
"Why the nerves at the top of your neck may be quietly driving your reflux — and what a precision-based upper cervical correction can do about it"
If you have been on a proton pump inhibitor for months or years and still find yourself reaching for antacids, you already know that medication doesn’t always fix the underlying problem. It can lower the acid your stomach produces, but it does not change the reason that acid is making it past the valve at the top of your stomach in the first place. For many people in Sarasota dealing with chronic acid reflux disease, that question — why is the valve not closing properly — never gets answered.
Schedule Your Appointment
Schedule appointmentThere is an answer that mainstream gastroenterology has documented in its own peer-reviewed literature but rarely communicates to patients: the valve at the bottom of the esophagus, the lower esophageal sphincter, is smooth muscle. It does not have a switch. It does not respond to willpower. Its tone is controlled almost entirely by the brainstem through the vagus nerve. When that neurological control weakens or becomes dysregulated, the sphincter’s ability to stay closed weakens with it — and reflux becomes a chronic problem regardless of what you eat, drink, or take.
This article walks through how that neurological control actually works, why the upper cervical spine plays a meaningful role in it, and what a precision-based, gentle correction can offer for patients who want a natural path to relief.
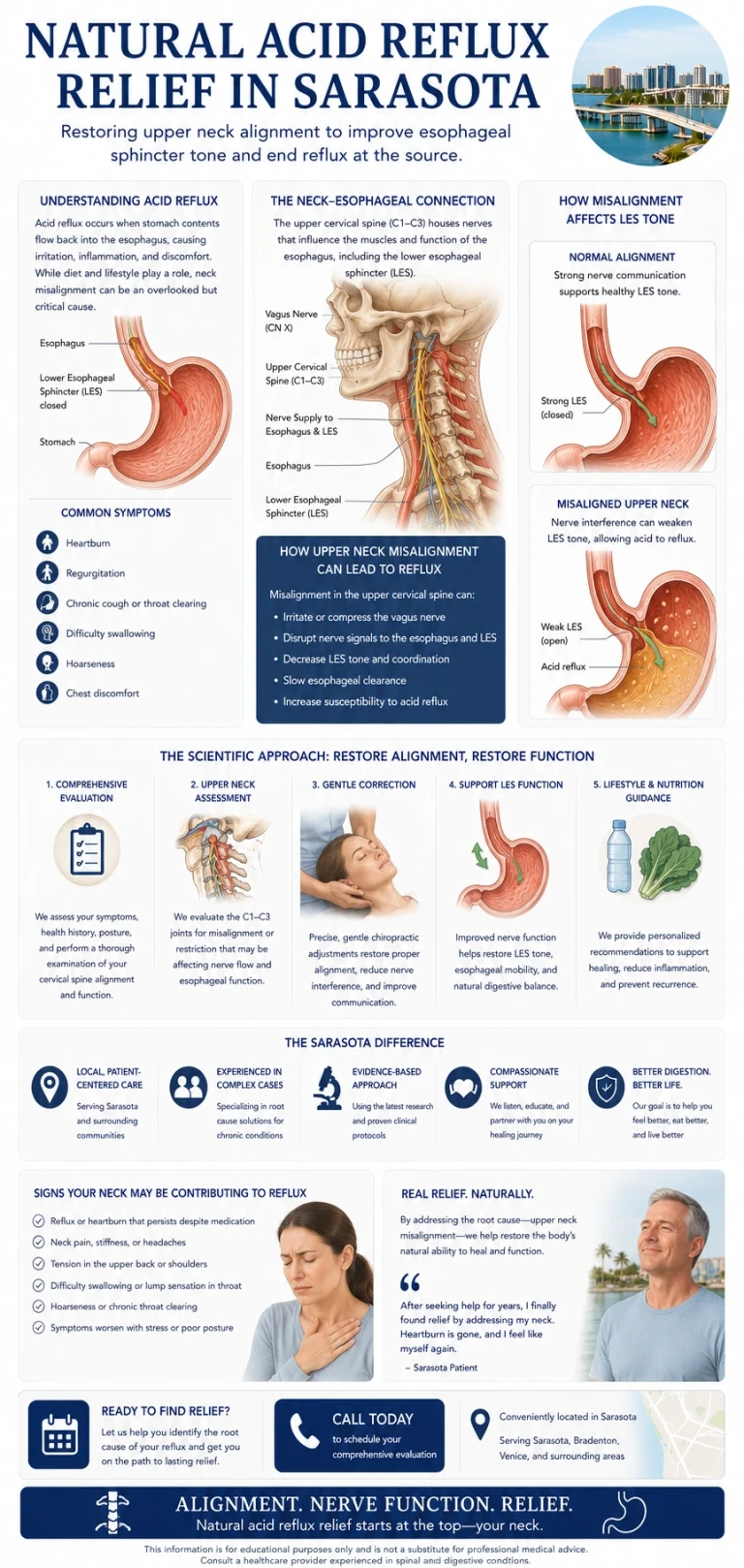
The Valve That Decides Whether You Have Reflux
The lower esophageal sphincter (LES) sits where the esophagus meets the stomach. It is not a separate organ — it is a specialized thickening of the smooth muscle in the wall of the esophagus, about two to five centimeters long. Working alongside it is the crural diaphragm, the part of your diaphragm that wraps around the esophagus and acts as an external sphincter. Together, these two structures form the anti-reflux barrier.
When that barrier is working properly, it stays closed at rest, opens precisely when you swallow, and closes again immediately after. When it is not working properly, two main things can go wrong. The LES can have a low baseline resting tone — it is weak when it should be strong. Or the LES can undergo what gastroenterologists call transient lower esophageal sphincter relaxations (tLESRs) — brief, inappropriate openings of the sphincter that allow stomach contents to wash back into the esophagus. Peer-reviewed literature has described tLESRs as the principal mechanism of gastroesophageal reflux disease. Both problems — weak resting tone and inappropriate transient relaxations — share the same underlying control system.
The Brainstem and the Vagus Nerve: Where the LES Gets Its Signal
Smooth muscle, including the muscle of the LES, does not work the way the muscles in your arm do. You cannot consciously tighten your esophageal valve any more than you can consciously slow your own heart rate. These muscles are under autonomic control, and the central command center for the digestive tract’s autonomic regulation is in the brainstem.
Specifically, the dorsal motor nucleus of the vagus and the nucleus tractus solitarius — two structures in the medulla, the lowest part of the brainstem — are responsible for sending signals down to the LES and receiving sensory information back from it. These signals travel through the vagus nerve, the tenth cranial nerve, which exits the skull through the jugular foramen at the base of the skull and runs down through the neck on its way to the digestive tract.
The vagus nerve sends two kinds of signals to the LES. Excitatory signals, carried primarily by acetylcholine, tell the sphincter to contract and stay closed. Inhibitory signals, carried by nitric oxide and vasoactive intestinal polypeptide, tell it to relax. The balance between these two streams determines the sphincter’s tone at any given moment. When that balance shifts toward weak excitation or excessive inhibition — in other words, when the neurological tone driving the sphincter is compromised — the valve loses its grip, and reflux becomes much more likely.
This is well-established gastroenterology. It is the reason researchers have spent years investigating ways to modify vagal control of the LES as a treatment target for GERD. What is less commonly discussed in patient settings is the mechanical part of the equation — what happens to vagal function when the structure surrounding the vagus nerve is itself under stress.
The Neuromechanical Connection: Why the Top of Your Neck Matters
The vagus nerve exits the skull through the jugular foramen, an opening at the base of the skull located directly adjacent to the atlas — the first cervical vertebra (C1). The brainstem itself sits at the level of the craniocervical junction, where the skull meets the upper cervical spine. Almost everything that controls digestive autonomic function passes through, or sits immediately next to, this small anatomical region.
When the atlas or axis is misaligned, the structures of the craniocervical junction can be placed under mechanical stress. That stress can do several things at once. It can subtly affect the local environment around the vagus nerve as it exits the skull. It can alter cerebrospinal fluid dynamics and venous drainage in a way that influences brainstem function. And it can disrupt the upper cervical mechanoreceptor input that feeds into the brainstem itself — the same brainstem that contains the dorsal motor nucleus of the vagus, which controls the LES.
This is what a neuromechanical cause of reflux looks like in practice. The acid is real. The symptoms are real. But the root cause isn’t necessarily the stomach producing too much acid or the diet. It is a sphincter that has lost its neurological tone because the system that controls it has been compromised — sometimes for years, often dating back to a head or neck injury the patient has long since forgotten.
What the Research Shows
Related article

The research in this specific area is still developing, but several clinically relevant findings are worth understanding.
A 2021 case report published in the journal Clinics and Practice described a 35-year-old woman with diagnosed GERD — confirmed by endoscopy showing inflammation at the gastroesophageal junction — alongside chronic neck pain and postural dysfunction. After cervical spinal correction over the course of several weeks, her neck pain resolved and her reflux symptoms resolved concurrently. She was able to discontinue her antacid and H2 blocker medications. At twelve-month follow-up, she remained symptom-free. The authors concluded that the cervical spine should be considered in patients with GERD, particularly when neck symptoms and reflux occur together.
Additional case reports in chiropractic and pediatric literature have described similar improvements in adults and infants — including a notable case series in which infants with GERD, feeding difficulties, and sleep disturbances saw symptom resolution after upper cervical correction. None of these are randomized controlled trials, and they don’t prove a definitive cause-and-effect relationship. What they do show is a consistent pattern: when the upper cervical spine is addressed in patients with reflux, a meaningful number of them experience real improvement. Combined with the established neuroanatomy of LES control, the case for evaluating the upper cervical spine in chronic reflux patients is mechanistically reasonable and clinically supported.
CBCT Imaging: Precision Before Anything Else
Before any care begins in our Sarasota office, we use Cone Beam Computed Tomography (CBCT) imaging of the upper cervical spine. CBCT is a precision imaging tool that produces three-dimensional views of the skull base, atlas, axis, and surrounding structures — detail that flat two-dimensional X-rays cannot provide.
Every craniocervical junction is built differently. The angles, the orientations, and the relationships between the skull, C1, and C2 are unique to each person. Without precision measurements, an upper cervical correction is a guess. With them, the correction can be specific, gentle, and matched to your exact anatomy. For a patient who has been told their reflux is something to manage indefinitely with medication, this is often the first time the structure most likely to be influencing the underlying neurology is being looked at directly.
No Twisting. No Cracking. No Pulling of the Neck
Most people picture a chiropractic adjustment as a fast head-turn and a popping sound. That is not what we do. The correction we deliver is specific, low-force, and based directly on the measurements taken from your CBCT scan. There is no twisting, cranking, or pulling. No cavitation noise. You lie on your side with your head supported. The correction takes seconds.
Gentle does not mean ineffective. Gentle means we are working with the nervous system, not against it. The goal is to give the brainstem cleaner input from the upper cervical joints and to restore optimal mechanical conditions for the vagus nerve and surrounding structures — so the autonomic control of your digestive tract can function the way it was designed to.
Who This Tends to Help
The patient we see most often in this category has a story that sounds familiar. Chronic reflux that started, or worsened significantly, after a specific event — a car accident, a fall, a sports injury, a difficult labor and delivery, or sometimes simply a long period of postural stress. A diagnosis of GERD. A course of proton pump inhibitors that worked for a while and then plateaued. Lifestyle changes that helped modestly but did not solve the problem.
Common features include reflux that occurs even when diet is controlled, neck pain or stiffness the patient may not have connected to the digestive symptoms, a history of head or neck trauma, and a sense that the medications are managing symptoms rather than addressing whatever is really going on. None of these features are diagnostic on their own — but together, they raise the question of whether the upper cervical spine is part of the picture.
A Realistic Path Forward
Reflux is rarely caused by one thing alone. Diet, weight, hiatal hernia, stress, alcohol, late meals, and medication all matter. We do not pretend that upper cervical care replaces any of these considerations. What it can offer is a piece that often goes missing — a look at the neurological control system that determines whether your sphincter has the tone it needs in the first place.
A first visit in our Sarasota office includes a thorough consultation, a focused examination, and CBCT imaging of the upper cervical spine. We pay particular attention to your history of head and neck injuries, even minor ones. After we review the imaging with you, we will tell you honestly whether upper cervical care looks like a good fit. If it does, we build a plan. If it does not, we say so and point you toward what is more likely to help.
If you are searching for natural acid reflux disease relief in Sarasota and you are tired of treating the symptom rather than the source, the next step is a conversation. The valve isn’t broken on its own. Something is telling it to be weak. The most important question you can ask is what.
Ready to take the next step? Schedule a consultation at our Sarasota office to find out whether upper cervical chiropractic care could be part of your reflux solution.
References: Mittal RK, Balaban DH. The esophagogastric junction. Pathophysiology of Gastroesophageal Reflux Disease: Motility Factors. • Tipnis NA, Rhee PL, Mittal RK. Neuro-regulation of lower esophageal sphincter function as treatment for gastroesophageal reflux disease. World J Gastroenterol. 2008. • Hornby PJ, Abrahams TP. Central control of lower esophageal sphincter relaxation. Am J Med. 2000. • Welch B. Resolution of Gastroesophageal Reflux Disease Following Correction for Upper Cross Syndrome — A Case Study and Brief Review. Clinics and Practice. 2021. • Alcantara J, Anderson R. Chiropractic care of a pediatric patient with symptoms associated with gastroesophageal reflux disease. J Can Chiropr Assoc. 2008.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Persistent reflux should be evaluated by a qualified healthcare provider to rule out serious causes including hiatal hernia, Barrett’s esophagus, and other conditions. Upper cervical chiropractic care does not diagnose, treat, or cure gastroesophageal reflux disease. Patients should not discontinue prescribed medications without consulting their physician. Individual results vary.



Leave a comment