
If you can change your ringing by clenching your jaw or turning your head, your tinnitus is telling you something: for many people, the neck is part of the signal.
Sarasota Upper Cervical · Tinnitus Relief Serving Sarasota, Lakewood Ranch, North Port, Venice, Punta Gorda, and Bradenton
Schedule Your Appointment
Schedule appointmentTinnitus Doctor Sarasota
What this guide covers:
1.What tinnitus actually is
2.The clue most people miss: somatic tinnitus
3.The switchboard in your brainstem (the DCN)
4. Five ways the neck reaches the hearing system
5.Why the upper neck specifically
6.Where upper cervical care fits
7.What it does — and doesn't — do
8.Our approach in Sarasota
9.FAQ
Tinnitus - ringing, buzzing, hissing, pulsatile or humming with no outside source, is one of the most frustrating symptoms a person can live with, partly because so many people are told the same thing: "There's nothing that can be done; learn to live with it." That advice comes from treating tinnitus as purely an ear problem. But for a meaningful number of people, the ear isn't the whole story. The hearing system is wired directly into the nervous system, and one of its closest neighbors is the top of your neck.
This guide explains that connection in plain language - how signals from your neck, jaw, and surrounding muscles can reach the hearing pathway in your brainstem, why that can turn the volume of your tinnitus up or down, and where upper cervical care fits in (and where it doesn't).
First, what tinnitus actually is
Tinnitus is the perception of sound without a matching sound in the environment. It isn't a disease in itself, it's a symptom, the way a fever is a symptom. It can come from noise exposure, age-related hearing change, earwax, certain medications, jaw problems, neck problems, and more. Because the causes vary, the right help varies too, which is exactly why understanding your tinnitus matters more than chasing a one-size-fits-all fix.
Here's the key idea that reframes everything: tinnitus is generated, in large part, by the nervous system — not only by the ear. The brain has a hearing pathway that processes sound, and that pathway can become overactive and "fill in" sound that isn't there. Once you understand that, the neck connection stops being mysterious.
The clue most people miss: somatic tinnitus
Here's something you can test right now to clarify if its somatic tinnitus or not. Clench your jaw firmly. Turn your head hard to one side. Press on the muscles at the top of your neck, just below the skull. For a large share of people with tinnitus, one of these movements changes the ringing — its volume, its pitch, or its quality shifts.
That phenomenon has a name: somatic tinnitus ("somatic" simply means "of the body"). It's the well-documented observation that input from the head, neck, or jaw can modulate the tinnitus signal. And it's a profound clue, because a pure ear problem shouldn't change when you move your neck. If your ringing responds to jaw or neck movement, it's strong evidence that your body — your neck and jaw — is feeding into the sound. The question is: how does a neck signal reach the hearing system at all?
The takeaway
If clenching, head-turning, or pressing on your upper neck changes your ringing, that's somatic tinnitus ,and it points toward the neck and jaw as part of the cause, not just the ear.
The switchboard in your brainstem: the DCN
The answer is a small but remarkable structure in the brainstem called the dorsal cochlear nucleus, or DCN. Think of it as a switchboard at the very first stop of the hearing pathway, the first place sound signals from the ear land inside the brain.
The crucial part: the DCN doesn't only receive sound. It's a meeting point. It also takes in body-sense signals from the neck, the jaw, and the surrounding nerves — the same kind of "where are my muscles and joints right now" signals your body uses to know its own position. Auditory input from the ear and physical input from the neck and jaw arrive at the same switchboard, side by side.
When those body signals are normal, the switchboard runs smoothly. But when the neck or jaw is sending a steady stream of irritated or distorted signals, that noise can spill over into the hearing side of the switchboard — and the brain can interpret it as sound. That's the heart of the neck–tinnitus connection: a body signal getting read as a sound signal, because they share the same junction.
Five ways the neck reaches the hearing system
Researchers have mapped several distinct routes by which the neck, jaw, and nearby structures feed into that brainstem switchboard. Here are the five that matter most — each translated into plain terms.
Pathway 01 Somatosensory input — neck and jaw signals reaching the hearing pathway
This is the umbrella route. The DCN directly receives sensory input from the upper neck's nerve roots, from the jaw and face (the trigeminal system), and from the body's position-sense pathways. So irritation anywhere in that neighborhood has a literal wire into the hearing switchboard. This is the anatomical reason somatic tinnitus exists at all.
Pathway 02 Joint signals from the upper neck (joint afferentation) also known as proprioception.
The small joints at the top of your spine are packed with sensors that constantly report their position and movement to the brain. When the top vertebrae aren't aligning or moving well, those sensors send a distorted report. Because that report feeds into the same brainstem region as hearing, a misaligned, irritated upper-neck joint can become a steady source of "static" on the hearing line.
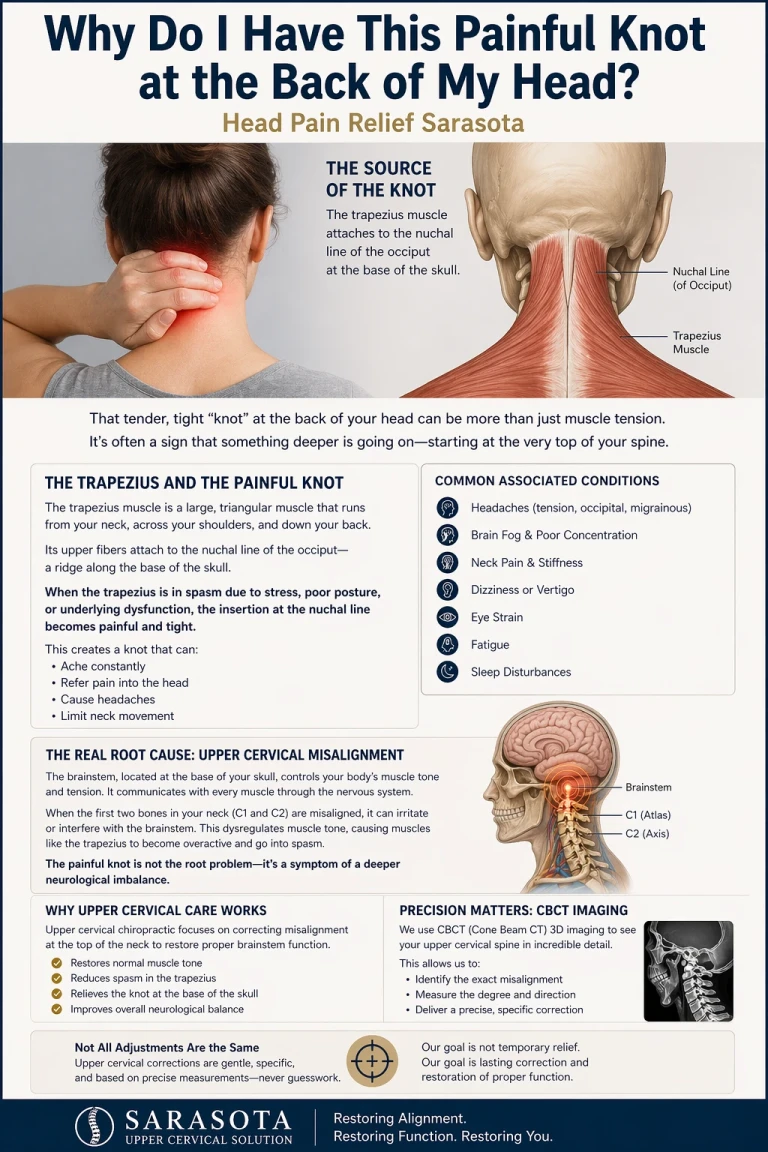
Pathway 03 Suboccipital muscle signals (muscle spindle input)
The suboccipital muscles — the small, deep muscles right at the base of your skull — are unusually rich in tiny sensors called muscle spindles, far more densely than most muscles in the body. Their job is to fine-tune head position with great precision. When these muscles are chronically tight or strained (think long hours at a screen, or an old neck injury), they flood the nervous system with abnormal signals — and once again, those signals feed toward the same hearing-related pathways. This is one of the most direct neck-to-tinnitus routes.
Pathway 04 The ear's own muscles and the jaw (stapedius and trigeminal pathways)
Inside your middle ear sits a tiny muscle called the stapedius, along with its neighbor the tensor tympani. These muscles are controlled by cranial nerves — including the trigeminal system that also serves the jaw. In some people, these muscles can contract abnormally or rhythmically (a spasm sometimes called middle-ear myoclonus), which can produce a clicking or buzzing. This is a less common cause overall, but it's a real one — and it matters here because the same nerves that drive these ear muscles also carry jaw and facial signals, tying the ear, jaw, and brainstem together on shared wiring. It's another reason jaw and neck input can register in the hearing system.
Pathway 05 Blood flow and brainstem dynamics
The top of the neck is also a busy corridor for blood vessels and for the brainstem structures that regulate them. Altered mechanics and irritation in this region can influence local circulation and the sensitive brainstem centers nearby. While this is the least specific of the five pathways, it rounds out the picture: the upper neck isn't just near the hearing system — it shares its nerves, its muscles, and its circulatory neighborhood.
The common thread
Every one of these five pathways converges at the craniocervical junction — the place where your skull meets the top of your spine. That single region is wired into the hearing switchboard through nerves, joints, muscles, and blood flow. It's why the upper neck is such a recurring character in tinnitus that responds to movement.
Why the upper neck specifically?
The top two vertebrae — the atlas and axis — sit directly beneath the skull and carry the head's weight while allowing a huge range of motion. That makes the region both powerful and demanding: it depends on balanced alignment and steady muscular support to function quietly. When that alignment is disturbed — by an old whiplash, a fall, a sports injury, or years of forward-head posture — the joints, muscles, and nerve sensors of the upper neck can become a chronic source of irritated signaling. And as we've seen, that signaling has a direct line into the hearing pathway. It's no coincidence that so many people with neck-responsive tinnitus also have a history of neck trauma or persistent upper-neck tension.
Related article

Why Do My Hands Always Get Cold and Then Hot? | Raynaud's Relief and Doctor in Sarasota
May 12, 2026Signs your tinnitus may have a neck or jaw component
Your ringing changes when you clench your jaw, turn your head, or press on your upper neck.
It's worse on one side, and that's also your stiffer or more painful side.
It started or worsened after a neck injury, whiplash, or concussion.
It comes bundled with neck tightness, headaches, or jaw symptoms.
Your ears have been checked and found healthy, yet the ringing persists.
None of these is a self-diagnosis — they're the patterns that make a proper upper cervical evaluation worthwhile.
Where upper cervical care fits
Upper cervical chiropractic focuses on the alignment and movement of those top two vertebrae. The logic for tinnitus follows directly from the five pathways: if irritated signals from the upper neck's joints, muscles, and nerves are feeding into the hearing switchboard, then restoring balanced alignment and reducing that irritation addresses the signal at its source — rather than trying to mask the sound.
In practice, that means gentle, precise corrections to the upper neck — not the forceful twisting people often picture with chiropractic. The goal is to quiet the abnormal body-signal "static" reaching the DCN, so the hearing pathway has less to misread.
What upper cervical care does — and does not — do
Honesty about scope is part of doing this well:
Upper cervical care addresses the cervical (neck) contribution to tinnitus — most relevantly when your tinnitus is the somatic, movement-responsive type.
It does not restore hearing loss, remove earwax, treat ear infections, or fix damage inside the ear itself.
It does not cure tinnitus, and it isn't the answer for tinnitus that's purely noise- or age-related with no neck or jaw component.
It is not a substitute for evaluation by your physician or audiologist — especially for tinnitus in only one ear, pulsatile (heartbeat-like) tinnitus, or tinnitus with hearing loss or dizziness, which need medical work-up.
For the right person — the one whose ringing changes with neck and jaw movement — addressing the upper neck can be a meaningful part of the picture. Individual results vary, and an examination is the only way to know whether your upper neck is involved in your case.
How we approach tinnitus and the neck in Sarasota
At Sarasota Upper Cervical, the first step is always evaluation, not treatment. We take a careful history — including any past neck trauma, whiplash, or jaw issues — and check whether your tinnitus responds to neck and jaw movement, along with how the top of your neck is aligning and moving. If we find an upper cervical pattern that fits your symptoms, we'll explain it plainly and discuss whether gentle upper cervical care is appropriate for you.
And if your tinnitus doesn't fit the cervical picture, we'll tell you honestly and point you toward the right provider — an audiologist or physician. Sending you to the right place is part of doing this well.
Does your ringing change when you move?
If clenching your jaw or turning your head changes your tinnitus, your neck may be part of the picture. An upper cervical evaluation can help you find out.
Frequently asked questions
1.Can a neck problem really cause tinnitus?
Related article
Why do I have this painful knot at the back of my head | Head Pain relief sarasota
Apr 23, 2026For some people, yes — it's called somatic tinnitus. Signals from the upper neck, jaw, and surrounding muscles feed into the same brainstem structure that processes hearing, the dorsal cochlear nucleus. When those body signals are irritated or distorted, they can be misread as sound. A telltale sign is tinnitus that changes when you clench your jaw, turn your head, or press on your upper neck.
2.Why does my tinnitus change when I move my jaw or neck?
Because the nerves carrying jaw and neck sensation connect into the hearing pathway at a shared brainstem switchboard. When you clench or turn, you change those body signals, which can shift the volume, pitch, or quality of the ringing. This responsiveness is the hallmark of somatic tinnitus and suggests the neck or jaw is part of the cause.
3.Does upper cervical care cure tinnitus?
No. Upper cervical care does not cure tinnitus. It focuses on the neck's contribution to tinnitus — most relevantly the somatic, movement-responsive type — by addressing irritation and alignment at the top of the neck. In many cases many different types of tinnitus can impoorve or remit completly.
4. What is the dorsal cochlear nucleus, in simple terms?
It's a small structure in the brainstem that acts as the first switchboard of the hearing pathway. It receives sound signals from the ear and, importantly, body-position signals from the neck and jaw at the same junction. That shared wiring is why neck and jaw irritation can register as sound.
5.When should I see a doctor instead?
Seek medical evaluation promptly for tinnitus in only one ear, pulsatile tinnitus that beats with your heart, tinnitus with sudden hearing loss, severe dizziness, facial weakness, or tinnitus after a head injury. These need a medical work-up. Upper cervical care is not a substitute for that.
6.Where can I get help for neck-related tinnitus in Sarasota?
Sarasota Upper Cervical serves the Sarasota and Bradenton area and focuses on the upper cervical contribution to tinnitus. You can request a consultation to find out whether your upper neck is part of the picture, and we'll refer you to an audiologist or physician when that's the right path.
References
Shore SE, et al. Somatosensory influences on the cochlear nucleus and the neural basis of somatic tinnitus.
Levine RA. Somatic (craniocervical) tinnitus and the dorsal cochlear nucleus hypothesis. American Journal of Otolaryngology.
Dehmel S, Shore SE. Convergence of somatosensory and auditory input in the dorsal cochlear nucleus.
Middle Ear Myoclonus / Tensor Tympani Syndrome. StatPearls, NCBI Bookshelf.
Hack GD, et al. Anatomic relationship between the suboccipital musculature and the dura (suboccipital connective tissue / muscle spindle density).
Bartsch T, Goadsby PJ. Anatomy and physiology of pain referral in the trigeminocervical complex.
This guide is for general educational purposes only and does not constitute medical advice, diagnosis, or treatment, and it does not establish a doctor–patient relationship. Tinnitus has many possible causes and requires professional evaluation to diagnose; some causes require medical or audiological work-up. Results of upper cervical care vary from person to person, and no specific outcome is promised or guaranteed. If you have tinnitus in one ear only, pulsatile tinnitus, sudden hearing loss, severe dizziness, or tinnitus following a head injury, seek medical care promptly. Always consult your physician or other qualified health provider with quest



Leave a comment