
"Why the upper cervical spine may be the missing piece — what the published research says, the vestibular pathways involved, and how a precision-based, gentle correction can help"
Vestibular migraine is one of the most frustrating diagnoses in modern neurology — not because it lacks treatments, but because the treatments rarely address the underlying mechanism, and patients are often told the condition is something to manage rather than something to truly resolve. The migraines come with vertigo. The vertigo comes with nausea. Light and sound become enemies. Driving feels unsafe. Work suffers. Sleep suffers. And the medications, while sometimes helpful, often trade one set of symptoms for another.
Schedule Your Appointment
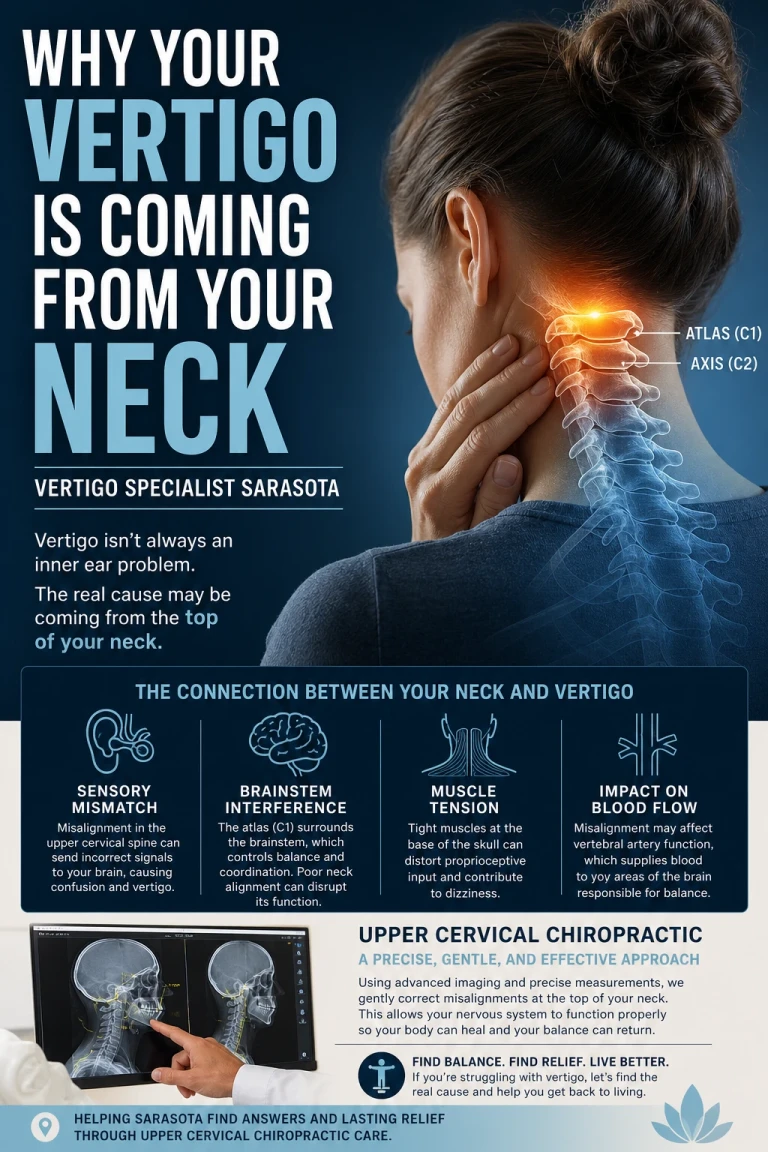
Schedule appointmentWhat is rarely discussed, and almost never imaged, is the role of the upper cervical spine — the joints between the skull and the first two vertebrae, where the brainstem, the vestibular nuclei, the trigeminal nerve, and the cervical spinal cord all converge. A growing body of research suggests this region may be a meaningful and overlooked contributor to vestibular migraine. For patients in Sarasota who have cycled through neurologists, ENTs, vestibular therapists, and a long list of medications without lasting relief, the upper cervical spine deserves a serious look.
This article explains what vestibular migraine actually is, what the published research on upper cervical chiropractic care for migraine and vestibular migraine shows, the specific vestibular pathways that can be affected by a craniocervical junction misalignment, and what a precision-based, non-twisting upper cervical correction can offer.
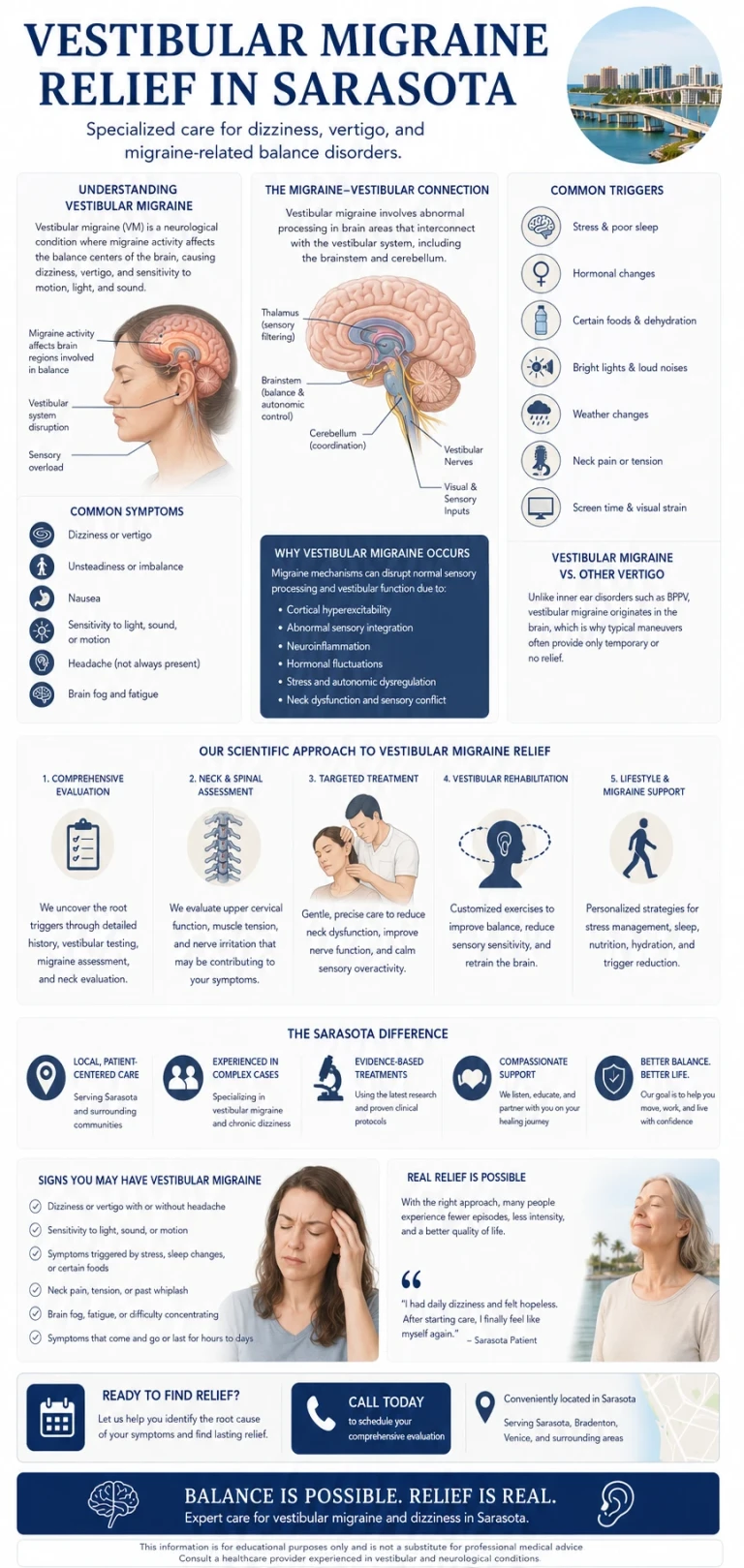
What Vestibular Migraine Is, and Why It’s So Hard to Treat
Vestibular migraine is a relatively young diagnostic entity. It was formally codified in 2012 by the Bárány Society and the International Headache Society, and it remains one of the most common causes of recurrent vertigo in adults. Patients meet criteria when they have a history of migraine, plus recurrent vestibular symptoms — vertigo, dizziness, motion sensitivity, imbalance — that occur with at least half of their migraine episodes.
The pathophysiology is still incomplete. Current hypotheses include abnormal thalamic function, calcitonin gene-related peptide (CGRP) release affecting the inner ear and brainstem, genetic factors, abnormal processing of vestibular and pain signals in the brainstem, and trigeminal-vascular dysfunction. These are real mechanisms, and they explain a great deal. But they do not explain everything, and the standard pharmacologic treatments — triptans, beta blockers, CGRP antagonists, anti-seizure medications — do not work for everyone.
What is striking in the more recent literature is the observation that the cervical spine has been almost entirely left out of the conversation, despite a substantial body of clinical, experimental, and anatomical evidence linking upper cervical afferents to the production of vestibular symptoms. A 2024 paper published in Health Open Research stated this directly: the potential contribution of upper cervical afferents to vestibular migraine “is consistently omitted” from the mainstream discussion. That gap is starting to close, and the early research is worth understanding.
The Research: What Published Studies Are Showing

Two recent studies stand out, both published in PubMed-indexed journals.
In 2024, a research team led by O’Toole, Watson, Hall, Treleaven, and Luedtke published a case series in Health Open Research titled “Manual cervical therapy and vestibular migraine: A case series.” The authors prospectively followed three patients who met strict diagnostic criteria for vestibular migraine. Each patient received a course of manual cervical therapy targeting the upper cervical spine. All three patients demonstrated improvement in both migraine attack frequency and the dizziness symptoms they experienced between attacks. These improvements were sustained over a six-month follow-up period. The authors concluded that the upper cervical spine “could be a therapeutic target in vestibular migraine and may have implications for future research into the pathogenesis of VM.”
Earlier, in 2015, Woodfield and colleagues published a larger observational pilot study in BioMed Research International titled “Effect of Atlas Vertebrae Realignment in Subjects with Migraine.” Eleven patients, all diagnosed with migraine by their medical neurologist, received NUCCA-protocol upper cervical chiropractic care with follow-up at four and eight weeks. The participants reported an average reduction of nearly six migraine days per month by the eighth week. The study also measured intracranial compliance using phase-contrast MRI, exploring whether the atlas correction was changing how the brain manages fluid pressure. The compliance results were mixed, but the symptomatic improvement was clear, and the study concluded that atlas realignment “may be associated with reduction in migraine frequency, marked improvement in quality of life yielding significant reduction in headache-related disability.”
These are small studies. They are not randomized controlled trials, and they do not prove that upper cervical care cures vestibular migraine — nothing in the literature claims that. What they do show is a consistent clinical pattern: patients with a structural component to their migraine experience meaningful improvement when the upper cervical spine is addressed precisely. That pattern is significant enough to take seriously.
The Vestibular Pathways a CCJ Misalignment Can Affect
Balance is not produced in any single place. It is produced through the coordinated activity of multiple pathways, all of which converge in or pass through the brainstem at the level of the craniocervical junction. When this region is misaligned, several distinct pathways can be affected simultaneously — and in vestibular migraine, that simultaneous disruption is likely part of why the condition feels so all-encompassing.
The first pathway involves direct cervical proproioceptive input from the upper cervical joints into the vestibular nuclei. The atlas and axis contain the highest density of mechanoreceptors anywhere in the spinal column. These joint sensors feed continuous information about head position and movement into the brainstem, where it converges with input from the inner ear and the eyes inside the vestibular nuclei. When the upper cervical joints are misaligned, that input becomes distorted. The brain then receives a signal from the neck that conflicts with what the inner ear and eyes are reporting. The brain interprets that mismatch as dizziness, unsteadiness, or vertigo — and in a brain already primed for migraine, the same mismatch can also serve as a trigger for an attack.
The second pathway involves the vestibulospinal tracts. These are the descending pathways that carry information from the vestibular nuclei down to the spinal cord, where they coordinate antigravity postural muscle activity, balance reflexes, and head-on-body orientation. The medial vestibulospinal tract specifically activates the cervical axial muscles in response to inner ear signals. When upper cervical mechanoreceptor input is abnormal, these reflex loops can become dysregulated, producing the chronic postural unsteadiness many vestibular migraine patients describe even between attacks.
The third pathway involves the trigeminal-vascular system. Migraine, including vestibular migraine, is increasingly understood as a brainstem phenomenon mediated through the trigeminal nerve and the upper cervical spinal cord. The trigeminal nucleus extends down into the upper cervical cord, where it shares territory with afferents from the cervical spine. This means upper cervical input and trigeminal input converge in the same neurons — a relationship called convergence. Sustained noxious input from a misaligned upper cervical joint can sensitize these shared neurons, lowering the threshold for migraine activation. This is one of the most plausible mechanisms by which neck dysfunction can directly trigger migraine attacks, and it has been described in peer-reviewed neurology literature by Goadsby and colleagues.
The fourth pathway involves the vestibulocochlear nerve (cranial nerve VIII) and the surrounding fluid dynamics of the craniocervical junction. The vestibulocochlear nerve carries signals from the inner ear to the brainstem, exiting the brainstem in the immediate vicinity of the CCJ. The same region houses the channels for cerebrospinal fluid (CSF) flow between the brain and the spinal cord, and the internal jugular veins responsible for draining most of the venous blood out of the skull. A misalignment at the CCJ can subtly impair CSF flow, reduce jugular venous drainage, and raise intracranial pressure. The inner ear is pressure-sensitive — it depends on a precisely balanced relationship between endolymph and perilymph pressures for normal function. Even small changes in intracranial pressure can therefore alter inner ear function, producing vertigo, ear fullness, and motion sensitivity, all common features of vestibular migraine.
Reduced clean input from upper cervical mechanoreceptors. Dysregulated vestibulospinal reflexes. Sensitized trigeminal-cervical convergence. Altered fluid dynamics affecting the inner ear. Four pathways, all running through the same anatomical region, all potentially affected by the same misalignment. For someone with vestibular migraine, this is not a single trigger — it is a stacked load on a system that is already predisposed to attack.
CBCT Imaging: Precision Before Anything Else
Before any care begins in our Sarasota office, we use Cone Beam Computed Tomography (CBCT) imaging of the upper cervical spine. CBCT is a precision imaging tool that produces three-dimensional views of the skull base, atlas, axis, and surrounding structures — detail that flat two-dimensional X-rays cannot provide.
Every craniocervical junction is built differently. The angles, the orientations, and the relationships between the skull, C1, and C2 are unique to each person. Without precision measurements, an upper cervical correction is a guess. With them, the correction can be specific, gentle, and matched to your exact anatomy. For a vestibular migraine patient who has been through workup after workup without anyone imaging the structure most likely to be driving the problem, this is often the first time the actual mechanical picture is being looked at directly.
No Twisting. No Cracking. No Pulling of the Neck
Most people picture a chiropractic adjustment as a fast head-turn and a popping sound. That is not what we do. The correction we deliver is specific, low-force, and based directly on the measurements taken from your CBCT scan. There is no twisting, cranking, or pulling. No cavitation noise. You lie on your side with your head supported. The correction takes seconds.
For a vestibular migraine patient, this matters enormously. The vestibular system is already sensitized. Sudden head movement is often a trigger. A forceful manipulation is the wrong tool. Our approach is built specifically to give the brainstem cleaner input from the upper cervical joints without adding mechanical stress to a system that is already in a heightened state of alert.
Gentle does not mean ineffective. Gentle means we are working with the nervous system rather than against it. The goal is to restore mechanical and neurological balance at the craniocervical junction so the vestibular nuclei, the trigeminal-cervical complex, and the inner ear can all do their jobs without the chronic conflicting input that has been part of the migraine pattern.
Who This Tends to Help
Related article
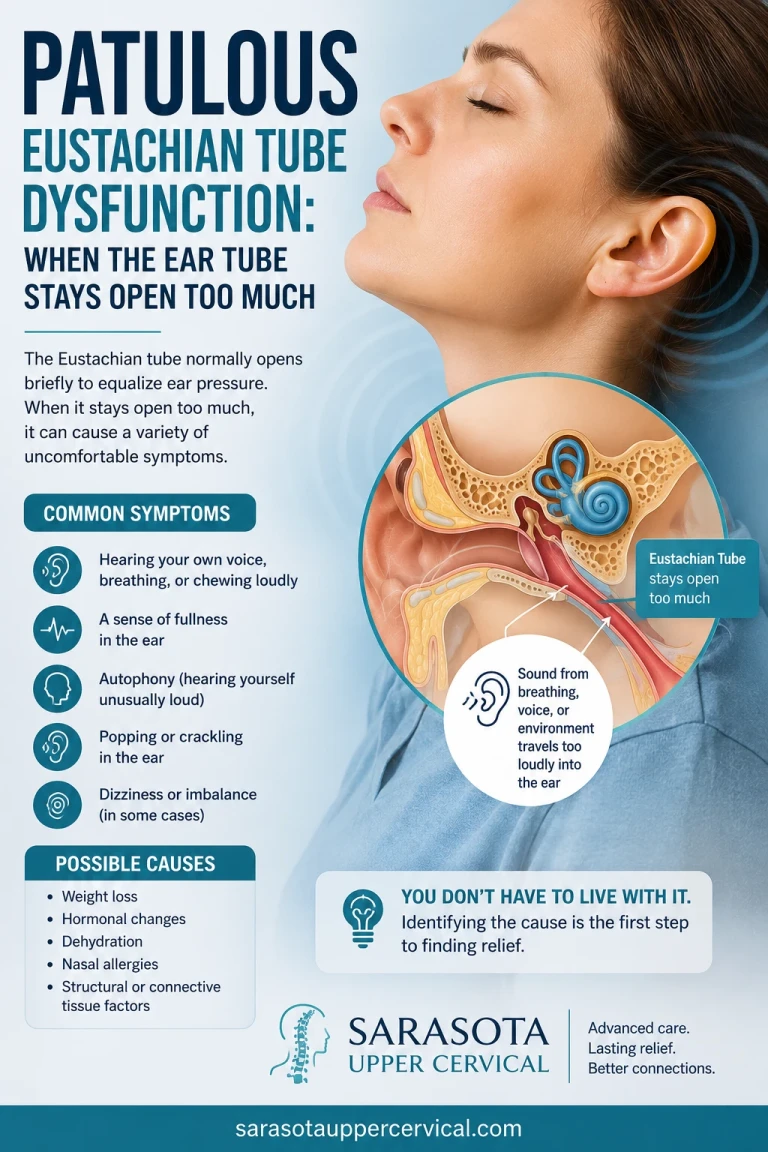
Patulous Eustachian Tube Dysfunction: When the Ear Tube Stays Open Too Much
May 26, 2026
The patient we see most often in this category has a story that sounds familiar. Migraines that began or worsened after a specific incident — a car accident, a concussion, a fall, a whiplash injury, sometimes even a dental procedure. A neurologist diagnosis of migraine, often with vestibular features. Triptans that work but only sometimes. A preventive medication that helps modestly but comes with side effects. Vestibular therapy that helps with some symptoms but not the attacks themselves. And a slowly growing suspicion that the root cause has not actually been identified.
Common features include attacks triggered or worsened by neck position, neck stiffness or pain that the patient may not have connected to the migraines, symptoms that worsen with stress, fatigue, screen time, or weather changes, and a sense of low-grade unsteadiness or visual motion sensitivity between attacks. None of these features are diagnostic on their own, but together they raise the question of whether the upper cervical spine is part of the migraine picture.
A Realistic First Visit, and a Real Path Forward
A first visit in our Sarasota office includes a thorough consultation, a focused examination, and CBCT imaging of the upper cervical spine. We pay particular attention to your full history — including any head or neck trauma, even decades old, because those events are often where the migraine story actually begins. After we review the imaging with you, we will tell you honestly whether upper cervical care looks like a good fit. If it is, we build a plan. If it is not, we say so and point you toward what is more likely to help.
Care for vestibular migraine works best when it is layered. Upper cervical chiropractic is one piece. Working with your neurologist on appropriate medication management is another. Sleep, hydration, identifying and avoiding personal triggers, regular movement, and stress regulation all matter. We do not replace any of that. We add a piece that often goes missing — the structural and neurological foundation that supports everything else.
If You’re Living With Vestibular Migraine in Sarasota
Vestibular migraine doesn’t have to be a permanent condition you manage around. The published research, while still early, is consistent enough to take seriously. The mechanism — the convergence of multiple vestibular pathways at the craniocervical junction — is anatomically real and supported by mainstream neurology literature. And the approach itself — precision imaging, a specific and gentle correction, no twisting of the neck — is exactly the opposite of what an already sensitized vestibular system fears.
If you are looking for vestibular migraine relief in Sarasota and you want to understand whether the upper cervical spine might be part of your picture, the next step is a conversation and a proper look at your anatomy. We will go through your history, image your craniocervical junction, and give you a straight answer about whether this approach makes sense for you.
Ready to take the next step? Schedule a consultation at our Sarasota office to start with a complete upper cervical evaluation and CBCT imaging.
References: O’Toole R, Watson D, Hall TM, Treleaven J, Luedtke K. Manual cervical therapy and vestibular migraine: A case series. Health Open Res. 2024. • Woodfield HC III, Hasick DG, Becker WJ, Rose MS, Scott JN. Effect of Atlas Vertebrae Realignment in Subjects with Migraine: An Observational Pilot Study. Biomed Res Int. 2015;2015:630472. • Goadsby PJ, et al. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017. • Treleaven J. Dizziness, unsteadiness, visual disturbances, and sensorimotor control in traumatic neck pain. J Orthop Sports Phys Ther. 2017. • Lempert T, Olesen J, et al. Vestibular migraine: diagnostic criteria. J Vestib Res. 2012.
Disclaimer: This article is for educational purposes only and does not constitute medical advice or a substitute for care from your neurologist. Vestibular migraine should be evaluated and managed by a qualified medical provider. Upper cervical chiropractic care does not diagnose, treat, or cure vestibular migraine or any other neurological disorder. The research cited above is preliminary and does not constitute proof of efficacy. Individual results vary.



Leave a comment