
You’ve tried things. Maybe masking devices or a white-noise app. Maybe supplements, a hearing aid, a change in diet, or cutting caffeine. Maybe your doctor ran tests, found nothing definitive, and told you the same thing so many people hear: there’s no cure, and you’ll need to learn to live with it.
And yet the ringing is still there.
Schedule Your Appointment
Schedule appointmentIf that’s where you are, it’s worth asking a different question. Not “how do I cover up the sound?” but “what is actually driving it — and has that driver ever been evaluated?” For a meaningful number of people in Sarasota, the answer that was missed lies in the upper neck.
If your tinnitus hasn’t responded to other approaches, schedule a free consultation — book here or call 941-259-1891 to see if you’re a candidate for care.
Why “Just Live With It” Leaves So Many People Stuck
Most conventional tinnitus care is built around one assumption: that the sound originates in the ear or the hearing pathway, and that if it can’t be cured there, the only option left is to manage how much it bothers you. That’s where masking, sound therapy, and coping strategies come in. They can genuinely help people cope — but they are designed to make the sound easier to ignore, not to address why it’s being produced.
So if your tinnitus has a driver that lives outside the ear, these approaches can fall short no matter how diligently you follow them. You’re treating the volume knob while the actual signal goes unexamined. That mismatch is one of the most common reasons tinnitus persists despite real effort.
The Structural Cause That Often Gets Overlooked
Tinnitus has many possible causes. One that is frequently missed in a standard workup is a structural component in the upper neck.
Related article
Seeing the Whole Picture: CBCT, the Blair Analysis, and Why Precision Changes Outcomes
Jun 20, 2026The nerves and joints of the upper cervical spine — especially around the atlas (C1) and axis (C2) — feed signals into the same region of the brainstem that handles early auditory processing. When the atlas is misaligned, the distorted position and tension information it sends upward can contribute to the brain generating or amplifying a phantom sound. This is sometimes called the somatosensory, or somatic, component of tinnitus.
The reason it gets overlooked is straightforward: a typical hearing-focused evaluation isn’t looking at the alignment of the top of your neck. If no one examines that region, a structural driver there simply never gets found — and the tinnitus gets filed under “no known cause.”
Signs Your Tinnitus May Have a Neck Component
Certain patterns make an upper cervical involvement more likely. Your tinnitus may have a structural component if:
The sound changes when you move your jaw, neck, head, or eyes
It gets louder with clenching, certain postures, or neck tension
It started or worsened after a head or neck injury, whiplash, or concussion
It comes alongside neck pain, headaches, jaw problems, or dizziness
It hasn’t responded to hearing-based or medication approaches
None of these confirms the cause on its own. But together they are exactly the profile that warrants a closer look at the upper neck — the look most standard tinnitus care never includes.
Why Some Cases Respond and Others Don’t
Here’s the honest part, and it’s the part that should make you trust the process more, not less: not all tinnitus comes from the neck, and not everyone is a candidate for upper cervical care.
Related article
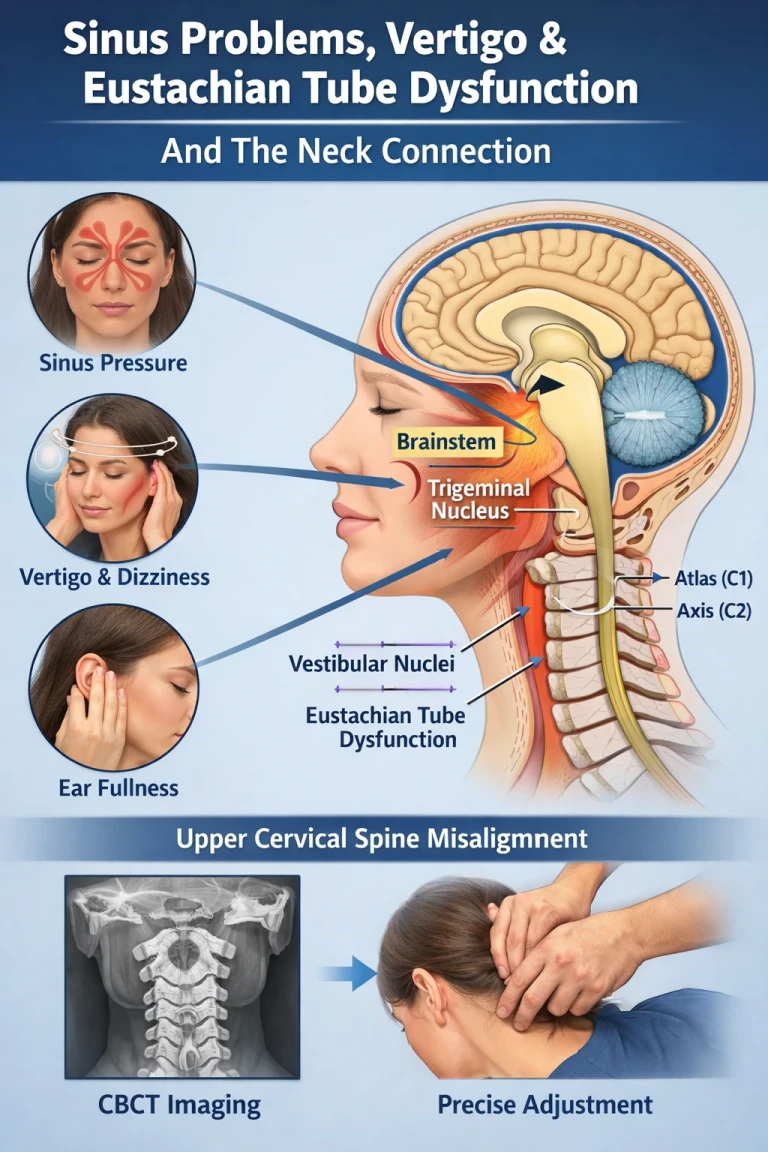
Sinus Problems, Eustachian Tube Dysfunction, Vertigo, and the Neck Connection
Apr 18, 2026Research on treating the cervical spine for tinnitus points consistently to the same conclusion — the benefit appears in a properly selected subgroup of people whose tinnitus has a genuine somatic component. Identifying who falls into that group, through careful evaluation, is the whole game. That’s why a responsible office doesn’t promise everyone relief. The first job isn’t to treat — it’s to find out whether your specific case shows the structural signs that make care appropriate.
If it doesn’t, you deserve to know that too, so you’re not spending time and hope on the wrong path.
How an Upper Cervical Evaluation Is Different
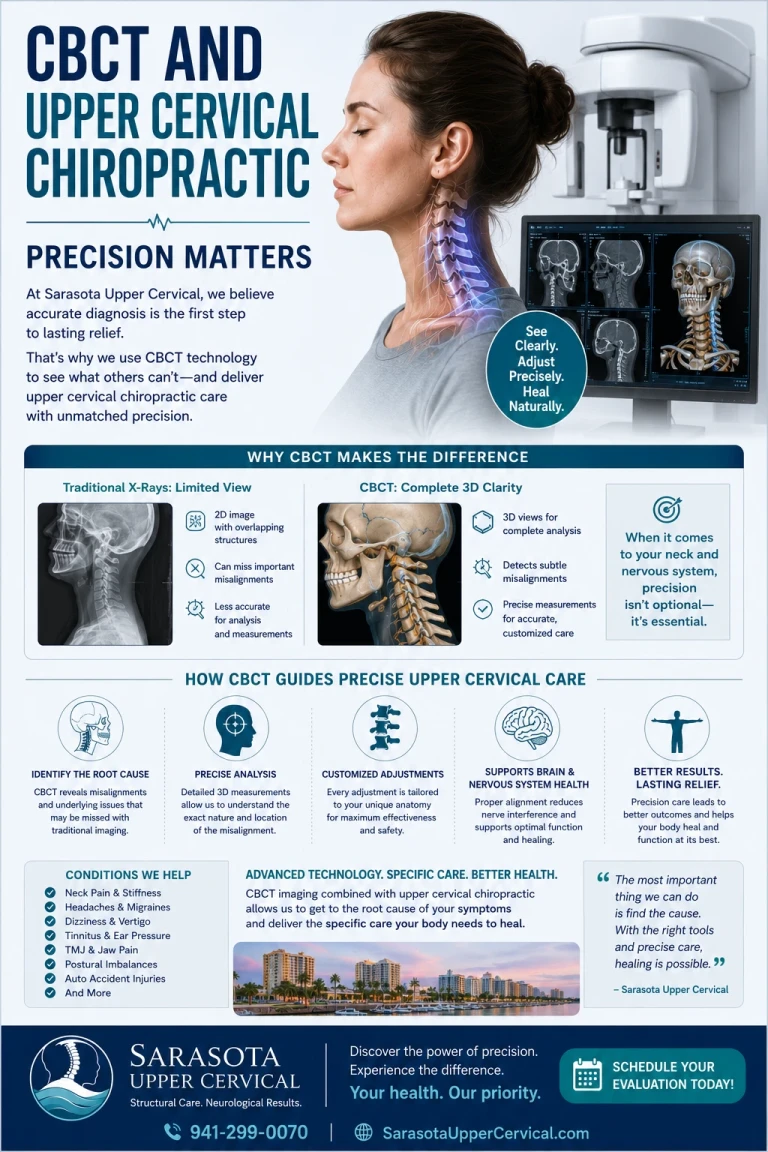
Instead of starting and ending at the ear, an upper cervical evaluation looks at the structure and signaling of the top of your neck. Detailed 3D imaging (CBCT scans) is used as a precision tool to analyze your individual anatomy and measure the exact position of the atlas. This is what makes it possible to tell whether a structural driver is present — rather than assuming it isn’t simply because no one looked.
If a correction is appropriate, it is gentle and specific, with no twisting, popping, or cracking. The goal is to make the right correction and allow the body to hold it over time, so the region where neck and auditory signals converge can function more normally.
A Different Question, A Different Path
If you’ve been told to live with your tinnitus, that advice was based on the causes that were checked. It says nothing about the one that may not have been. For the right candidate, addressing a structural driver in the upper neck focuses on the source of the sound rather than just its volume — and that’s a fundamentally different path than the one most people are offered.
Find Out If Your Neck Is Part of the Picture
You don’t have to keep guessing, and you don’t have to accept “there’s nothing more to do” before the upper neck has ever been evaluated.
Schedule your free consultation today to find out whether you’re a candidate for upper cervical care. Book here or call 941-259-1891 to take the first step.
Related article

Why Upper Cervical Alignment Could Be the Missing Link in Your Chronic Headaches
Oct 06, 2025Learn More
For the full picture of how the neck and tinnitus are connected, start with our complete guide: A Complete Guide to Tinnitus and the Neck Connection. If your ringing changes when you move, read Understanding the Upper Cervical Connection to Ear Ringing, and if it has a whooshing or pulsing quality, see Whooshing & Pulsatile Tinnitus Treatment and Relief in Sarasota.
Frequently Asked Questions
1.Why won’t my tinnitus go away even after treatment?
Most tinnitus care is designed to mask the sound or help you cope, assuming the cause is in the ear. If your tinnitus has a driver outside the ear — such as a structural component in the upper neck — those approaches may not address it, which is one common reason tinnitus persists.
2.Can a neck problem really cause ear ringing?
The nerves of the upper neck feed into the same brainstem region that processes early auditory signals. When the atlas is misaligned, that distorted input can contribute to tinnitus. This is known as the somatic or somatosensory component, and it is often not examined in a standard hearing-focused workup.
3.How do I know if upper cervical care could help me?
Patterns such as tinnitus that changes with movement, started after a head or neck injury, or comes with neck pain or dizziness make a neck component more likely. A thorough evaluation, which may include 3D imaging, is used to determine whether you are a candidate. Not everyone is, and careful selection comes first.
4.Is it too late if I’ve had tinnitus for years?
Length of time alone doesn’t determine candidacy. What matters is whether your case shows a structural component that has never been evaluated. The only way to know is a proper assessment of the upper neck.
5.What’s the first step?Schedule a free consultation to find out whether your tinnitus shows the structural signs that make you a candidate for care. You can book online or call 941-259-1891.
This content is for informational purposes only and does not constitute medical advice.



Leave a comment