
How tight occipital muscles, upper cervical misalignment, and a precise correction without twisting, popping, or pulling can change the picture for chronic head pain.
Occipital neuralgia is one of the most misunderstood causes of chronic head pain. Patients describe sharp, electric, stabbing, or shocking sensations that begin at the base of the skull and shoot up the back of the head, often into the scalp, behind the eyes, or into the temples. The pain can be triggered by something as simple as turning the head, lying on a pillow, brushing the hair, or even a cool breeze on the back of the neck. For many patients, the condition is misdiagnosed as migraine, tension headache, or simply chronic neck pain — and treated accordingly, with limited results.
Schedule Your Appointment
Schedule appointmentAt Neckwise in Sarasota, we approach occipital neuralgia from a structural and neurological angle that is often overlooked in conventional care. Rather than asking only how to mute the pain, we ask why the occipital nerves are being irritated in the first place. The answer, in a significant number of cases, lies in the relationship between the upper cervical spine, the deep muscles at the base of the skull, and the greater and lesser occipital nerves themselves.
Understanding the Occipital Nerves
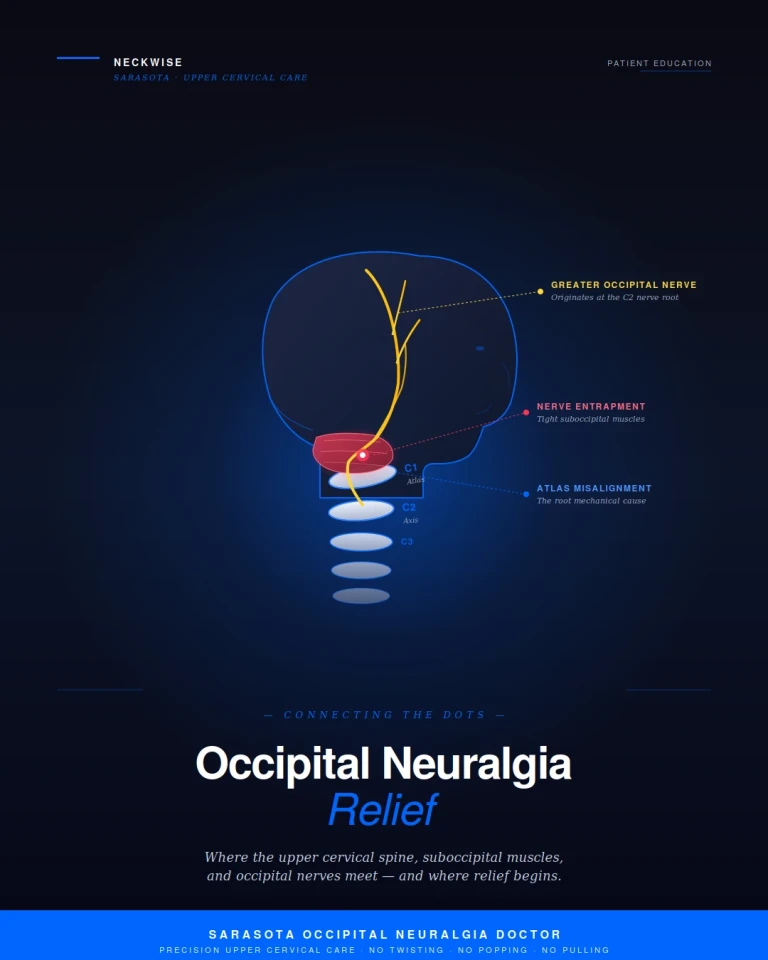
The greater occipital nerve and the lesser occipital nerve are responsible for sensation across the back and sides of the scalp. The greater occipital nerve originates from the C2 nerve root, emerges from between the upper cervical vertebrae, and travels through the deep suboccipital muscles before piercing the trapezius and fanning out across the back of the head. The lesser occipital nerve emerges from the C2 and C3 nerve roots and travels along the side of the neck to supply the area behind the ear and the upper side of the scalp.
Because of where these nerves originate and the path they travel, they are uniquely vulnerable. They have to thread their way through layers of muscle, fascia, and bone in a region that is mechanically demanding. Any sustained tension, mechanical irritation, or compression along that path can produce the firing pattern patients recognize as occipital neuralgia — sharp, lancinating pain that follows the territory of the nerve from the base of the skull upward.
How Tight Occipital Muscles Entrap the Nerves
Just below the base of the skull is a group of small but powerful muscles called the suboccipital muscles. These include the rectus capitis posterior major and minor, and the obliquus capitis superior and inferior. They are responsible for fine, precise movements of the head and play a key role in postural control. They are also some of the most densely innervated muscles in the human body, with an unusually high concentration of sensory receptors per square inch.
The greater occipital nerve must pass directly through and around these muscles on its way to the scalp. When the suboccipital muscles are healthy and balanced, the nerve travels its path freely. When those muscles become chronically tight, shortened, or inflamed, the result is mechanical entrapment. The nerve is squeezed, compressed, and irritated by the very tissue it is supposed to pass through. Over time, this leads to the hallmark symptoms of occipital neuralgia — pain at the base of the skull, scalp tenderness, sensitivity to touch, and the sharp, shocking sensations that radiate up the back of the head.
This is why so many occipital neuralgia patients describe their pain as starting at the base of the skull. They are correctly identifying the location of the entrapment. The deeper question is what is keeping those muscles in a state of chronic tightness in the first place.
The Upper Cervical Misalignment Connection
The suboccipital muscles do not become tight randomly. They tighten in response to mechanical stress, postural demands, or — most importantly for occipital neuralgia patients — a misalignment of the upper cervical spine.
The atlas (C1) is the top vertebra of the spine. It sits directly beneath the skull and supports the entire weight of the head, which averages 10 to 12 pounds. Below it sits the axis (C2), the vertebra from which the greater occipital nerve originates. The atlas is the only vertebra in the spine that does not have a disc above or below it. It relies on a delicate balance of ligaments and the suboccipital muscles to remain in position.
When the atlas shifts even a fraction of a millimeter out of its ideal alignment, the suboccipital muscles are forced to compensate. They contract asymmetrically and remain in that contracted state to hold the head as level as possible over an off-balance foundation. This is not a temporary spasm. It is a sustained, low-grade contraction that can persist for years. Over time, the muscles become chronically shortened, fibrotic, and unyielding — and the occipital nerves traveling through them are caught in the middle.
This is the connection that conventional treatment often misses. Massage, stretching, nerve blocks, and medication may temporarily reduce the muscle tension or quiet the nerve, but if the underlying upper cervical misalignment is still present, the muscles will return to their compensatory pattern and the entrapment will return with them. To resolve the issue at its source, the misalignment itself must be identified and corrected.
Objective Testing: Confirming a Misalignment Exists
One of the most important differences between Neckwise and a general chiropractic office is our use of objective testing to determine whether an upper cervical misalignment is actually present. We do not guess, and we do not adjust based on how the neck feels to the touch. We measure.
Leg Balance Test:

When the upper cervical spine is misaligned, the body compensates from the top down. The pelvis tilts, the muscles on one side of the body work harder than the other, and one leg will appear functionally shorter than the other when measured in a specific position. This is not a true anatomical leg length difference — it is a neurological imbalance produced by the body trying to compensate for the misalignment above. The leg balance test is a simple, repeatable, and remarkably sensitive screening tool. A positive finding is one of the first objective indicators that the upper cervical spine is contributing to the patient's symptoms.
Infrared Thermography:
The autonomic nervous system, which controls blood flow and skin temperature, is heavily influenced by the brainstem and upper cervical region. When the atlas is misaligned and irritating the surrounding neural tissue, the nervous system produces measurable temperature differences along the spine, particularly at the upper cervical level. We use a precision infrared thermography scan to capture these patterns. A consistent thermal asymmetry at C1 and C2 — repeated across multiple scans on different days — is strong objective evidence that the nervous system is under mechanical stress at that level. This is not a subjective interpretation. It is data.
Together, these two tests give us a clear, evidence-based answer to a simple question: is there a measurable upper cervical problem, or not? If both tests are normal, an upper cervical correction is unlikely to be the right answer for that patient, and we will say so. If both tests are abnormal and consistent with the patient's symptom pattern, we move to the next step.
CBCT 3D Imaging: Mapping the Misalignment Precisely
Once objective testing has confirmed that an upper cervical misalignment is present, the next question is exactly how the neck is out of alignment. This is where general chiropractic and precision upper cervical care diverge most clearly.
Neckwise uses CBCT (cone beam computed tomography) 3D imaging as a precision tool to visualize the upper cervical spine in three dimensions. Unlike a standard X-ray, which produces a flat, two-dimensional image, CBCT creates a true three-dimensional model of the atlas, axis, and skull. We can measure the position of each structure from multiple angles and quantify the misalignment in degrees and millimeters.

This level of precision matters because the upper cervical spine does not misalign in just one direction. The atlas can shift forward or backward, rotate to the left or right, and tilt upward or downward — often in combination. A correction that addresses one component but not the others will not resolve the underlying problem. With CBCT imaging, the doctor knows exactly which directions the atlas has shifted, and the correction can be planned with millimeter-level specificity. There is no guesswork. The plan is built from the patient's own anatomy.
The Correction: No Twisting, No Popping, No Pulling
This is often the moment a patient relaxes for the first time in the office. The Neckwise correction is not what most people picture when they hear the word chiropractic. There is no twisting of the neck. There is no cracking or popping sound. There is no forceful pulling or sudden movement of the head.
Instead, the patient lies on their side on a precisely engineered table. The doctor uses the measurements from the CBCT imaging to determine the exact angle and direction needed to guide the atlas back toward its ideal position. The correction itself is delivered through a controlled, low-force input — gentle enough that many patients are surprised it has happened at all. The intent is not to force a vertebra into place. The intent is to give the body a precise mechanical input that allows it to release the misalignment on its own terms.
Because the correction is so specific and so gentle, it is appropriate for a wide range of patients, including those who have been told they are not candidates for traditional chiropractic care. Patients with prior neck injuries, hypermobility, anxiety about neck manipulation, or simply a strong preference for a non-forceful approach often find that this style of care fits them in a way nothing else has.
What Happens After the Correction
When the upper cervical spine is restored toward its ideal position, the suboccipital muscles no longer have to hold a compensatory contraction to keep the head balanced. Over time, those muscles begin to release. As they release, the mechanical entrapment on the greater and lesser occipital nerves eases. The nerves that have been irritated for months or years are finally given the space they need.
Patients commonly report that the sharp, shocking pain at the base of the skull becomes less frequent and less intense. The scalp tenderness fades. Triggers that used to set off an episode lose their power. Sleep improves, because lying on a pillow no longer ignites the same firing pattern. The improvements often build in steps rather than all at once, which is why care is structured as a corrective program over weeks to months — long enough for the muscles, ligaments, and nervous system to adapt to the new position and for healing to consolidate.
Finding Real Relief in Sarasota
If you have been searching for an occipital neuralgia doctor in Sarasota, and especially if you have already cycled through neurologists, pain management, nerve blocks, and medication without lasting relief, the upper cervical approach offers a different starting point. It begins with objective testing to determine whether a misalignment is actually present. It uses precision 3D imaging to map exactly how the neck is out of alignment. And it delivers a correction that involves no twisting, no popping, and no pulling.
Neckwise focuses on patients who have not found answers in the conventional system, and the connection between upper cervical misalignment, suboccipital muscle tension, and occipital nerve entrapment is one of the clearest examples of why a structural and neurological perspective matters. The pain in the back of the head is real. The cause is often more specific than patients have been led to believe. And the path to relief begins with measuring, imaging, and correcting the upper cervical spine with the precision the region demands.
To learn more or schedule a consultation, contact Neckwise Sarasota. The first step is finding out whether your upper cervical spine is part of the picture — and from there, building a plan to address it at the source.



Leave a comment