

A complete guide to how the alignment of C1 and C2 influences nearly every common headache pattern — and how precise structural correction can change the trajectory.
Why Headaches Deserve a Structural Evaluation
Schedule Your Appointment
Schedule appointment
Headaches are among the most common reasons adults seek medical care, and also among the most frustrating to manage. The conventional approach focuses almost entirely on symptom suppression — medication to reduce pain when it occurs, with comparatively little attention to why the headache is happening in the first place. For patients who experience headaches frequently or chronically, this can become a long cycle that does not resolve the underlying problem.
At Sarasota Upper Cervical Chiropractic, we routinely meet patients who have spent years on that path. They have seen neurologists, headache specialists, ENTs, and primary care providers. They have undergone MRIs, CT scans, and blood work. They have tried over-the-counter analgesics, triptans, beta blockers, anticonvulsants, antidepressants, and the newer CGRP inhibitors. Some treatments helped a little. Most did not change the underlying pattern. The headaches kept coming.
There is a structural factor that gets overlooked in this workup, and it sits at the very top of the spine. The relationship between the skull, the atlas (C1), and the axis (C2) influences nearly every major headache type through pathways that mainstream headache medicine does not routinely evaluate. This article walks through the science, the conditions, and the precise approach we use to identify and address the upper cervical contribution to headache when it is present.
Whether you are dealing with tension-type headaches, migraines, cluster headaches, occipital neuralgia, post-concussion headaches, or any other chronic head pain — the question of whether your upper cervical spine is part of the picture deserves an honest answer.
If headaches have been part of your life longer than they should be, a structural evaluation may be the missing step.
Call 941-259-1891 to schedule a free consultation.
The Anatomy Behind the Connection
Understanding the connection between the upper cervical spine and headaches requires a brief tour of the anatomy at the top of the neck — a region called the craniocervical junction.
The bones
Three bones define the craniocervical junction. The occiput, at the base of the skull. The atlas (C1), the first cervical vertebra, which sits directly underneath the skull and supports its full weight. The axis (C2), the second cervical vertebra, which provides the rotational pivot for the head. Unlike most vertebrae, the atlas has no central body — it is essentially a ring of bone cradling the skull. The axis has a unique vertical bony peg, the odontoid process, that rises up into the atlas. The atlas rotates around this peg, allowing the head to turn left and right.
The nerves
Three pairs of cervical nerves exit the spine in this region — C1, C2, and C3. These nerves supply the back of the head, the scalp, the temples, the forehead, the upper part of the neck, and parts of the face. The greater occipital nerve, a branch of C2, is one of the most clinically important nerves in headache medicine — irritation of this nerve is the direct cause of occipital neuralgia and contributes to many other headache patterns through referred pain.
The trigeminocervical complex
This is the anatomical key to understanding the headache-neck connection. The trigeminocervical complex is a region of the brainstem where sensory fibers from the upper cervical nerves (C1, C2, C3) converge and share neurons with sensory fibers from the trigeminal nerve — the nerve that carries pain signals from the face, forehead, eyes, and front of the head. Because these inputs share neurons in the brainstem, irritation arising from the upper cervical spine can be felt as pain in areas supplied by the trigeminal nerve — the forehead, the eye, the temple, the face. The brain cannot always distinguish which input the pain originated from.
This convergence is the reason a patient with an upper cervical structural problem can experience pain that feels exactly like a migraine in the forehead and behind the eye, with no problem in the forehead or eye at all. The signal originated in the neck. The brain referred it forward.
The vascular and fluid systems
Inside the small corridor formed by the foramen magnum, the atlas, and the axis, several critical structures pass simultaneously. The vertebral arteries supply blood to the back of the brain. The internal jugular veins and surrounding venous plexuses drain blood from the cranial vault. The cerebrospinal fluid pathways circulate fluid between the brain and the spinal cord. And the brainstem itself sits inside this region. The geometry of this corridor depends on the alignment of the bones around it. When alignment shifts, the mechanical environment changes for every structure inside.
How Upper Cervical Misalignment Drives Headache Pain
Upper cervical misalignment can drive headache pain through several distinct but overlapping mechanisms. Different headache types involve different combinations of these mechanisms, but they share the same underlying anatomical reality.
Mechanical irritation of the upper cervical nerves
When the atlas, axis, or occiput sit slightly off neutral, the surrounding muscles tighten and the joint capsules become mechanically stressed. The C1, C2, and C3 nerves — which exit the spine in this region — can be irritated by the altered mechanical environment. The result is pain in the territory those nerves supply: the back of the head, the temples, the forehead, the area behind the eye.
Suboccipital muscle tension and trigger points
The deep suboccipital muscles ,the rectus capitis posterior major and minor, and the obliquus capitis superior and inferior — sit at the base of the skull and respond to upper cervical misalignment with chronic tightness. These muscles develop trigger points that refer pain forward into the head, producing the classic pattern of tension-type and cervicogenic headache. Anatomical research has documented direct connective tissue bridges between the rectus capitis posterior minor muscle and the dura mater — the membrane covering the brain. Tension in this muscle can transmit mechanical force directly to the pain-sensitive dura, contributing to headache pain (Hack et al., 1995). This is referred to as the myodural bridge.
Related article
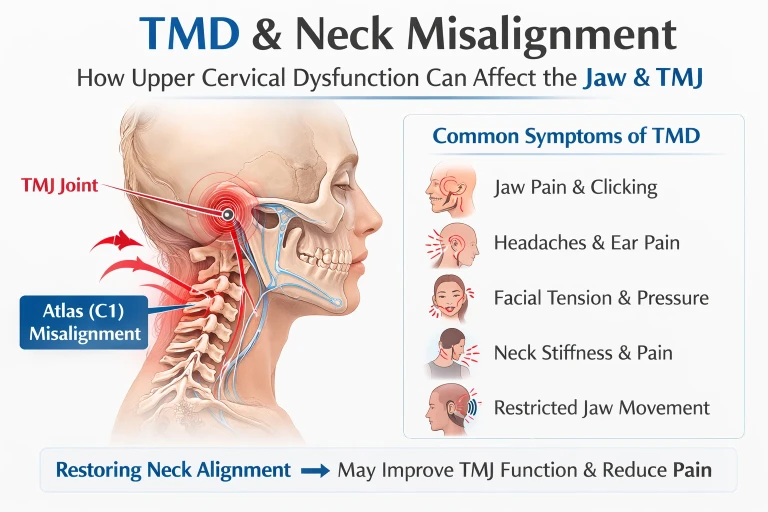
Lakewood Ranch TMD Specialist | Neck & Jaw Connection | Holistic TMD Relief
Mar 12, 2026Trigeminocervical convergence
Because upper cervical sensory input and trigeminal sensory input share neurons in the brainstem, irritation arising in the upper cervical spine can be perceived as pain in the face, forehead, and eye. This is the mechanism that makes cervicogenic headache mimic migraine and tension headache in its presentation, and it is one of the reasons headache diagnosis is so frequently difficult.
Vertebral artery and posterior circulation effects
The vertebral arteries pass through the transverse foramina of the upper cervical vertebrae. Misalignment at C1 or C2 can alter the mechanical environment of these arteries, potentially affecting flow to the brainstem and posterior brain. Reduced posterior circulation has been implicated in some migraine subtypes, particularly migraine with aura, where transient blood flow changes appear to play a role.
Brainstem irritation
The brainstem itself sits inside the corridor formed by the occiput, atlas, and axis. Mechanical irritation in this region can affect the trigeminal nucleus and the periaqueductal gray — both of which are central to migraine pathophysiology. This is a less direct but increasingly recognized mechanism by which upper cervical structural problems can influence central headache networks.
The Choke Point Theory: Flanagan's Hydrodynamic Framework
In 2015, chiropractic neurologist Michael F. Flanagan published a peer-reviewed review article in Neurology Research International titled "The Role of the Craniocervical Junction in Craniospinal Hydrodynamics and Neurodegenerative Conditions" (Flanagan, 2015). The paper described the craniocervical junction as a potential choke point for craniospinal hydrodynamics — a region where misalignment can compromise blood flow, venous drainage, and cerebrospinal fluid circulation simultaneously. The framework has direct implications for understanding chronic headache.
The blood flow problem
The vertebral arteries supply the brainstem, cerebellum, and parts of the posterior brain. When craniocervical alignment is altered, the mechanical environment of these arteries changes. Reduced blood flow to brainstem structures — including the trigeminal nucleus, the periaqueductal gray, and the locus coeruleus, all of which are involved in headache generation — can lower the threshold at which headaches occur. Patients with this kind of structural compromise often describe headaches that come on with prolonged neck position, with stress, or with anything else that further reduces an already compromised flow.
The venous drainage problem
The venous plexuses around the upper cervical spine drain blood from the cranial vault. When craniocervical alignment is altered, these venous pathways can become congested. The downstream consequence is increased intracranial pressure — a condition that produces a characteristic pattern of headache: worse in the morning, worse when lying down, worse when bending over, worse with anything that increases head pressure. Many patients with chronic daily headache who have been worked up extensively without a clear diagnosis have this kind of subtle venous drainage problem.
The cerebrospinal fluid problem
Cerebrospinal fluid circulates between the cranial vault and the spinal canal through the corridor at the craniocervical junction. When this corridor is geometrically compromised, CSF flow can be impeded. The downstream effects include altered pressure dynamics in the brain. CSF flow disruption has been implicated in headache patterns associated with conditions like Chiari malformation, but milder versions of the same mechanism can occur in patients with simple upper cervical misalignment.
The brainstem irritation problem
The brainstem itself sits inside this corridor. Mechanical irritation of the brainstem and its surrounding structures can produce both afferent disruption (distorted sensory signals coming up from the body) and efferent disruption (altered motor and autonomic signals going down). For headaches, this matters because the autonomic features of many headache types — nausea, light sensitivity, sound sensitivity, sweating, tearing — are produced by brainstem networks. Mechanical irritation of those networks can lower the threshold for those features to appear.
The craniocervical junction is a potential choke point for blood and CSF flow between the cranial vault and spinal canal that can cause faulty craniospinal hydrodynamics. (Flanagan, 2015)
If you have been told nothing is wrong but you keep getting headaches, the choke point may be where the answer lives.
Call 941-259-1891 for a free consultation.
The Different Types of Headaches
Headaches are not one condition. They are a category that includes more than 200 distinct types, each with its own pattern, mechanism, and management approach. The International Classification of Headache Disorders, now in its third edition, organizes them into primary headaches (where the headache itself is the disease) and secondary headaches (where the headache is a symptom of another condition). The sections below cover the headache types we most commonly see in clinical practice, with an emphasis on how each one relates to upper cervical structural function.
Tension-Type Headache
Tension-type headache is the most common headache disorder, affecting most adults at some point in their lives. The pattern is characteristic: a pressing or tightening pain, usually on both sides of the head, often described as a band around the head or a vise grip. The pain is mild to moderate, does not typically pulse, and is not worsened by routine physical activity. Tension-type headaches can be episodic — occurring a few times a month — or chronic, occurring more than 15 days per month for at least three months.
The cervical contribution to tension-type headache is significant. The deep suboccipital muscles are the source of much of the pain in tension-type headache, and these muscles respond to upper cervical misalignment with chronic tightness. Patients with tension-type headache almost universally have palpable tightness in the suboccipital region, with trigger points that reproduce the headache pattern when pressed. Correcting the underlying upper cervical alignment can reduce the chronic muscle tension that drives the recurrent headaches.
Cervicogenic Headache
Cervicogenic headache is the headache type most directly attributable to the cervical spine. It is defined by pain originating in the neck and referred to the head, typically starting at the base of the skull or in the neck and radiating forward to the back of the head, the temple, the forehead, or behind one eye. The pain is usually one-sided, steady rather than throbbing, and provoked by neck movement or sustained neck positions. Patients often describe it as a deep ache rather than a sharp pain.
The mechanism of cervicogenic headache is the trigeminocervical convergence described earlier. Sensory fibers from the upper cervical nerves and the trigeminal nerve share neurons in the brainstem, so irritation arising in the upper cervical spine is perceived as pain in the head. The diagnostic criteria for cervicogenic headache, established by the International Headache Society, specifically require evidence that the cervical spine is the source — typically demonstrated by reproduction of the pain with cervical maneuvers, or by relief of the pain with cervical intervention (Bogduk & Govind, 2009).
Cervicogenic headache is one of the conditions where upper cervical chiropractic has the strongest theoretical and clinical alignment. The condition is, by definition, a cervical problem. Addressing the cervical source structurally is the direct path to addressing the headache.
Migraine Headache
Migraine is a neurological disorder characterized by recurrent attacks of moderate-to-severe headache, typically one-sided and throbbing, usually accompanied by nausea, sensitivity to light, sensitivity to sound, and worsening with physical activity. Migraine attacks last 4 to 72 hours and can be accompanied by aura — visual disturbances, sensory changes, or speech difficulty — in roughly a third of patients. Migraine affects approximately 12 percent of adults globally and is one of the leading causes of disability in working-age adults.
The relationship between migraine and the cervical spine is more complex than for tension-type or cervicogenic headache, but it is real. Several mechanisms are involved.
First, the trigeminocervical complex sits at the center of migraine pathophysiology. The brainstem region where cervical and trigeminal inputs converge is the same region where migraine attacks are generated. Chronic irritation from upper cervical sources can lower the threshold at which migraine attacks occur — a phenomenon described in the headache literature as central sensitization.
Second, neck pain is extremely common in migraine. Research has demonstrated that neck pain is more prevalent in migraine patients than nausea, and a substantial percentage of migraine attacks begin with neck symptoms (Calhoun et al., 2010). For these patients, the cervical component is not incidental — it is part of the attack itself.
Third, patients with chronic migraine often have measurable upper cervical dysfunction. A 2017 study in Cephalalgia demonstrated that patients with migraine showed significantly different cervical musculoskeletal findings than healthy controls, including reduced cervical range of motion and increased upper cervical joint dysfunction (Luedtke et al., 2017).
Addressing the cervical contribution to migraine does not replace migraine-specific medical management. For most patients, it complements it. The goal of upper cervical care in migraine is to reduce one of the inputs that lowers the attack threshold — allowing migraine medications to work better and the underlying central sensitization to gradually settle.
Cluster Headache
Cluster headache is one of the most painful conditions in medicine. Attacks involve severe, strictly one-sided pain centered around the eye, accompanied by autonomic features on the same side: tearing, redness of the eye, nasal congestion, sweating, drooping of the eyelid. Attacks last 15 to 180 minutes and occur in clusters — periods of frequent attacks separated by remission. The condition is much less common than migraine, affecting roughly 0.1 percent of adults, and predominantly affects men.
The mechanism of cluster headache involves the hypothalamus and the trigeminal-autonomic reflex — a connection between the trigeminal nerve and the autonomic nervous system in the brainstem. Both of these are influenced by the mechanical environment at the craniocervical junction. While cluster headache is primarily a central nervous system disorder, the brainstem irritation produced by upper cervical misalignment can affect the same structures involved in cluster attack generation. Some patients with cluster headache who have an identifiable cervical structural component report improvement in attack frequency or severity when the structural component is addressed.
Occipital Neuralgia
Occipital neuralgia is a distinct headache disorder caused by irritation of the greater or lesser occipital nerves — the nerves that supply the back of the head. The pain is characteristic: sharp, shooting, or electrical-feeling, starting at the base of the skull and radiating up the back of the head. Patients often describe tenderness over the back of the head and scalp, and the pain can be triggered by pressing on the affected area.
The greater occipital nerve is a branch of the C2 nerve root, which exits the spine between the atlas and the axis. Upper cervical misalignment at C1-C2 can directly irritate this nerve through mechanical compression, muscle entrapment, or altered joint mechanics. For occipital neuralgia, the relationship between upper cervical structure and the condition is anatomically direct — and structural correction can address the source of the nerve irritation rather than just numbing the nerve with injections.
Post-Traumatic and Post-Concussion Headache
Post-traumatic headache is one of the most common symptoms following concussion or head injury. The headache pattern is variable — it can resemble tension-type, migraine, or cervicogenic headache — but it shares a common feature: it began after a specific traumatic event. Persistent post-traumatic headache is defined as headache that continues for more than three months after the initial injury.
The cervical contribution to post-traumatic headache is significant and frequently missed. Concussion and head injury rarely affect the head in isolation — the cervical spine is almost always involved in the same mechanical event. Whiplash injuries place the upper cervical spine under extreme load. Joint capsules can tear. Ligaments can stretch. The atlas and axis can be displaced from their neutral position. The resulting structural problem can persist long after the concussion symptoms have resolved, driving headaches that do not respond to standard concussion management.
For patients with persistent post-traumatic or post-concussion headache, a structural evaluation of the upper cervical spine deserves serious consideration. The injury that caused the concussion almost certainly affected the upper cervical region, and that injury may be why the headaches have not resolved.
Sinus Headache
Sinus headache is one of the most over-diagnosed and under-diagnosed conditions in headache medicine. Many patients diagnosed with chronic sinus headache actually have migraine — the symptoms overlap considerably, and pain in the forehead and cheeks can occur in both. True sinus headache is associated with active sinus infection, including purulent nasal discharge and fever, and resolves when the infection clears.
Where the cervical spine becomes relevant is in patients who have been diagnosed with chronic sinus headache without evidence of active sinusitis. The trigeminocervical complex refers cervical pain into the face, forehead, and area around the eyes — exactly the locations patients describe as sinus pain. Patients who have been on years of sinus medications without relief, and who have unremarkable sinus imaging, frequently turn out to have a cervical contribution to their facial pain. A structural evaluation of the upper cervical spine is reasonable in these cases.
Hormonal Headache
Hormonal headache refers to headaches that occur in relationship to the menstrual cycle, hormonal contraception, perimenopause, or pregnancy. Estrogen fluctuations, particularly the rapid drop in estrogen before menstruation, are a recognized migraine trigger. Many women with chronic headaches experience an exacerbation in the days leading up to their period.
While hormonal headaches are clearly driven by hormonal physiology, the cervical contribution interacts with that physiology. A woman with chronic upper cervical dysfunction and a low headache threshold will be more susceptible to hormonal triggers than a woman with a high threshold. Addressing the cervical component does not change the hormonal pattern, but it can raise the threshold at which hormonal fluctuations produce a headache. Many patients describe that their hormonal headaches do not stop entirely but become less severe and less disabling when the cervical component is addressed.
Hypnic, Exertional, and Cough Headaches
Several less common headache types deserve mention because they have specific connections to craniocervical structure.
Hypnic headache is a rare condition occurring exclusively during sleep, typically waking the patient at a consistent time each night. It primarily affects older adults. The mechanism is not fully understood, but the cervical position during sleep — particularly in patients with upper cervical structural issues — can contribute. Some patients with hypnic headache report improvement after pillow and sleep position changes that reduce upper cervical loading at night.
Exertional headache occurs with physical exertion — running, lifting, sexual activity. While most cases are benign, exertional headache can also be a marker of structural problems in the head or neck, including craniocervical instability or vertebral artery compromise. Imaging is usually warranted before assuming the cause is benign. Where upper cervical dysfunction is identified, addressing it may reduce exertional symptoms.
Cough headache is triggered by coughing, sneezing, straining, or laughing. Primary cough headache is benign, but the same maneuvers that trigger cough headache also briefly increase intracranial pressure and stress the craniocervical junction. Patients with underlying upper cervical structural problems may be more susceptible to this pattern.
Medication Overuse Headache
Medication overuse headache is a secondary headache disorder caused by the very medications used to treat other headaches. When a patient with a primary headache disorder uses pain medications, triptans, or combination analgesics on more than 10-15 days per month for several months, the medication itself can become a driver of headaches — a daily or near-daily headache that does not respond to further medication and only improves when the offending medication is withdrawn.
Medication overuse headache is one of the strongest arguments for finding and addressing the structural cause of the original headache pattern. Patients in the medication overuse cycle did not get there because their original headache was minor — they got there because their original headache was severe and frequent enough to require regular medication. If a structural factor is driving that frequency, identifying and addressing it can be the path out of the cycle. Upper cervical evaluation belongs in the workup of patients who are using headache medications more often than they should.
How We Identify the Structural Cause
At Sarasota Upper Cervical Chiropractic, we use a structured assessment process to determine whether the upper cervical spine is contributing to a patient's headache pattern. The process has three layers.
The history conversation
Most of what we need to know surfaces in the first conversation. We ask about the headache pattern — location, character, duration, frequency, associated symptoms. We ask about triggers, including whether neck position or movement is involved. We ask about the timeline, including any injuries or events that preceded the headache onset. And we ask carefully about past trauma — including events that may not have seemed connected at the time. A whiplash from college. A fall off a bicycle in childhood. A sports concussion. A difficult birth. These often turn out to be the precipitating event for headaches that developed years later.
The examination
A focused physical examination assesses cervical range of motion, the mobility of the upper cervical segments, the tone and tenderness of the suboccipital musculature, and any reproducible relationship between cervical positions or pressure and the headache pattern. Findings consistent with upper cervical involvement include reduced upper cervical range of motion, palpable joint restriction, suboccipital tension, and reproduction of headache symptoms with specific cervical maneuvers.
The structural measurement
Where upper cervical chiropractic differs most clearly from general chiropractic and from medical imaging is in the precision of the structural measurement we use. This is covered in the next section.
CBCT Imaging and Objective Testing
The assessment tools we use at our practice are what separate precise upper cervical care from general chiropractic adjustment. Each tool answers a specific question about your structural anatomy and current alignment status.
Cone beam computed tomography (CBCT)
CBCT is a low-dose three-dimensional imaging technology that produces a true 3D reconstruction of the upper cervical anatomy. The upper cervical region is geometrically complex, and misalignments can occur in multiple planes simultaneously — rotation, lateral tilt, anterior-posterior translation. Standard two-dimensional X-rays of this region are subject to projectional distortion and cannot reliably capture this three-dimensional information.
CBCT eliminates that limitation. From a CBCT scan, we can measure the precise angle and direction of misalignment between the occiput, atlas, and axis to within fractions of a degree. Every patient's anatomy is unique. The exact correction that one patient needs is different from what another patient needs, and CBCT is what allows us to calculate the specific correction each individual requires. In our practice, CBCT is used as a measurement tool, not a diagnostic tool — the goal is precision in correction, not pathology identification.
Related article
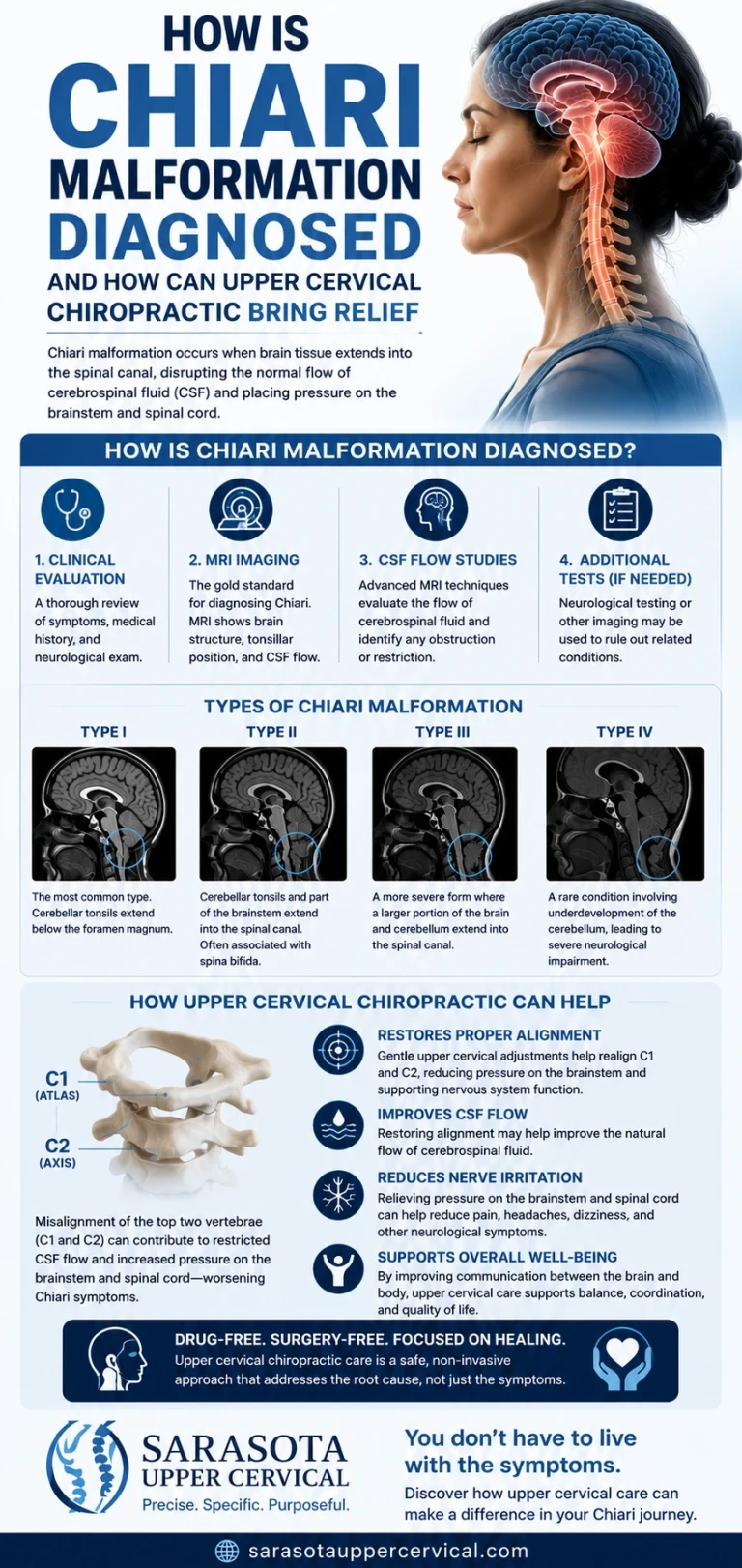
How is chiari malformation diagnosed and how can upper cervical chiropractic bring relief
Jul 12, 2026Leg length analysis
Leg length analysis is a postural test in which we examine the patient for asymmetry in functional leg length. Upper cervical misalignment produces measurable functional leg length inequality through the compensatory postural changes it triggers below the neck — the body adjusts to a head that is sitting slightly off-center, and that adjustment shows up in the legs. When the upper cervical correction is holding, leg length normalizes. When the correction has shifted, leg length asymmetry returns. The test takes seconds and provides an objective check before any decision to adjust is made.
Paraspinal infrared thermography
Paraspinal infrared thermography is a non-invasive scan that measures heat patterns along the cervical spine. Asymmetric autonomic nervous system activity, driven by upper cervical irritation, produces measurable temperature differentials along the neck. A consistent thermal pattern indicates the spine is out of alignment. A neutral pattern indicates the correction is holding.
The decision the testing makes
If leg length analysis and thermography both indicate the upper cervical spine is in alignment, we do not adjust. The body is doing the work. If the tests indicate the spine has shifted, we deliver a precise correction along the vector calculated from the CBCT analysis. This is the opposite of routine, schedule-based adjusting. The principle is restraint guided by data. We adjust when adjusting is warranted, and we leave the body alone when it is not.
For patients with chronic headache — whose nervous systems are typically sensitized from years of pain — this matters significantly. Unnecessary manipulation aggravates a sensitive system. The precision-and-restraint approach respects the sensitivity of the nervous system you bring to the office.
We do not adjust because it is Tuesday. We adjust because the measurements indicate an adjustment is needed. If they do not, we do not. The body is doing the work, and our job is to support that — not to interfere with it.
If you want a structural evaluation that uses 3D imaging and objective testing — not guesswork — Sarasota Upper Cervical Chiropractic is the place to start.
Call 941-259-1891 for a free consultation.
What Happens After a Precise Correction
Upper cervical correction does not eliminate headaches by itself. It removes the structural obstacle that has been contributing to the headache pattern, and allows the body to begin healing the systems that have been compensating. Once the correction is established and the joint is in proper position, a sequence of changes begins.
The joint capsule is no longer held in an abnormal position. The mechanical strain on surrounding ligaments and the suboccipital muscles is reduced. The chronic muscle tension that has been pulling on the dura begins to release. The mechanoreceptors in the joint capsules begin firing in a more accurate pattern. The trigeminocervical complex in the brainstem receives less abnormal input. The venous drainage and CSF flow through the craniocervical corridor improves as the mechanical environment normalizes.
Patients typically describe the improvement as gradual rather than instantaneous. The intensity of headaches tends to decrease first. The frequency drops next. Patients often realize at some point that they used to have a headache every day or every week, and now they have had one in the last month — and it was milder than usual. Over a longer time frame, the central sensitization that has been amplifying every headache trigger begins to settle, and the threshold for headache attacks rises.
Care at our practice generally proceeds in two phases. The first is a corrective phase, during which the alignment is established and the body is given time to stabilize. Visit frequency is higher early on and tapers as the correction begins to hold. The second is a maintenance phase, during which we monitor the alignment at longer intervals and adjust only when objective testing indicates a shift. Most patients settle into monthly or less-frequent maintenance over time.
When to Schedule an Evaluation
An upper cervical evaluation is worth scheduling when any of the following are true:
You have chronic or recurrent headaches that have not been adequately controlled by other approaches. You have a history of whiplash, concussion, sports injury, or other neck trauma — even years or decades ago. Your headaches are accompanied by neck pain, neck stiffness, or symptoms that radiate from the back of the head forward. Specific neck positions or movements reliably provoke your headaches. You have been diagnosed with a primary headache disorder but have not had lasting relief from standard treatment. You are using headache medications more than 10-15 days per month. You experience associated symptoms like dizziness, brain fog, fatigue, or visual disturbance alongside your headaches. You have completed extensive medical testing and been told nothing is wrong despite ongoing headaches.
None of these alone is diagnostic. Several of them together are a strong signal that the upper cervical spine deserves to be evaluated as part of your workup. For most patients with chronic headache, this evaluation has not yet been done with the precision needed to identify the structural component.
Schedule a free consultation to find out whether the upper cervical spine is part of your headache picture.
Frequently Asked Questions
How is upper cervical chiropractic different from regular chiropractic?
Upper cervical chiropractic focuses exclusively on the precise structural relationship between the skull, atlas (C1), and axis (C2). We use 3D CBCT imaging to measure misalignment with high precision, objective testing (leg length analysis and thermography) before every adjustment to determine whether correction is needed, and specific low-force corrections delivered along a calculated vector. There is no twisting, no popping, no full-spine manipulation. The principle is precision over volume — fewer, better-targeted adjustments rather than more frequent, generalized ones.
Is upper cervical correction safe for patients with chronic headaches?
The low-force, precision nature of upper cervical correction makes it particularly well suited for patients with sensitized nervous systems, which is common in chronic headache disorders. Because we only adjust when objective testing indicates a misalignment is present, patients are not subjected to unnecessary manipulation. The corrections themselves are small and specific.
How long does it take to see results?
Improvement is typically gradual rather than instantaneous. Some patients notice changes in headache intensity within the first few weeks. Others require longer as the underlying central sensitization settles. Outcomes vary by individual, by the chronicity of the underlying problem, and by overall health factors. We discuss realistic expectations with every patient based on their specific case.
Will I need to stop my headache medications?
No. Upper cervical care does not require stopping medical management of your headache disorder, and we do not advise patients to stop or change their medications. We work alongside whatever care you are receiving from your neurologist, headache specialist, or primary care physician. For patients who are eventually able to reduce their medication use as their structural component is addressed, those decisions are made in coordination with the prescribing physician.
What if I cannot remember any neck trauma?
The precipitating event is often distant in time and not consciously connected to current symptoms. Many patients cannot recall the original event, particularly when it occurred in childhood, in sports, or in minor accidents that did not require medical attention. The absence of a remembered trauma does not rule out an upper cervical contribution. A structural evaluation can identify misalignment regardless of whether you can recall how it began.
Is the free consultation really free?
Yes. The initial consultation is offered at no cost and is designed to determine whether upper cervical care is appropriate for your situation. It includes a thorough history conversation and examination. If we determine that further evaluation with CBCT imaging or objective testing is warranted, that becomes a separate decision and is discussed with you before proceeding.
How do I schedule the free consultation?
Call our office at 941-259-1891. Our team will schedule you at a time that works for you.
Take the Next Step
Chronic headaches deserve a thorough evaluation that includes a precise structural assessment of the upper cervical spine. For most patients with chronic headache, this assessment has not yet been part of their workup. It often becomes the step that opens the answer they have been searching for.
Sarasota Upper Cervical Chiropractic serves patients throughout the Sarasota and Bradenton areas.
To schedule your free consultation, call 941-259-1891.
References
Flanagan, M. F. (2015). The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Research International, 2015, Article 794829.
Hack, G. D., Koritzer, R. T., Robinson, W. L., Hallgren, R. C., & Greenman, P. E. (1995). Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine, 20(23), 2484–2486.
Bogduk, N., & Govind, J. (2009). Cervicogenic headache: An assessment of the evidence on clinical diagnosis, invasive tests, and treatment. The Lancet Neurology, 8(10), 959–968.
Calhoun, A. H., Ford, S., Millen, C., Finkel, A. G., Truong, Y., & Nie, Y. (2010). The prevalence of neck pain in migraine. Headache, 50(8), 1273–1277.
Luedtke, K., Starke, W., & May, A. (2017). Musculoskeletal dysfunction in migraine patients. Cephalalgia, 38(5), 865–875.
International Headache Society (2018). The International Classification of Headache Disorders, 3rd edition. Cephalalgia, 38(1), 1–211.
Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355–359.
McLain, R. F. (1994). Mechanoreceptor endings in human cervical facet joints. Spine, 19(5), 495–501.
Bartsch, T., & Goadsby, P. J. (2003). The trigeminocervical complex and migraine: Current concepts and synthesis. Current Pain and Headache Reports, 7(5), 371–376.
Peng, B., Yang, L., Yang, C., Pang, X., Chen, X., & Wu, Y. (2022). Proprioceptive cervicogenic dizziness: A narrative review of pathogenesis, diagnosis, and treatment. Journal of Clinical Medicine, 11(21), 6293.
Antonaci, F., & Sjaastad, O. (2011). Cervicogenic headache: A real headache. Current Neurology and Neuroscience Reports, 11(2), 149–155.
Treleaven, J., Jull, G., & Sterling, M. (2003). Dizziness and unsteadiness following whiplash injury: Characteristic features and relationship with cervical joint position error. Journal of Rehabilitation Medicine, 35(1), 36–43.
This article is educational in nature and does not constitute medical advice, diagnosis, or treatment. Individual results vary. Chiropractic care focuses on the structure and function of the spine and nervous system. Patients with chronic headache should pursue appropriate medical evaluation alongside any structural assessment. No claim is made or implied that upper cervical chiropractic cures or treats any specific disease.



Leave a comment