
If you've been diagnosed with a Chiari malformation, or you have the headaches, neck pain, dizziness, and pressure symptoms that often go with it, you've probably been told it's a structural problem you were born with, and that your only options are to watch it or have surgery. That's the standard picture. But there's a growing body of research suggesting the relationship between the cerebellar tonsils, the upper neck, and the flow of fluid through the craniocervical junction is more dynamic than once believed. For some people, the neck isn't a bystander to Chiari, it's part of the story.
This article walks through what a Chiari malformation actually is, the difference between the congenital and acquired forms, and the emerging mechanical models that connect the upper cervical spine, the atlas (C1) and axis (C2), to symptom severity. We'll cover cord tethering, the flattening of the cervical curve, the myodural bridge, and the research of clinicians and scientists working at this intersection, including Dr. Scott Rosa's craniocervical junction imaging work. Throughout, one principle stays front and center: upper cervical chiropractic does not treat, repair, or cure a Chiari malformation. What it focuses on is the biomechanics of the craniocervical junction — and for some people, that mechanical environment may be contributing to how they feel. Many cases that have aquired chiari malformation find life changing relief with upper cervical chirorpactic care.
Schedule Your Appointment
Schedule appointmentWhat a Chiari malformation actually is
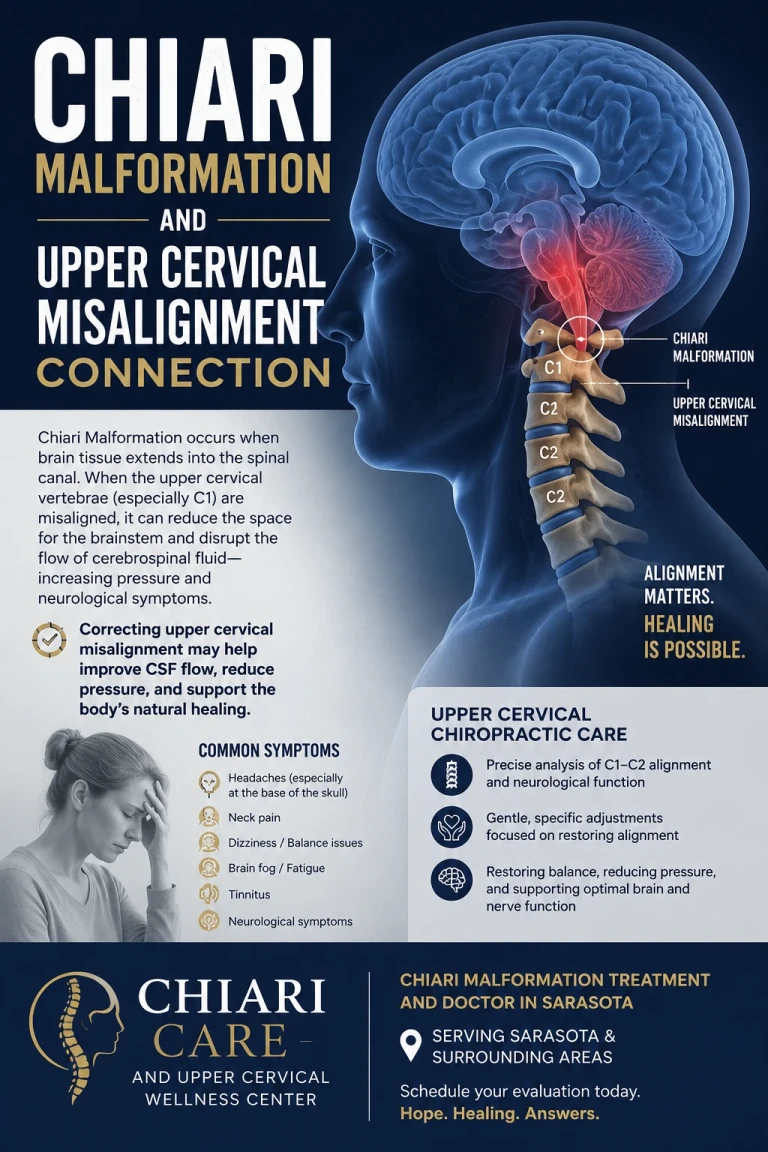
A Chiari malformation type I (CM-I) is defined as downward herniation of the cerebellar tonsils 5 mm or more through the foramen magnum — the large opening at the base of the skull where the brainstem becomes the spinal cord. When the tonsils descend into that opening, they can crowd the space, interrupt the normal pulsing flow of cerebrospinal fluid (CSF) between the brain and spine, and in some cases contribute to a fluid-filled cavity in the cord itself called a syrinx (syringomyelia), which is present in roughly 50–70% of CM-I cases.
The symptoms are highly variable. The classic presentation is an occipital or upper-cervical headache made worse by coughing, sneezing, or straining (Valsalva), but the list also includes dizziness, neck pain, visual disturbance, ringing in the ears, swallowing difficulty, brain fog, balance problems, and tingling in the hands. Crucially, many people with measurable tonsillar descent have no symptoms at all — the finding is incidental. That gap, between the anatomy on a scan and how a person actually feels, is exactly where the upper cervical conversation begins.
Congenital vs. acquired Chiari — and why "acquired" changes everything
The traditional view holds that Chiari is congenital: a posterior fossa (the bony compartment at the back of the skull) that's simply too small for the brain it contains, forcing the tonsils downward. That model is real and well accepted. But it is not the whole picture.
The medical literature now clearly recognizes an acquired Chiari, tonsillar descent that develops in someone who didn't have it before, driven by something other than a small skull. Radiology references note that supratentorial mass effect or low CSF pressure can pull the tonsils downward, a phenomenon termed "acquired Chiari I malformation". Documented cases describe patients with a normal brain MRI at birth who later developed tonsillar descent — showing the position of the tonsils can change over a lifetime rather than being fixed from day one. Huang's 1994 paper formally describing "acquired" Chiari I was a turning point in this thinking.
This matters because the most-cited mechanical triggers for acquired or newly symptomatic Chiari are trauma and instability of the upper neck. One frequently referenced analysis found that about 25% of patients cited trauma — most commonly whiplash from auto accidents or direct blows to the head and neck — as the precipitating factor for their symptoms. In other words: the tonsils may have been sitting quietly at a borderline position, and an injury to the craniocervical junction is what tipped a silent finding into a symptomatic problem.
The key reframe: If a Chiari can be made worse, or made symptomatic, by an upper-neck injury, then the mechanical state of the upper neck is a legitimate variable worth examining. That's the door upper cervical care works within, without ever claiming to alter the malformation itself.
The tethering model: when the cord is pulled from below
One of the most compelling mechanical theories of Chiari is the caudal traction or tethering model — the idea that the cerebellar tonsils don't just fall down, they get pulled down.

The clearest version of this comes from tethered cord research. Tethered cord syndrome is a stretch-induced disorder caused by an inelastic filum terminale anchoring the bottom of the spinal cord and limiting its normal movement. When the cord is abnormally fixed below, the entire neuraxis is under downward tension, and that tension can be transmitted all the way up to the hindbrain. Neurosurgical work by Milhorat and colleagues found that about 14% of CM-I patients had an associated tethered cord, with spinal cord traction considered one of the pathological mechanisms, and that children with a thickened or fatty filum showed greater tonsillar displacement. In selected cases, sectioning the filum terminale has allowed the tonsils to rise and the syrinx to resolve — direct evidence that downward traction can position the tonsils.
The same logic operates higher up. A separate model from Goel and colleagues proposes that, in many adults, atlantoaxial (C1–C2) instability is the primary driver, and the tonsils herniate as a protective response to mechanical pinching at the junction. Whether the tension originates at the bottom of the cord (filum) or at the top (an unstable, misaligned craniocervical junction), the unifying theme is the same: abnormal mechanical tension on the cord and its coverings can pull or displace the tonsils. This is why upper cervical clinicians take the upper neck seriously in Chiari, it's the upper anchor of that whole tension system.
Cervical curve loss: how a flattened neck adds cord tension
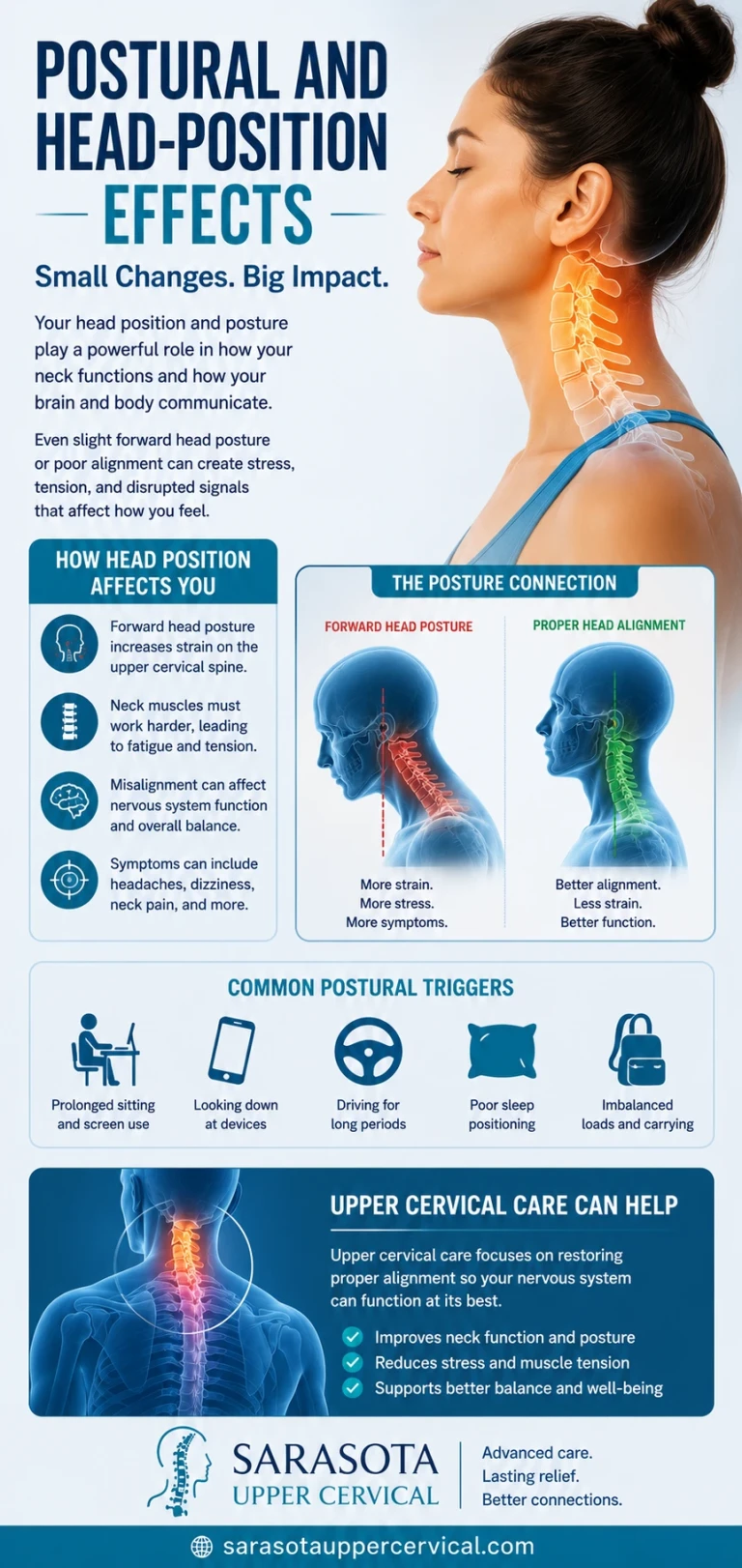
Here is where the upper cervical perspective ties trauma, tethering, and the neck together. A healthy cervical spine has a gentle forward curve (lordosis). When that curve flattens (hypolordosis) or reverses, the geometry of the spinal canal changes, and so does the length the spinal cord must travel.
The spinal cord is not infinitely slack. When the neck loses its curve and straightens, the canal effectively lengthens along its back wall, and the cord and its dural covering are placed under increased longitudinal tension. This is the cord-tethering effect of curve loss: a literature review citing Henderson describes how "tethering" of the spinal cord occurs as a result of abnormal stresses from biomechanical changes of the cervical spine, creating local stenosis and abnormal shearing and strain within the cord's axons. Put simply: a flattened or reversed cervical curve stretches the cord — and that added upward-and-downward strain is precisely the kind of tension the tethering model says can influence tonsillar position.
Loss of cervical lordosis is one of the most common consequences of whiplash and head/neck trauma. So the sequence becomes coherent: an injury damages the upper neck, the protective curve flattens, the cord and dura come under increased tension, and in a person whose tonsils already sit at a borderline level, that mechanical change may contribute to symptom onset or worsening. None of this means the curve "caused" the Chiari — but it offers a plausible mechanical reason why two people with identical tonsillar measurements can feel completely different.
The myodural bridge: a physical cable between neck muscle and the cord's covering
There's a specific anatomical structure that makes the upper neck's influence on this system more direct than its small size suggests — the myodural bridge.
The myodural bridge is a band of connective tissue that physically connects the deep suboccipital muscles — chiefly the rectus capitis posterior minor, along with the rectus capitis posterior major and obliquus capitis inferior — to the dura mater, the membrane enveloping the spinal cord and brainstem. It is a literal mechanical cable between muscle and the cord's covering at the exact level of the craniocervical junction. The same research notes that whiplash-type hyperflexion-extension injuries transmit traction forces straight through this bridge to the cervical dura, and that the bridge participates in the normal pumping of cerebrospinal fluid with head movement.
This is the connection that ties the whole article together — and recent research makes it explicit for Chiari specifically. Studies have reported that the rectus capitis posterior minor, the principal myodural bridge muscle, undergoes degeneration in Chiari patients: patients with rectus capitis posterior minor damage from cervical whiplash injury have a significantly increased probability of developing CM-I, and some previously asymptomatic CM-I patients developed symptoms after whiplash-like injuries without any increase in the degree of tonsillar herniation. Read that last part again: symptoms appeared and worsened without the tonsils moving — meaning the change was in the soft tissue, the muscle, the dural tension, and the CSF dynamics, not in the malformation's measurement. That's a strong signal that the upper neck's mechanical state, not just the millimeters of descent, drives how a person feels.
Proprioceptive mismatch, muscle imbalance, and the feedback loop
The suboccipital muscles aren't just mechanical cables — they're sensory organs. They carry one of the highest densities of muscle spindles in the body, constantly reporting head position to the brainstem's balance centers. After a neck injury, those muscles often settle into a chronically unbalanced state — short and tight on one side, lengthened on the other — feeding asymmetric, inaccurate position signals into the same brainstem region the Chiari is already crowding.
This creates a self-reinforcing problem. Injury flattens the curve and unbalances the suboccipital muscles. The unbalanced muscles pull asymmetrically through the myodural bridge on the dura and feed distorted proprioceptive signals to a brainstem that's already mechanically stressed. The distorted signals and altered tone help hold the neck in its faulty, curve-flattened posture, which sustains the cord tension. Each piece keeps the others in place — which is part of why post-traumatic craniocervical symptoms so often become chronic and resistant to treatments aimed only at the tonsils.
Dr. Scott Rosa and the craniocervical junction imaging research
Much of the modern interest in the neck–Chiari relationship traces to imaging work at the craniocervical junction, where Dr. Scott Rosa is among the most recognized names. Rosa is a co-author of a peer-reviewed book chapter, "Craniocervical Junction Syndrome: Anatomy of the Craniocervical and Atlantoaxial Junctions and the Effect of Misalignment on Cerebrospinal Fluid Flow," which examines how misalignments of the upper cervical junction can disturb CSF flow and contribute to neurological signs and symptoms.
A central theme of this work is that position matters. Standard MRI is performed lying down, but the tonsils and CSF dynamics behave differently under the full weight of the head. Rosa's research uses upright, weight-bearing MRI because, as the FONAR-published work describes, only upright imaging can visualize the craniocervical junction in the fully weight-loaded position needed to detect fully distended cerebellar tonsillar ectopia and CSF-flow-impeding misalignments. A Chiari that looks borderline lying down can look meaningfully different standing up — which helps explain symptomatic patients whose recumbent scans were called "mild."
Rosa's broader contributions include co-authoring a case-control study on cerebellar tonsillar ectopia and head/neck (whiplash) trauma published in Brain Injury in 2010, and developing imaging-guided protocols for assessing the junction before and after upper cervical correction. It's important to characterize this honestly: this body of work consists largely of imaging studies, case series, and hypothesis-generating research rather than large randomized trials, and it remains an area of active investigation and debate. It is best understood as a compelling mechanical framework — not as settled proof that upper cervical care changes Chiari outcomes.
Where upper cervical care fits — and where it doesn't
To be unambiguous: a Chiari malformation is a structural neurological condition. It is diagnosed by MRI, managed by neurologists and neurosurgeons, and in some cases requires surgery (posterior fossa decompression). Upper cervical chiropractic does not decompress the foramen magnum, does not move the cerebellar tonsils, and does not cure the malformation. Any clinician or article claiming otherwise is overstating the evidence.
What focused upper cervical care can reasonably address is the mechanical environment of the craniocervical junction: the alignment and motion of C1 and C2, the cervical curve, suboccipital muscle balance, and the proprioceptive input feeding the brainstem. The working hypothesis — supported by the tethering, curve-loss, myodural bridge, and CCJ-imaging research above — is that for some patients, improving that mechanical environment may reduce the secondary tension and dysfunction layered on top of the underlying anatomy. Some people with Chiari-region symptoms find that addressing an upper cervical injury helps how they feel, even though the malformation itself is unchanged.
At Sarasota Upper Cervical, our role is to evaluate that mechanical picture carefully — using precise upper cervical analysis and, where appropriate, advanced imaging such as cone beam CT (CBCT) to understand the three-dimensional position of the atlas and axis — and to work alongside your medical team, never in place of it. If you have a known or suspected Chiari, neurological evaluation comes first.
Questions and Answers
Can upper cervical chiropractic cure my Chiari malformation?
Aquired chiari malformation cases do well under upper cervical chirorpactic care. It is not a cure all but the relief and quality of life changes for these patients is significant.
What's the difference between congenital and acquired Chiari?
Congenital Chiari is generally attributed to a posterior fossa that's too small from birth, crowding the brain downward. Acquired Chiari develops later from another cause — trauma, instability of the upper neck, changes in CSF pressure, or downward cord tension — in someone who didn't previously have tonsillar descent. The acquired form is where the upper cervical connection is most relevant, because the upper neck is a mechanical variable that can change over time.
I had a car accident and now I have Chiari symptoms. Is that connected?
It may be. A frequently cited analysis found roughly a quarter of symptomatic patients linked their onset to trauma, most often whiplash. Research also shows that some previously asymptomatic Chiari patients became symptomatic after whiplash-type injuries without any increase in tonsillar herniation — meaning the change was in the neck's soft tissue, muscle, and fluid dynamics. A whiplash history is one of the strongest reasons to have the upper neck evaluated mechanically, in addition to your neurological workup.
How does losing my neck curve relate to Chiari?
A flattened or reversed cervical curve lengthens the back wall of the spinal canal and increases longitudinal tension on the spinal cord and its dural covering. Because the tethering model holds that downward/longitudinal cord tension can influence tonsillar position and symptoms, restoring or supporting a healthier curve is a plausible way to reduce that mechanical strain — though it does not change the malformation itself.
What is the myodural bridge, and why does it matter here?
It's a connective-tissue cable linking the deep suboccipital muscles directly to the dura surrounding the spinal cord and brainstem, right at the craniocervical junction. Whiplash forces transmit through it to the dura, and the main muscle involved (rectus capitis posterior minor) has been shown to degenerate in Chiari patients. It's the anatomical reason a neck injury can affect dural tension and CSF dynamics at the exact level of a Chiari.
Why do you recommend upright MRI or CBCT instead of regular imaging?
Standard MRI is done lying down, but the tonsils and CSF flow behave differently under the head's full weight. Upright, weight-bearing MRI — central to Dr. Scott Rosa's craniocervical junction research — can reveal tonsillar descent and flow obstruction that a recumbent scan underestimates. CBCT, meanwhile, gives a precise 3D picture of the atlas and axis position to guide an accurate upper cervical analysis. Different tools answer different questions.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Chiari malformation is a structural neurological condition that must be diagnosed and managed by qualified medical professionals; upper cervical chiropractic does not treat, correct, or cure Chiari malformation and is intended only to address the biomechanics of the craniocervical junction as a complement to medical care. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization is made or implied. The mechanisms and research described — including work on acquired Chiari, cord tethering, cervical curve loss, the myodural bridge, and craniocervical junction imaging — represent emerging and in some cases debated areas of science, and are presented for education rather than as proof of treatment outcomes. Individual results vary, and no specific outcome is guaranteed. Always consult your physician, neurologist, or neurosurgeon regarding diagnosis and treatment of Chiari malformation or any neurological symptoms.



Leave a comment