visual disturbances, brain fog, and balance issues. The same upper cervical dysfunction that disrupts autonomic regulation also disrupts the sensorimotor integration that those systems depend on.
What the Research Shows
The connection between upper cervical structural problems and POTS is increasingly supported in the literature.
A 2018 case report published in *Frontiers in Neurology* documented a 26-year-old female with POTS who underwent upper cervical chiropractic care combined with neurorehabilitation. After 12 weeks of care, the patient showed measurable improvements in resting heart rate, standing heart rate, and overall symptom burden. The authors concluded that further research into upper cervical chiropractic for POTS was warranted.
A 2022 study published in the *Journal of Family Medicine and Primary Care* by Chu and Lin reported on a 50-year-old woman with three years of lightheadedness, palpitations, and neck pain. Tilt table testing confirmed POTS, and imaging revealed cervical kyphosis and thoracic scoliosis. After three months of chiropractic care, the patient reported full resolution of neck pain, dizziness, and POTS symptoms. At 12-month follow-up, both her radiographic alignment and her POTS symptoms remained improved.
A 2024 case report by Trager and colleagues, published in *Cureus*, documented a patient with cervicogenic dizziness, upper cervical instability, and POTS. After eight months of conservative care including gentle manual therapy and cervical stabilization, her dizziness improved dramatically, with her Dizziness Handicap Inventory score dropping from 50 (moderate handicap) to 10 (less than mild handicap). The authors highlighted the importance of considering cervical spine dysfunction in the differential diagnosis of chronic dizziness and dysautonomia.
A separate 2022 case study in the *Journal of Upper Cervical Chiropractic Research* documented resolution of chronic POTS and dysautonomia following upper cervical correction, with sustained improvement at follow-up.
None of these are randomized controlled trials, and outcomes documented in case reports are not typical of every patient. But the consistency of the findings across independent investigators — and the biological plausibility of the mechanism — point to upper cervical care as an option worth understanding for POTS patients.
The Role of CBCT Imaging in Precision Care
One of the reasons upper cervical chiropractic care has advanced significantly over the past two decades is the availability of cone beam computed tomography, or CBCT. Traditional two-dimensional X-rays can show the upper cervical spine, but they have limitations when the goal is to measure the precise three-dimensional relationship between the skull, the atlas, and the axis.
CBCT changes that. It produces a high-resolution, three-dimensional image of the upper cervical region, allowing the doctor to see exactly how the atlas is positioned relative to the skull above and the axis below. Angles, rotations, and lateral shifts that would be invisible or ambiguous on a standard X-ray become measurable to a fraction of a degree.
For a region of the body where small structural changes can have outsized effects on the nervous system, this level of precision matters. Every spine is unique, and the angle of an atlas misalignment in one patient may be very different from another. Without precise imaging, the correction becomes generalized. With CBCT, the correction can be calculated specifically for that patient's anatomy and delivered with the appropriate vector, then verified with post-correction imaging to confirm that the structural change actually occurred.
For POTS patients, this precision is particularly important. The research connecting upper cervical care to POTS improvement consistently points to structural correction of the atlas as the variable that correlates with symptomatic change. Achieving that correction reliably is what CBCT-guided care is built to do.
What the Correction Actually Looks Like
One of the most common concerns we hear from POTS patients is fear of being adjusted. POTS sufferers often have hypersensitive nervous systems, and the thought of an aggressive chiropractic manipulation is understandably alarming. We want to be clear about this:
The upper cervical correction does not involve any popping, twisting, or pulling of the neck.
Instead, the correction is delivered with a gentle, precise, low-force impulse that is calculated specifically for the misalignment seen on your imaging. There is no cracking sound. There is no sudden rotation of the head. There is no manual traction. Most patients describe the correction as so light that they wonder whether anything happened at all — until they begin to notice changes in their symptoms in the hours and days afterward.
This is by design. The upper cervical region is too important and too delicate for force-based techniques. The goal is precision, not pressure, and the body responds to a correctly delivered correction with subtle but powerful neurological changes.
What This Means for POTS Patients in Sarasota
If you have been diagnosed with POTS — or if you suspect you have it but haven't yet received a diagnosis — there are several things worth considering.
First, a history of head or neck trauma is common among POTS patients. Many people who develop POTS can trace its onset to a specific event: a concussion, a car accident, a fall, a viral illness that hit hard. Any of these can affect the structural integrity of the upper cervical spine and the function of the brainstem.
Second, upper cervical chiropractic care does not claim to cure POTS. What the research suggests is that for a meaningful number of POTS patients, addressing the underlying structural problem at the top of the neck is associated with reduced symptoms, improved function, and better quality of life. Results vary from person to person.
Third, the kind of care we are describing is specific. It is not a general chiropractic adjustment. It focuses on the precise structural relationship at C1 and C2, uses CBCT imaging to inform the correction, and avoids any high-force manipulation. It is a different kind of care, designed for a different kind of problem.
If you would like to learn whether your POTS symptoms may be connected to an underlying upper cervical structural issue, the first step is a thorough evaluation that includes precision imaging of your craniocervical junction. From there, you and your doctor can discuss whether a structural correction is appropriate for your case.
The research is real. The mechanism is biologically plausible. And the option is available right here in Sarasota.
**References**
1. Kulkarni V, Chandy MJ, Babu KS. *Quantitative study of muscle spindles in suboccipital muscles of human foetuses.* Neurology India, 2001; 49(4): 355-359.
2. Chung J. *Improvements in resting heart rate and symptoms of postural orthostatic tachycardia syndrome in a 26-year-old female under upper cervical chiropractic care and neurorehabilitation.* Frontiers in Neurology, 2018.
3. Chu ECP, Lin AFC. *Relief of postural orthostatic tachycardia syndrome with chiropractic rehabilitation.* Journal of Family Medicine and Primary Care, 2022; 11(7): 4006-4009.
4. Trager RJ, Schuster A, Tao C, Zamary G. *Conservative management of cervicogenic dizziness associated with upper cervical instability and postural orthostatic tachycardia syndrome: A case report.* Cureus, 2024.
5. *Resolution of Chronic Postural Orthostatic Tachycardia Syndrome (POTS) & Dysautonomia Following Chiropractic Care: A Case Study & Review of Literature.* Journal of Upper Cervical Chiropractic Research, 2022.



Leave a comment