
Some POTS patients drink water constantly, add salt to everything, and still feel like they're running on empty. That pattern often points to a specific, well-studied subtype: hypovolemic POTS, where the fundamental problem is a genuine deficit in circulating blood volume, and, strangely, a hormone system that should be fixing that deficit but isn't. This guide explains the mechanism behind hypovolemic POTS, why the body's usual fix for low blood volume fails to kick in, and where the brainstem and upper cervical spine plausibly factor into a condition rooted largely in kidney hormone regulation.
The Core Problem: Not Enough Blood to Go Around
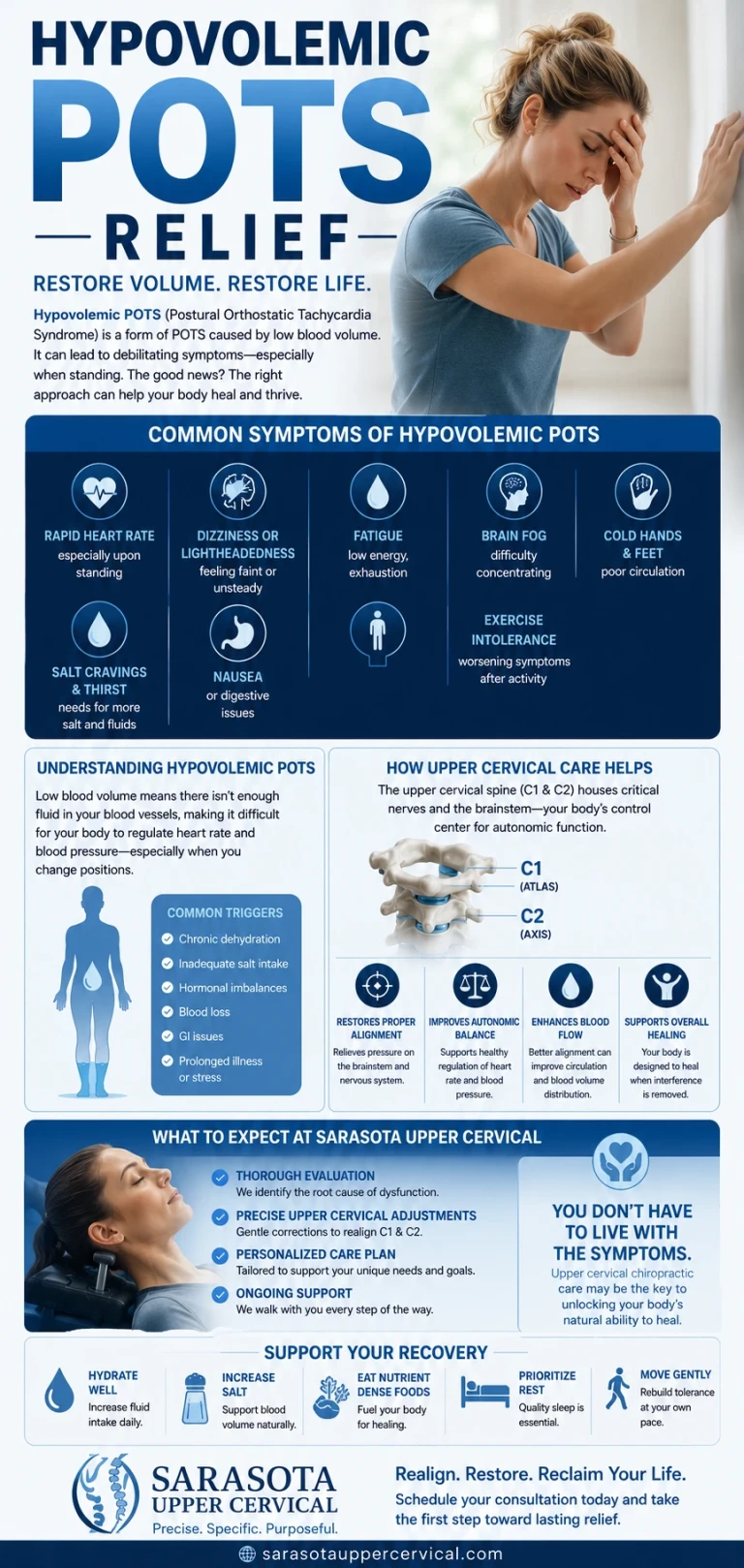
Research has consistently found that a substantial share of POTS patients have measurably lower blood volume than healthy people of the same size, with one well-controlled study finding an overall deficit of roughly 13%, affecting both plasma volume and red blood cell volume. When there isn't enough circulating blood to fill the vascular system, standing up creates an immediate problem: not enough blood returns to the heart, cardiac output drops, and the heart compensates by beating faster, the hallmark tachycardia that defines POTS.
Schedule Your Appointment
Schedule appointmentThe Renin-Aldosterone Paradox
Here's what makes hypovolemic POTS particularly strange, and particularly well documented. In a healthy person, low blood volume should trigger the kidneys to release more renin, which converts to angiotensin and stimulates the adrenal glands to release aldosterone, a hormone that tells the kidneys to hold onto sodium and water, expanding blood volume back toward normal. It's a textbook feedback loop.
In a landmark 2005 study published in Circulation, researchers measured this system directly in POTS patients and found the loop simply wasn't working. Despite a clear, measurable deficit in plasma and red blood cell volume, plasma renin activity remained unchanged from healthy controls, and aldosterone levels were, if anything, paradoxically low. The researchers termed this the renin-aldosterone paradox: the exact hormonal response that should be correcting the low blood volume is essentially absent, leaving the deficit uncorrected and the body stuck compensating with a faster heart rate instead.
Recognizing the Hypovolemic Pattern

Rapid heart rate on standing -that responds noticeably, at least temporarily, to aggressive fluid and salt loading
Profound, heavy fatigue, often described as feeling drained rather than wired or anxious
Poor response to standing that improves somewhat with compression garments, which mechanically compensate for the volume the body isn't holding onto on its own
A history of post-viral onset in some patients, with infections including COVID-19 and Epstein-Barr virus identified as potential triggers for this pattern, sometimes through autoimmune mechanisms affecting the kidney's hormonal regulation
Formal diagnosis of true hypovolemia requires specialized blood volume analysis, historically limited to select centers, though newer, more accessible techniques such as CO-rebreathing have been validated as alternatives. A RAAS panel, measuring plasma renin activity and serum aldosterone, can help confirm the characteristic paradox even when direct blood volume measurement isn't available, though it isn't diagnostic on its own.
Where the Brainstem and Upper Cervical Spine Enter the Picture
The primary abnormality in hypovolemic POTS is hormonal and renal: a breakdown in the feedback loop between blood volume, renin, and aldosterone. Upper cervical chiropractic does not correct kidney hormone regulation directly, and it does not replace fluid, salt, or medication strategies aimed at expanding blood volume. That said, there's a plausible, indirect mechanism worth understanding.
Renal sympathetic tone and brainstem control
The kidney's release of renin is not purely a local, autonomous process, it's influenced by renal sympathetic nerve activity, and the central command for that sympathetic outflow originates in specific brainstem nuclei. If the craniocervical junction, the region formed by the atlas (C1) and axis (C2) directly beneath the brainstem, is mechanically compromised, the resulting irritation to brainstem autonomic centers may plausibly influence the sympathetic signaling that helps regulate renal renin release, layered on top of, not as a replacement for, whatever is separately driving the underlying RAAS dysfunction.
Proprioceptive aberrancy and autonomic strain
The suboccipital region carries an unusually high density of proprioceptive receptors feeding constant positional information to the brainstem. When the atlas is misaligned, this input can become distorted, a phenomenon called dysafferentation, adding a layer of sensory noise to a brainstem already managing a body that cannot maintain adequate blood volume on its own. Whether this measurably worsens hypovolemic POTS specifically has not been directly studied, but the underlying anatomical relationship is well established.
The myodural bridge
The suboccipital muscles connect directly to the dura mater surrounding the brainstem via myodural bridges. Chronic tension in this area, often following whiplash or repetitive postural stress, may contribute low-grade mechanical irritation to brainstem regions involved in broader autonomic and cardiovascular regulation.
What Atlas Correction May and May Not Do Here
To be unambiguous: upper cervical chiropractic does not treat, cure, or reverse hypovolemic POTS, does not correct the renin-aldosterone paradox directly, and does not replace fluid loading, compression garments, or medications aimed at blood volume expansion. What a focused upper cervical evaluation addresses is the mechanical environment of the craniocervical junction and its relationship to brainstem-level autonomic regulation. For appropriately evaluated patients, particularly those with a relevant trauma history, addressing that mechanical layer may help reduce additional autonomic strain, alongside, never in place of, medical management of blood volume and RAAS function.
Questions and Answers
Related article

Upper Cervical Chiropractor Sarasota, Bradenton, Venice and Tampa Bay Area
Nov 15, 2021
How much blood volume deficit is typical in hypovolemic POTS?
Research has found an average deficit of roughly 13%, affecting both plasma volume and red blood cell volume, though this varies between individuals and not all POTS patients show this pattern.
What is the renin-aldosterone paradox?
It's the finding, first well documented in a 2005 study, that POTS patients with clear blood volume deficits fail to show the expected compensatory rise in renin and aldosterone, the hormones that would normally correct low blood volume. The mechanism preventing this compensatory response remains an active area of research.
Can post-viral illness cause hypovolemic POTS?
Some patients develop hypovolemic POTS symptoms following viral infections, including COVID-19 and Epstein-Barr virus, potentially through autoimmune mechanisms affecting the hormonal systems that regulate blood volume, though this connection is still being actively studied.
Does upper cervical chiropractic fix the renin-aldosterone paradox?
No. Upper cervical chiropractic does not correct kidney hormone regulation or the renin-aldosterone paradox directly. Care in this area focuses on the biomechanics of the craniocervical junction and its relationship to brainstem autonomic regulation, which may be a contributing factor alongside, not instead of, the primary hormonal mechanism.
How is hypovolemic POTS diagnosed?
Formal diagnosis involves direct blood volume analysis, historically available only at specialized centers, or newer alternatives such as CO-rebreathing. A RAAS panel measuring renin and aldosterone can add supportive, though not independently diagnostic, information.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Hypovolemic POTS is a medical condition that must be diagnosed and managed by qualified medical professionals. Upper cervical chiropractic does not treat, correct, or cure hypovolemic POTS or any POTS subtype, and is intended only to address the biomechanics of the craniocervical junction as a complement to medical care. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization is made or implied. Individual results vary, and no specific outcome is guaranteed. Always consult your physician or autonomic specialist regarding diagnosis and treatment of POTS or any autonomic symptoms.



Leave a comment