
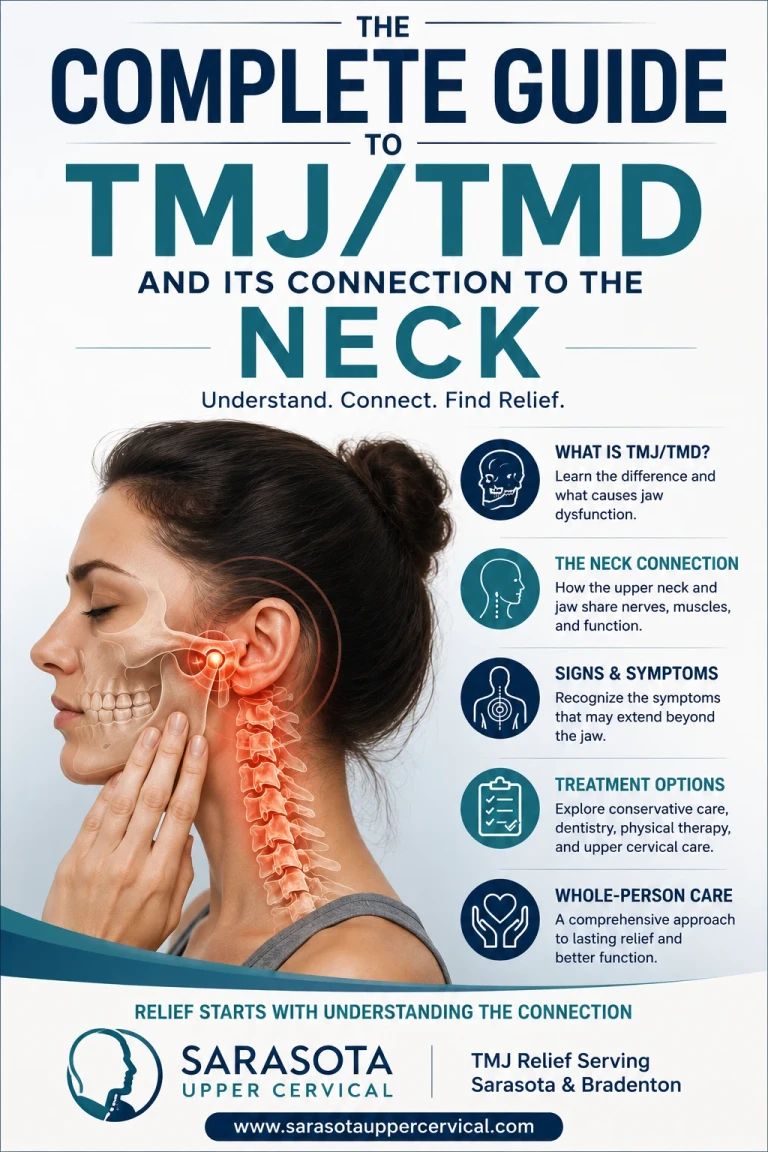
"Jaw pain rarely starts and stops at the jaw. For many people, the top of the neck is a quiet partner in the problem — and the part most often left unexamined"
Sarasota Upper Cervical · TMJ Relief Serving Sarasota - Bradenton-Lakewood Ranch - Osprey - Englewood - Venice -Parrish -Longboat Key
Schedule Your Appointment
Schedule appointmentWhat this guide covers:
1.What TMJ and TMD actually mean
2.Common symptoms
3.What drives TMD
4.The neck–jaw connection
5.Forward head posture and the jaw
6.Where upper cervical care fits
7.Who treats what: dentistry vs. the neck
8.How we approach it in Sarasota
9.FAQ
If you've been told you have "TMJ," you've probably also been told a dozen things to try, night guards, soft foods, jaw exercises, stress management. Some of it helps. But for a lot of people, the jaw symptoms keep circling back, and no one can quite explain why. One reason this happens so often is that the jaw and the upper neck are far more connected than most people realize, and the neck's role tends to go unexamined.
This guide walks through what TMJ and TMD really are, why the symptoms spread the way they do, and how the top of your neck fits into the picture, including where upper cervical care can help and, just as importantly, where it can't.
First, the terms: TMJ vs. TMD
People use "TMJ" as a catch-all, but the two terms mean different things:
TMJ is the temporomandibular joint itself — the hinge connecting your lower jaw to your skull, just in front of each ear. Everyone has two of them. Having a TMJ isn't a problem; it's anatomy.
TMD stands for temporomandibular disorder — the umbrella term for pain and dysfunction involving that joint, the muscles that move the jaw, and the surrounding structures.
So when someone says "I have TMJ," what they usually mean is "I have TMD." It matters here because TMD is rarely a single, isolated joint problem — it's a condition with several moving parts, and the neck is one of them.
Common symptoms of TMD
TMD symptoms often extend well beyond the jaw, which is part of why it gets misread. People commonly experience:
Jaw pain or soreness, often near the ear
Clicking, popping, or grating with movement
Difficulty or discomfort opening wide
The jaw locking or catching
Headaches at the temple or behind the eye
Ear fullness, pressure, or ringing
Facial muscle fatigue or tension
Neck and upper-shoulder tightness
Notice how many of those aren't jaw symptoms at all — headaches, ear pressure, neck tightness. That spread is a clue to the underlying wiring, which we'll get to in a moment.
What drives TMD
TMD is what clinicians call multifactorial — it usually has more than one contributor. Common ones include:
Muscle overuse and clenching or grinding (often stress-related, often during sleep).
Bite and joint mechanics — how the teeth meet and how the joint and its disc move.
Trauma , a blow to the jaw, or a whiplash-type injury that affects both the jaw and the neck at once.
Posture, particularly sustained forward head posture, which changes how the jaw rests and works.
Cervical (neck) dysfunction irritation and altered mechanics in the upper neck that feed into the same nerve pathways as the jaw.
That last two are where the neck enters the story and they're the parts most often skipped when TMD is treated as a jaw-only problem.
The neck–jaw connection: why they share symptoms
Here's the anatomy that ties it together. The muscles and joint of your jaw are supplied by the trigeminal nerve. The top of your neck, the C1, C2, and C3 levels, sends its own sensory signals into the brainstem. And these two streams don't stay separate: they converge at a shared junction called the trigeminocervical complex, where signals from the jaw and signals from the upper neck can feed into the very same nerve cells.
This convergence is the reason TMD symptoms travel the way they do. It's why jaw dysfunction can be felt as a headache or ear pressure, and — running the other direction — why irritation in the upper neck can show up as jaw and facial symptoms. The jaw and the upper neck are, neurologically, part of the same neighborhood. Treat one and ignore the other, and you may only be addressing half the system.
In plain terms
Your jaw and the top of your neck report to the same switchboard in your brainstem. When either one is sending irritated signals, the other region can feel it. That's why "jaw" problems so often come bundled with neck tightness, headaches, and ear pressure — and why leaving the neck out of the picture can leave the loop unbroken.
Forward head posture and the jaw
There's also a purely mechanical link, and it's one almost everyone can relate to now: forward head posture — the "tech neck" of hours spent over phones and screens. When the head drifts forward of the shoulders, also known as military neck, the muscles at the base of the skull and along the neck work overtime, and the resting position of the lower jaw shifts. Research has repeatedly found forward head posture more often in people with jaw-joint pain than in those without it.
The takeaway isn't that posture is the whole story, it's that the head, neck, and jaw operate as one connected unit. Where the head sits on the neck changes how the jaw hangs and functions. So a jaw that keeps flaring up despite good dental care may be responding to what's happening one level down, at the top of the neck.
Where upper cervical care fits
Upper cervical chiropractic focuses on the alignment and movement of the top two vertebrae of the neck — the atlas and axis — which sit directly beneath the skull and anchor the head's position. Because those upper cervical structures share nerve pathways with the jaw and influence head posture, addressing irritation and altered mechanics there can be a meaningful part of the picture for people whose TMD has a cervical component.
What that looks like in practice: gentle, precise corrections to restore balanced alignment at the top of the neck — not the forceful twisting people often associate with general chiropractic. The aim is to reduce the cervical irritation feeding into the shared trigeminocervical pathways and to support a more balanced head-on-neck posture.
It's important to be exact about scope here:
Related article
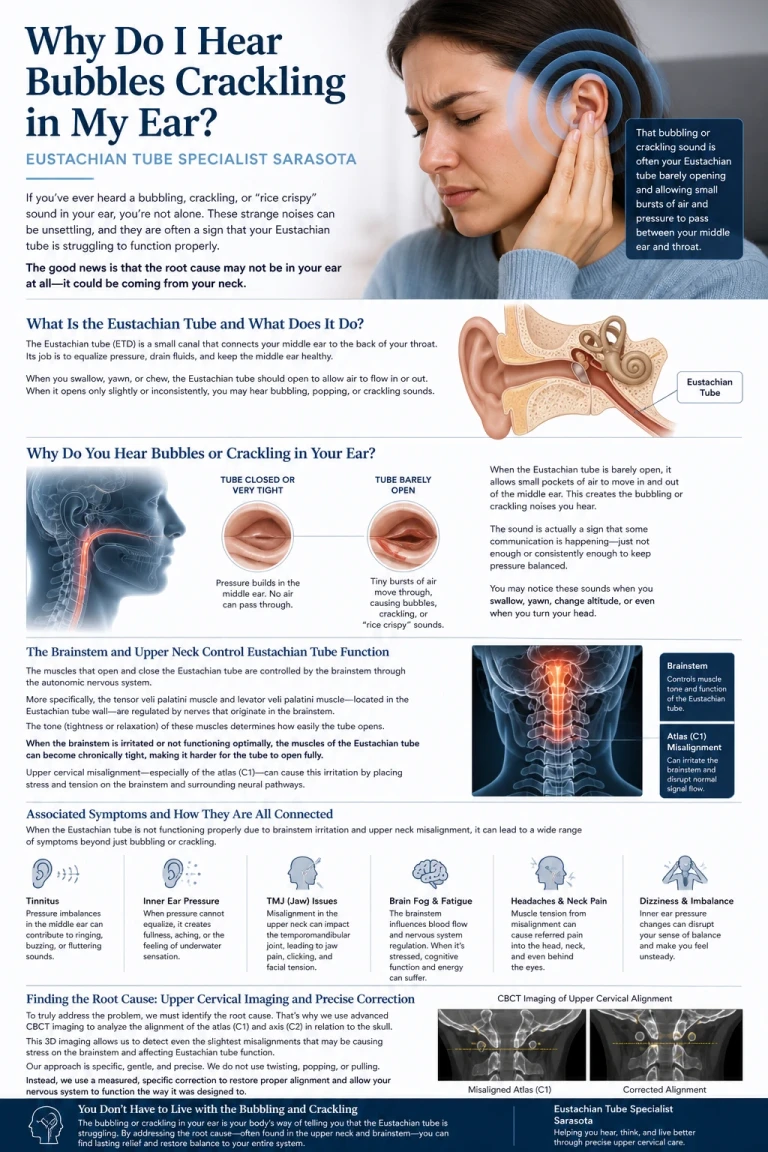
Why Do I Hear Bubbles or Crackling in My Ear? | Eustachian Tube Specialist Sarasota
May 04, 2026Upper cervical care addresses the cervical (neck) contribution to TMJ symptoms.
It does not treat the jaw joint itself, correct your bite, fit splints or night guards, or perform any dental work.
It does not cure TMD, and it isn't a standalone fix for a problem that's truly joint- or bite-driven.
For many people, the best results come from the neck and the jaw being addressed by the right providers working in their own lanes. Individual results vary, and an examination is the only way to know whether your upper neck is part of your particular case.
Who treats what
TMD is genuinely a team condition. Knowing who handles what saves you time and frustration:
Dentists and oral-medicine / TMJ specialists own the joint itself, the bite, the disc, splint and night-guard therapy, and any dental causes. If your TMD is bite- or joint-driven, this is the front line.
Upper cervical chiropractic focuses on the neck's contribution — the upper cervical alignment, mechanics, and posture that share nerve pathways with the jaw.
Physical therapists often address jaw and neck muscles, mobility, and posture through manual therapy and exercise.
Your physician for medical causes, pain management, and ruling out other conditions.
None of these replaces the others. The point of understanding the neck connection isn't to send everyone to a chiropractor — it's to make sure the neck doesn't get left out when it's part of the problem.
How we approach TMJ-related neck care in Sarasota
At Sarasota Upper Cervical, the first step is always evaluation, not treatment. We take a thorough history — including any jaw or neck trauma, whiplash, or longstanding posture patterns — and examine how the top of your neck is aligning and moving. If we find an upper cervical pattern that fits your jaw and head symptoms, we'll explain it in plain language and discuss whether gentle upper cervical care is appropriate for you.
We also believe in staying in our lane. If your TMD looks primarily joint- or bite-driven, we'll say so and encourage you to work with a dentist or TMJ specialist, and we're glad to be one part of a coordinated approach when the neck is involved. The goal is simply to make sure the cervical piece of your TMJ puzzle isn't the piece everyone forgot to check.
Is your neck part of your jaw problem?
If your TMJ symptoms keep returning and no one has examined your upper neck, an upper cervical evaluation can help answer whether the neck is part of the picture.
Request a Consultation-Call 941-259-1891
Frequently asked questions
1.Can a neck problem really cause jaw pain?
The jaw muscles and the upper neck share nerve pathways through a brainstem junction called the trigeminocervical complex, where their signals can converge on the same nerve cells. Because of this overlap, irritation in the upper neck can contribute to jaw and facial symptoms, and jaw dysfunction can be felt as neck tightness or headache. This is why the neck is increasingly considered part of the TMD picture.
2.Does upper cervical care treat TMJ?
Upper cervical care addresses the cervical, or neck, contribution to TMJ symptoms — the upper cervical alignment, mechanics, and posture that share nerve pathways with the jaw. It does not treat the jaw joint itself, correct the bite, or fit splints, and it does not cure TMD. For joint- or bite-driven TMD, a dentist or TMJ specialist is the right provider.
Related article

Upper Cervical Chiropractor Sarasota, Bradenton, Venice and Tampa Bay Area
Nov 15, 20213.Should I see a dentist or a chiropractor for TMJ?
It depends on what's driving your TMD, and often the answer is both. Dentists and TMJ specialists handle the joint, bite, disc, and splint therapy. Upper cervical chiropractic focuses on the neck's contribution. If your symptoms keep returning despite dental care, or come bundled with neck tightness and headaches, having the upper neck evaluated can help identify whether that piece has been missed.
4.Why do I have ear pressure and headaches with my jaw pain?
Because the jaw, the area around the ear, and the head all share sensory pathways through the trigeminal nerve and the trigeminocervical complex. Symptoms generated at the jaw or upper neck can be felt as ear fullness, ringing, or headache even when the ear itself is healthy. Persistent ear symptoms should also be checked by a physician.
5.How does forward head posture affect the jaw?
When the head sits forward of the shoulders, the muscles at the base of the skull and neck work harder and the resting position of the lower jaw shifts, which can increase strain on the jaw muscles and joint. Studies have found forward head posture more often in people with jaw-joint pain, which is one reason posture and the upper neck are part of a complete TMD picture.
6.Where can I get help with TMJ and neck pain in Sarasota?
Sarasota Upper Cervical serves the Sarasota and Bradenton area and focuses on the upper cervical contribution to TMJ-related symptoms. You can request a consultation to find out whether your upper neck is part of your jaw problem, and we'll coordinate with dental or other providers when that's the right path.
References:
Calixtre LB, et al. Effectiveness of physiotherapy in the treatment of temporomandibular disorders and the relationship with the cervical spine.
La Touche R, et al. Cervical spine influence on the temporomandibular system: trigeminocervical convergence.
Studies on forward head posture and temporomandibular disorders (cephalometric analyses). NCBI / PMC.
Bartsch T, Goadsby PJ. Anatomy and physiology of pain referral in the trigeminocervical complex.
National Institute of Dental and Craniofacial Research (NIDCR). TMD overview.
This guide is for general educational purposes only and does not constitute medical or dental advice, diagnosis, or treatment, and it does not establish a doctor–patient relationship. TMD is a multifactorial condition that requires professional evaluation to diagnose and is often best managed by a coordinated team that may include a dentist or TMJ specialist, physician, physical therapist, and chiropractor. Results of upper cervical care vary from person to person, and no specific outcome is promised or guaranteed. If you have a locked jaw, significant swelling, signs of infection, or jaw pain following an injury, seek dental or medical care promptly. Always consult a qualified health provider with questions about a medical or dental condition.



Leave a comment