

"How precision upper cervical care addresses the structural piece of the CCI puzzle — without twisting, popping, or pulling the neck"
If you've been searching for craniocervical instability relief in Sarasota, you've probably already lived through a long list of specialists, imaging studies, and treatments that didn't fully resolve your symptoms. You may have a confirmed CCI diagnosis through a referral center, or you may suspect CCI based on a constellation of symptoms — headaches at the base of the skull, dizziness, brain fog, the unsettling feeling that your head is too heavy for your neck to hold. Either way, the upper cervical spine is one of the most overlooked structural variables in your care, and addressing it correctly can make a meaningful difference.
Schedule Your Appointment
Schedule appointmentAt our Sarasota practice, we focus on the upper cervical spine — specifically the relationship between the skull, the atlas (C1), and the axis (C2). The technique we use is the Blair upper cervical method, a precision-driven, low-force approach that does not involve twisting the neck, popping joints, or pulling on the head. For patients with craniocervical instability or CCI-pattern symptoms, the absence of forceful manipulation is not a marketing point. It is a clinical requirement.
What Craniocervical Instability Actually Is
Craniocervical instability is a structural condition in which the ligaments that connect the skull to the upper cervical spine — primarily the alar, transverse, and apical ligaments — are unable to hold the head in a stable relationship with the neck. The result is excessive movement between the skull, the atlas, and the axis. That excessive movement can irritate, compress, or stretch the brainstem, the upper spinal cord, the vertebral arteries, the jugular veins, and the cerebrospinal fluid pathways that pass through the craniocervical junction.
CCI is most commonly recognized in patients with hereditary connective tissue disorders such as Ehlers-Danlos syndrome, but it can also follow trauma — whiplash, sports injuries, falls — or develop in connection with conditions like rheumatoid arthritis, Down syndrome, or post-surgical changes following Chiari decompression. Severe structural CCI is a serious medical condition, and surgical fusion is sometimes the appropriate treatment. We want to be clear about that. Upper cervical chiropractic is not a substitute for neurosurgical evaluation when true structural instability is present. What it can offer, however, is conservative care that addresses misalignment at the craniocervical junction — which is often present alongside, or contributing to, the symptoms patients describe.
Why the Craniocervical Junction Matters So Much
The craniocervical junction — the small region where your skull meets the top of your spine — is not just a pivot point for head movement. It is one of the most anatomically dense and functionally critical regions in the human body. In a 2015 peer-reviewed paper published in Anatomy Research International, Dr. Michael F. Flanagan, a chiropractic neurologist and longtime researcher of the craniocervical junction, described the CCJ as a "potential choke point for craniospinal hydrodynamics." That single phrase captures the problem.
Three critical systems converge at the craniocervical junction:
• Arterial inflow to the brain through the vertebral arteries, which pass through small foramina in the atlas and axis before joining to form the basilar artery.
• Venous drainage out of the brain, particularly through the vertebral venous plexus, which Flanagan and others have argued is the primary venous drainage route when the body is upright.
• Cerebrospinal fluid (CSF) flow between the cranial vault and the spinal canal, which depends on the patency and geometry of the upper cervical spinal canal.
When the structures at this junction are misaligned — whether from ligament laxity (true CCI), trauma, or chronic mechanical strain — these three systems can all be affected at once. Flanagan's body of work, including his book The Downside of Upright Posture, argues that disruption at the craniocervical junction can contribute to chronic ischemia (reduced blood flow into the brain), venous congestion (slowed drainage out of the brain), and altered CSF dynamics. He and other researchers have suggested links between these disruptions and a range of chronic neurological conditions. Whether you accept the full scope of his hypotheses or not, the underlying anatomical reality is well established: this is a region where small structural changes have outsized physiological consequences.
Related article
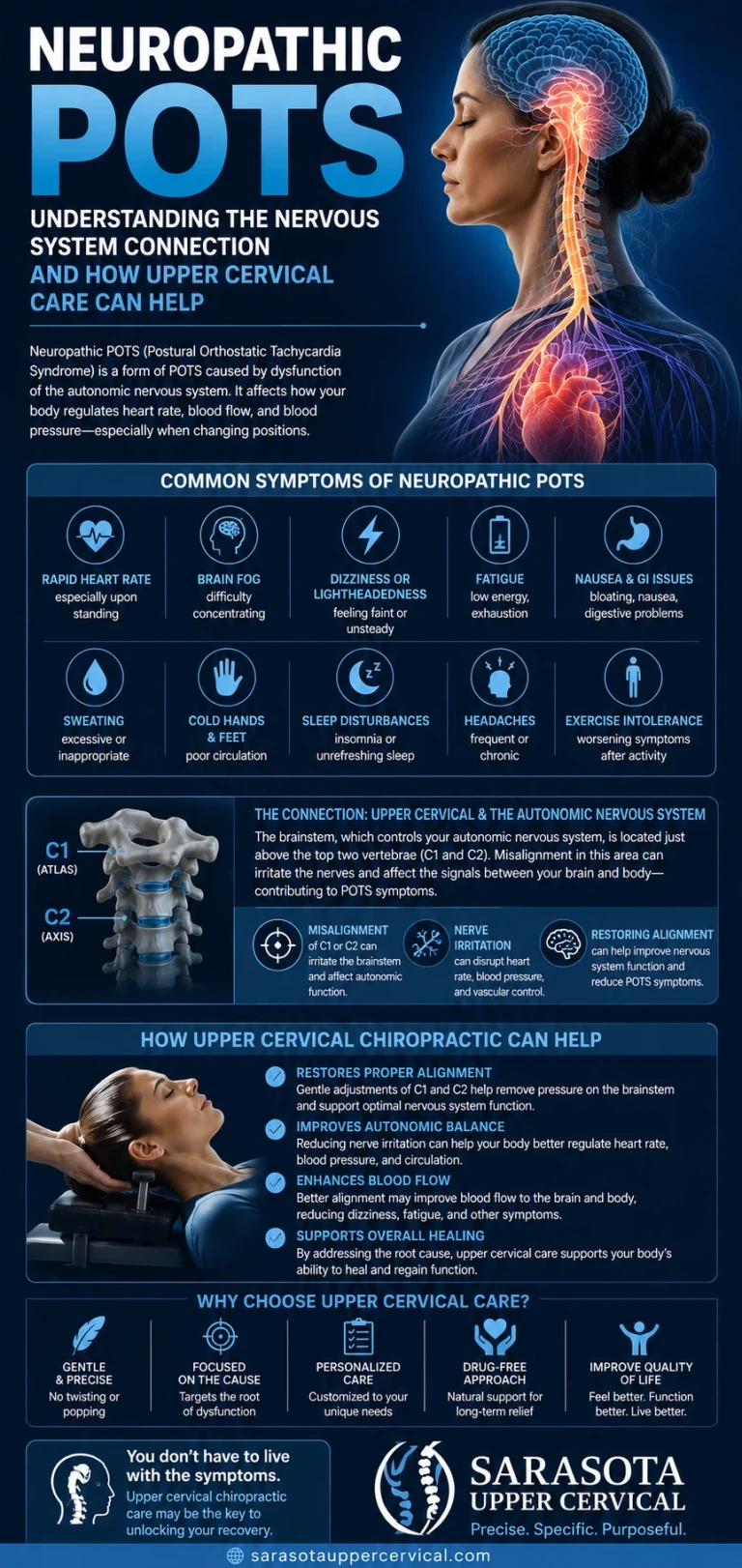
Neuropathic POTS and the upper neck connection | Holistic healing for POTS
Jul 14, 2026Abnormal Proprioceptive Input — The Hidden Driver of CCI Symptoms
The other reason the upper cervical spine matters in CCI is what it tells your nervous system. The suboccipital region — the small muscles at the base of your skull — contains one of the highest densities of muscle spindles in the entire body. Muscle spindles are sensory receptors that report position, movement, and tension to the central nervous system. The facet joints at C0-C1 and C1-C2 are similarly packed with mechanoreceptors that report joint position.
When the atlas and axis are misaligned, the input from these receptors becomes asymmetric and chronically abnormal. The brain receives a continuous stream of mismatched signals about where the head is in space. That mismatch — combined with conflicting signals from the visual system and the inner ear — is one of the proposed mechanisms behind many of the symptoms patients with CCI describe: dizziness, vertigo, visual disturbances, brain fog, difficulty concentrating, and a generalized sense that something is "off." The cord and brainstem also receive this aberrant input, and the cascade of downstream effects can include autonomic dysregulation, sleep disturbance, and pain processing changes.
Correcting the structural misalignment doesn't just restore mechanical position. It changes the sensory information the nervous system is working with.
Symptoms Commonly Associated with CCI
Patients with craniocervical instability or CCI-pattern symptoms often present with combinations of the following:
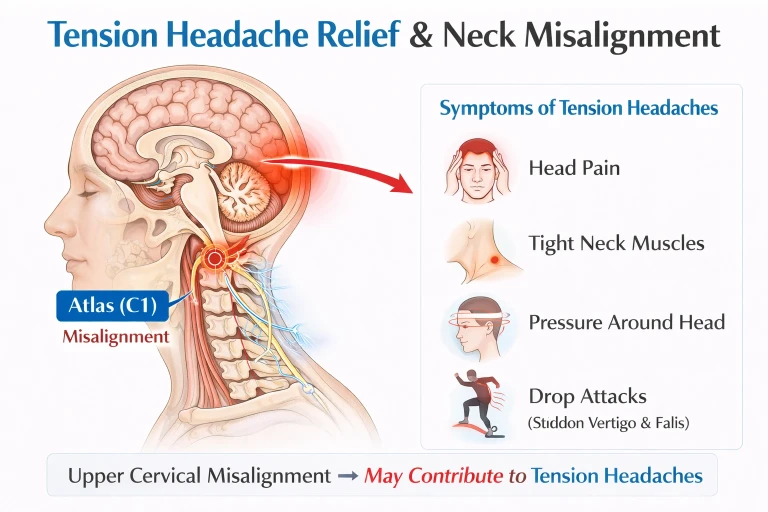
• Severe occipital pain or upper neck headaches, often described as "pressure at the base of the skull"
• The "bobblehead" sensation — the feeling that the head is too heavy for the neck to support
• Dizziness, vertigo, or chronic disequilibrium
• Brain fog, memory difficulties, and word-finding problems
• Visual disturbances — blurred vision, double vision, light sensitivity
• Tinnitus, fullness in the ears, or hearing changes
• Autonomic dysfunction including POTS (postural orthostatic tachycardia syndrome), rapid heart rate, and temperature regulation problems
• Swallowing difficulty, voice changes, or a "lump in the throat" sensation
• Facial numbness, tingling, or spasms
• Fatigue that doesn't improve with rest
• Anxiety, mood changes, and sleep disturbance
• Numbness, weakness, or tingling in the arms or hands
Not every patient has every symptom, and many of these symptoms have other potential causes. That is precisely why a thorough workup matters. A CCI-pattern symptom presentation is not the same as a confirmed structural CCI diagnosis, and the appropriate next step depends on the full clinical picture.
How CBCT Imaging Identifies the Exact Misalignment
One of the things that separates precision upper cervical chiropractic from general chiropractic care is the imaging. Standard cervical X-rays show the spine in two dimensions and cannot accurately capture the three-dimensional relationships between the skull, atlas, and axis. The Blair upper cervical technique was developed around the recognition that every patient's upper cervical anatomy is unique — the angles of the joint surfaces, the orientation of the atlas, and the position of the axis vary from person to person.
Cone Beam Computed Tomography, or CBCT, is a low-dose three-dimensional imaging technology that allows us to see the actual joint surfaces of the upper cervical spine in three planes simultaneously. With a CBCT scan, we can measure the exact angular and positional relationship of the atlas to the skull above and the axis below. We can identify which side is misaligned, in which direction, and by how many degrees and millimeters. We can also see the structural anatomy of the joint surfaces — which means the correction is built around your specific anatomy, not a generic template.
For patients with CCI or CCI-pattern symptoms, this matters for two reasons. First, it allows the correction to be highly specific, which reduces the force required to deliver it. Second, it gives us an objective baseline. We can see, on imaging, what was misaligned before care began, and we can verify the change. That kind of objectivity is rare in conservative care.
The Blair Adjustment — No Twisting, No Popping, No Pulling
For a patient with craniocervical instability, the idea of having their neck adjusted can be understandably frightening. Many patients with CCI have been told by neurologists, physical therapists, and sometimes other chiropractors that manipulation is contraindicated for their condition. That advice is correct when it refers to high-velocity, rotational adjustments — the kind that produce an audible "crack" and require the neck to be twisted past its natural range. Those techniques can be inappropriate for any patient with ligament laxity at the craniocervical junction.
The Blair upper cervical technique is fundamentally different. The patient lies on their side on a specialized table. The head is supported throughout. The contact is gentle, made with the fingertip on a precise anatomical landmark on the side of the atlas. The correction itself is a small, low-velocity, low-amplitude impulse delivered along the vector calculated from the patient's own CBCT imaging. There is no rotation. There is no traction. There is no popping or cracking. Many patients describe the correction as feeling like a soft tap. The objective is not to force motion into the joint, but to restore alignment along the path the joint itself is designed to move.
Related article
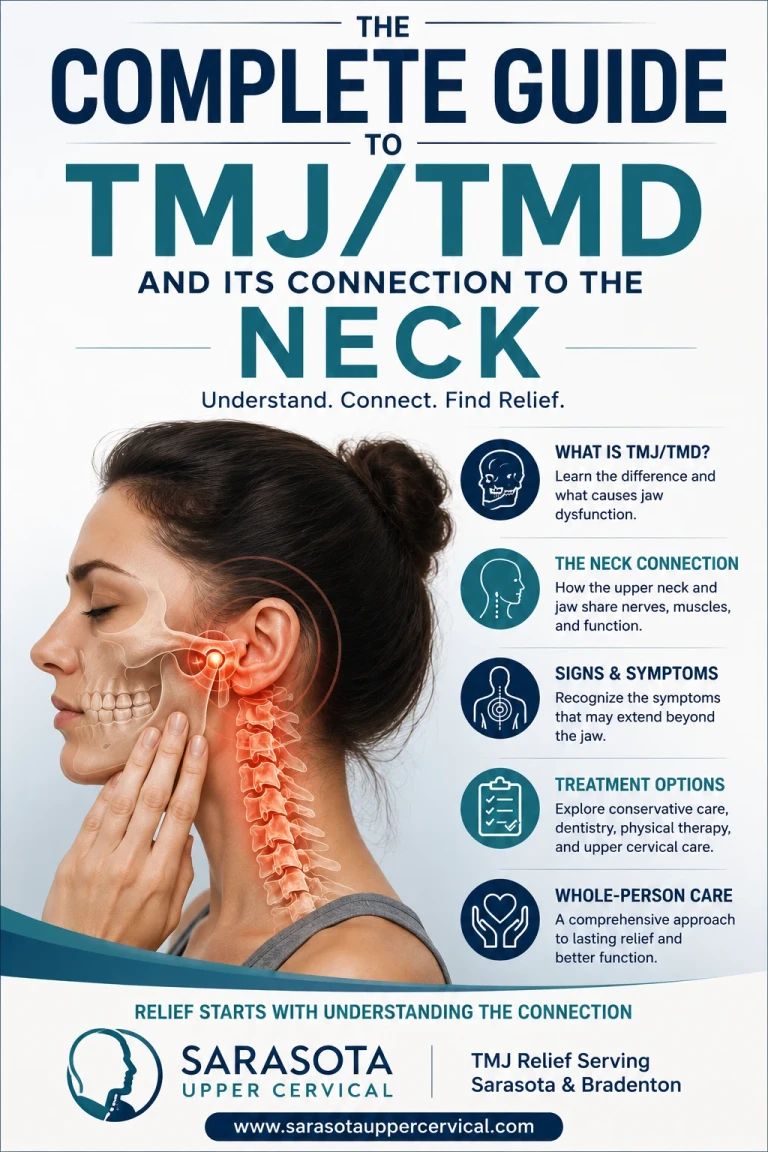
The Complete Guide to TMJ/TMD and Its Connection to the Neck | Tmj treatment and relief sarasota
Jun 14, 2026For patients with hypermobility, connective tissue disorders, or post-traumatic instability, this matters. The body has enough mechanical irritation already. The last thing it needs is more.
What Happens After Correction
When the structural misalignment is corrected and held, several things tend to follow. The proprioceptive input from the upper cervical region begins to normalize. The chronic asymmetric signaling that has been feeding into the brainstem starts to settle. Patients often describe a reduction in dizziness and brain fog within the first few weeks of care. The mechanical stress on the vertebral arteries and venous drainage pathways is reduced, which can support improvements in pressure-related symptoms — headaches, head pressure, ear fullness. Sleep frequently improves, and many patients notice their nervous system feeling "quieter" — less reactive, less constantly on alert.
We want to be honest about what we don't claim. We do not claim that upper cervical care cures CCI. We do not claim it replaces neurosurgical evaluation when true structural instability is present. We do not claim that every patient with CCI-pattern symptoms will respond. Results vary, and they depend on the underlying causes, the severity of the structural changes, the patient's overall health, and how long the condition has been present. What we can offer is a thorough evaluation, precision imaging, a corrective approach that does not add mechanical risk, and a clinical perspective that takes the structural piece of the puzzle seriously.
If You're Considering Care in Sarasota
If you've been searching for craniocervical instability relief and you live in Sarasota, Bradenton, Venice, Lakewood Ranch, or anywhere in the surrounding area, the first step is a no-pressure consultation. The consultation is free. It includes a thorough history, a physical examination, and an honest conversation about whether upper cervical care makes sense in your specific situation. If imaging is appropriate, we can review your existing studies or recommend a CBCT scan. If your case is one where neurosurgical evaluation should come first, we will tell you that. If conservative care is the right next step, we will explain the plan, the timeline, and what to expect.
Craniocervical instability is a serious condition, and the right care begins with the right evaluation. The upper cervical spine is one of the most overlooked variables in CCI symptom management, and addressing it correctly — precisely, gently, and based on your own anatomy — is often the missing piece of the puzzle.
References
• Flanagan MF. The Role of the Craniocervical Junction in Craniospinal Hydrodynamics and Neurodegenerative Conditions. Anatomy Research International, 2015. Open-access. Available via PMC: PMC4681798.
• Flanagan MF. The Downside of Upright Posture: The Anatomical Causes of Alzheimer's, Parkinson's and Multiple Sclerosis. Two Harbors Press, 2010.
• Flanagan MF. About Dr. Flanagan / Upright Doctor blog — uprightdoctor.wordpress.com
• Henderson FC Sr, et al. Craniocervical instability in patients with Ehlers-Danlos syndromes: outcomes analysis following occipito-cervical fusion. Neurosurgical Review, 2024.
• Klinge PM, et al. Craniocervical Instability in Ehlers-Danlos Syndrome — A Systematic Review of Diagnostic and Surgical Treatment Criteria. PMC9609512.
This article is for educational purposes only and is not medical advice. Craniocervical instability is a serious condition that requires individualized clinical evaluation. If you suspect CCI, consult with a qualified healthcare provider. Upper cervical chiropractic care focuses on the structural alignment of the upper cervical spine and is not a substitute for neurosurgical evaluation when structural instability is present



Leave a comment