
"Why the vagus nerve, the cervical spine, and a loss of normal neck curve may be the missing piece in unexplained, persistent nausea"
Chronic nausea is one of the most disruptive and misunderstood symptoms in modern medicine. Patients describe a constant, low-grade queasiness that never fully goes away, a sense that the stomach is unsettled, waves of nausea triggered by food, motion, or even certain head positions, and an inability to function normally because the symptom is always present in the background. For many patients, the standard workup begins and ends in the gastrointestinal system. Endoscopy, gastric emptying studies, blood panels, and imaging are ordered. Reflux medications, anti-nausea drugs, and dietary changes are tried. The findings are often unremarkable, the relief is incomplete, and the diagnosis ends up being something vague — functional dyspepsia, idiopathic nausea, or simply nausea of unknown cause.
Schedule Your Appointment
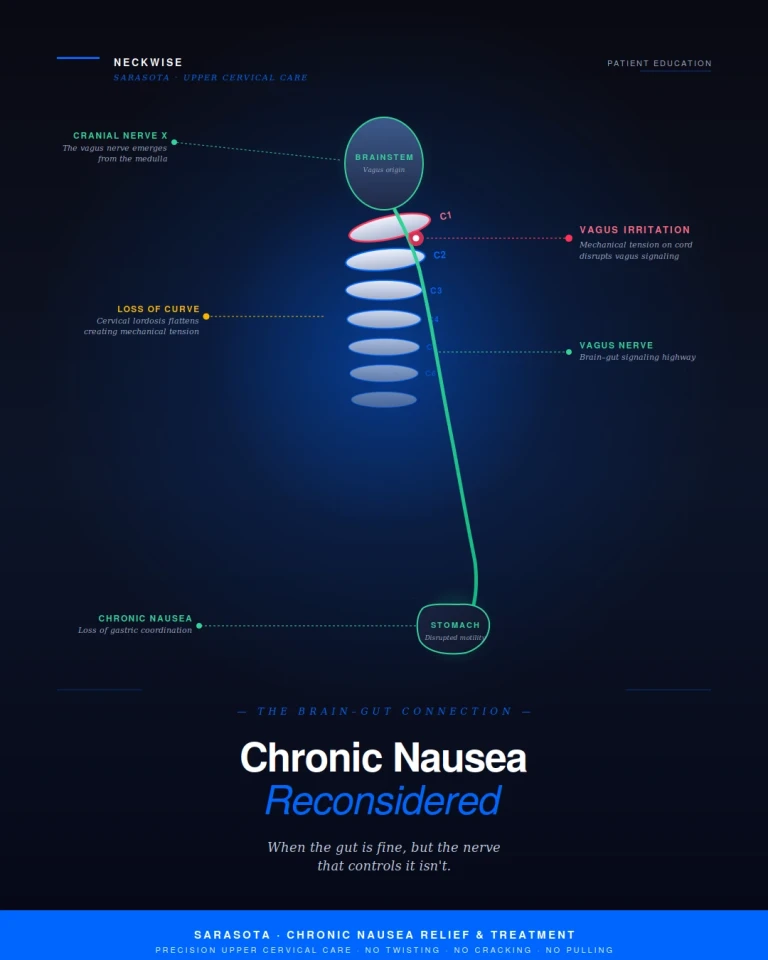
Schedule appointmentAt Neckwise in Sarasota, we focus on a part of the picture that the conventional gastrointestinal workup is rarely designed to evaluate. The stomach does not regulate itself in isolation. It is governed by the vagus nerve, and the vagus nerve emerges from the brainstem and travels directly through the cervical spine on its way to the gut. When the upper cervical spine is misaligned and the normal curve of the neck is lost, the resulting mechanical tension on the spinal cord and surrounding tissues can disrupt vagus nerve function. For a meaningful subset of patients with persistent, unexplained nausea, this is the missing piece.
The Vagus Nerve: The Brain-Gut Highway
The vagus nerve, also known as cranial nerve ten, is the longest and most influential nerve of the parasympathetic nervous system. It emerges from the brainstem at the level of the medulla, exits the skull through the jugular foramen at the base of the skull, and descends through the neck alongside the carotid artery and internal jugular vein. From there, it continues down through the chest and abdomen, branching extensively into the heart, lungs, esophagus, stomach, liver, pancreas, kidneys, and intestines.
In the context of nausea, the vagus nerve is the primary nerve that controls the stomach. It regulates gastric motility — the rhythmic muscular contractions that move food through the digestive tract. It controls the production and release of digestive enzymes and stomach acid. It signals to the brain when the stomach is full, when it is empty, and when something is wrong. It also carries information back from the gut to the brain, informing the central nervous system of the digestive system's status in real time.
When the vagus nerve is functioning normally, the stomach empties on schedule, motility is coordinated, and the brain-gut signaling that governs appetite, fullness, and nausea operates within a narrow physiological range. When vagus nerve function is disrupted, that entire system loses its coordination. Gastric motility slows, food sits longer than it should, and the brain begins receiving abnormal signals from a digestive system that is no longer operating the way it was designed to.
The Cervical Spine and the Loss of Normal Curve
The healthy cervical spine has a gentle forward curve called a lordosis. This curve is not cosmetic — it is mechanically essential. The lordotic curve allows the seven cervical vertebrae to bear the weight of the head efficiently, distributes load across the discs and joints, and gives the spinal cord the room it needs to lie comfortably within the spinal canal without being placed under tension.
When the upper cervical spine is misaligned, the curve of the entire neck changes. The atlas, sitting at the very top of the spine and supporting the full weight of the head, sets the foundation for everything below it. When the atlas shifts even fractions of a millimeter out of its ideal position, the rest of the cervical spine compensates. The lower cervical vertebrae adjust their angles to keep the head as level as possible, the supporting muscles work harder on one side than the other, and over time the natural lordotic curve straightens out. In more advanced cases, the curve can reverse entirely — a condition known as cervical kyphosis or military neck.
This change in geometry is not benign. The spinal cord runs through the center of the cervical spine, and it is anchored above to the brainstem and below to the rest of the spinal canal. When the curve of the neck flattens or reverses, the spinal cord is forced to take a longer, straighter path through a structure that is no longer the right shape for it. The cord and the surrounding tissues are placed under sustained mechanical tension that they were never designed to bear.
How Mechanical Cord Tension Affects Vagus Nerve Function
Related article

Post-Viral POTS: Why Autonomic Symptoms Persist After Infection | Sarasota
Jul 28, 2026
The vagus nerve does not simply pass through empty space on its way down from the brainstem. It travels in close proximity to the spinal cord, the brainstem, the dural membranes that surround the central nervous system, and the muscles and connective tissues of the upper neck. When the cervical curve is lost and mechanical tension develops in this region, several things happen at once.
The brainstem, where the vagus nerve originates, can become irritated by mechanical stress at the craniocervical junction. The dural membranes that surround the brainstem and upper spinal cord can be placed under tension, and dural tension is increasingly recognized in the literature as a contributor to autonomic dysfunction. The deep neck muscles can hold sustained, asymmetric contractions that compress the soft tissue corridor through which the vagus nerve descends. The internal jugular vein, which sits adjacent to the vagus in the carotid sheath, can be partially compressed by the same mechanical pattern, contributing to venous backflow that further irritates the surrounding nerve tissue.
The result is a vagus nerve that is mechanically irritated along its path and that is receiving abnormal input from a brainstem under sustained stress. The signals it sends to the stomach and the rest of the digestive tract become disorganized. Gastric motility loses its rhythm. The brain-gut signaling that governs nausea begins to misfire. The patient experiences chronic, unexplained queasiness that has no apparent cause in the gut itself — because the problem is not in the gut. The problem is in the nerve that controls the gut, and the nerve is being mechanically irritated upstream.
Why Conventional Workups Often Miss This
Standard gastrointestinal evaluations are designed to look at the gastrointestinal system. Endoscopy examines the lining of the stomach and esophagus. Gastric emptying studies measure how quickly food leaves the stomach. Blood work screens for inflammation, infection, and metabolic causes. Imaging looks for structural abnormalities. These are appropriate and necessary studies that rule out serious pathology, and they should be performed.
What these studies are not designed to evaluate is the position of the upper cervical spine, the curvature of the cervical lordosis, the mechanical tension on the spinal cord, or the status of the vagus nerve as it descends through the neck. When all of those variables are normal, the GI workup correctly identifies a normal gut. When those variables are abnormal, the GI workup still shows a normal gut — because the gut itself is not the problem. The diagnosis ends up labeled functional or idiopathic, and the patient is left to manage symptoms without an answer to the underlying question.
This pattern is recognizable. Patients who eventually find their way to upper cervical care for nausea often share a similar history: a normal endoscopy, a normal gastric emptying study, normal imaging, a trial of reflux medication that did not fully resolve the symptoms, and a sense that their nausea is connected to something beyond the digestive tract. That sense is often correct.
Common Symptoms Patients Describe
Patients who present to Neckwise with chronic nausea linked to upper cervical dysfunction frequently report a constellation of symptoms that extends well beyond the digestive system. Common patterns include:
• Persistent, low-grade nausea that never fully resolves, often described as a constant unsettled feeling in the stomach
• Waves of nausea triggered by certain head positions, lying down, or turning the head
• Nausea that worsens with stress and improves when lying still
• A sense of fullness or bloating after eating even small amounts of food
• Loss of appetite and unintentional changes in weight
• Neck pain, neck stiffness, or tension at the base of the skull that often goes unmentioned during GI appointments
• Headaches, brain fog, or a sense of mental cloudiness alongside the nausea
• Dizziness or lightheadedness, particularly when changing positions
• Heart rate changes, palpitations, or a feeling that the autonomic nervous system is dysregulated
• A history of head or neck trauma — sometimes recent, often years or decades old
The presence of neck symptoms alongside the nausea is one of the strongest signals that the upper cervical spine is contributing. Patients often do not initially connect the two, because the nausea feels like a stomach problem and the neck pain feels like a separate issue. The mechanical reality is that they share the same upstream cause.
How Neckwise Evaluates and Corrects
The Neckwise process is built around objectivity. We do not guess at whether a misalignment is present and we do not adjust based on how the neck feels to the touch. We measure.
The evaluation begins with a comprehensive consultation and history, with particular attention to prior trauma, the timeline of the nausea, the pattern of associated symptoms, and any prior GI workup. We then use objective testing — including a leg balance test and infrared thermography — to determine whether the nervous system is showing measurable signs of upper cervical involvement. These screens are repeatable, evidence-based, and tell us whether the upper cervical spine is part of the picture or not.
If the screens point toward upper cervical involvement, we move to imaging. Neckwise uses CBCT 3D imaging as a precision tool to visualize the atlas, the axis, and the curvature of the cervical spine in three dimensions. Unlike a flat X-ray, CBCT produces a true three-dimensional model of the upper cervical region, and the misalignment is quantified in degrees and millimeters across all axes of motion. The imaging also reveals the loss of cervical lordosis when present, allowing us to see the full mechanical picture rather than guessing at it.
The Correction: No Twisting, No Cracking, No Pulling
The Neckwise correction is not what most people picture when they hear the word chiropractic. There is no twisting of the neck, no cracking or popping sound, and no forceful pulling or sudden movement of the head. This matters in general, and it matters even more for patients dealing with chronic nausea — because the autonomic nervous system in this population is already sensitive, and forceful manipulation can provoke symptoms rather than relieve them.
Instead, the patient lies on their side on a precisely engineered table. The doctor uses the measurements taken from the CBCT imaging to determine the exact angle and direction needed to guide the atlas back toward its ideal position. The correction is delivered as a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place. The intent is to give the body a precise mechanical input that allows it to release the misalignment on its own terms, so that the cervical curve has the opportunity to begin restoring itself and the mechanical tension on the cord and surrounding nerves can ease.
What Happens After the Correction
When the atlas is restored toward its ideal position, the cervical spine has the opportunity to begin rebuilding its natural curve. As the curve returns, the mechanical tension on the spinal cord eases. The dural membranes that surround the brainstem and cord are no longer being pulled in directions they were not designed to bear. The deep neck muscles that have been holding asymmetric contractions begin to release. The corridor through which the vagus nerve descends becomes less mechanically compromised.
Patients commonly report that the constant queasiness becomes intermittent, then occasional, then absent. Triggers that previously set off waves of nausea — certain head positions, stress, eating — lose their power. Appetite returns. Bloating decreases. The associated symptoms that travel with the nausea — neck tension, brain fog, dizziness, autonomic instability — often improve in parallel because they share the same upstream mechanical cause. Healing is not always linear, and progress in autonomic conditions tends to come in steps rather than all at once, which is why care is structured as a corrective program over weeks to months.
Upper cervical care is also designed to integrate alongside the rest of a patient's care team. We do not ask patients to stop medications or skip GI appointments. Our role is to address a specific mechanical and neurological factor that is consistently overlooked, and to bring that piece into the broader picture so the system as a whole has the best chance of recovery.
Finding Real Answers in Sarasota
If you are searching for chronic nausea relief and treatment in Sarasota, and especially if your gastrointestinal workup has come back clean, your reflux medication has not fully resolved the problem, and your nausea has become a daily reality, an upper cervical evaluation may be a meaningful next step. The connection between the vagus nerve, the cervical spine, and chronic nausea is anatomical, measurable, and addressable. It is consistently overlooked in conventional workups for the simple reason that the conventional workup is not designed to measure it.
Neckwise focuses on patients who have not found lasting answers in the conventional system. Objective testing, CBCT 3D imaging, and a precise correction with no twisting, cracking, or pulling offer a structured, evidence-based path to determine whether the upper cervical spine is contributing to your nausea — and if it is, to address it at the source so the body has the opportunity to recover.
To learn more or schedule a consultation, contact Neckwise Sarasota. Chronic nausea is real, exhausting, and often deeply isolating. For many patients, the answer begins with looking at a system the standard workup has not yet looked at — the corridor at the top of the neck where the vagus nerve makes its long journey from the brainstem to the gut.



Leave a comment