
If you have numbness and tingling down your arm into your hand, aching in your shoulder, a heavy or "dead" feeling in the arm when you raise it, or symptoms that flare when you work at a keyboard or reach overhead, you may have been told you have thoracic outlet syndrome, or you may still be searching for an answer. Here's a piece of the puzzle that's often overlooked: the compression happens at the base of the neck, and what controls the muscles doing the compressing is the top of the neck. For many people, thoracic outlet syndrome isn't really a shoulder problem at all. Its root cause sits in the upper cervical spine.
This article walks through what thoracic outlet syndrome (TOS) actually is, why the scalene muscles and forward head carriage narrow the very space your nerves pass through, and,most importantly — how the upper neck acts as the master control center for postural muscle tone throughout the body. We'll cover the role of the suboccipital muscles, the myodural bridge, proprioception, the "double crush" concept, and how precise 3D imaging like cone beam CT (CBCT) fits into a thorough upper cervical evaluation. Throughout, one boundary stays clear: some forms of TOS are medical or surgical conditions, and upper cervical care focuses on the postural and mechanical contributors — it is not a cure-all.
Schedule Your Appointment
Schedule appointmentTo book a FREE consultation call 941 259-1891 or book here.
What thoracic outlet syndrome actually is
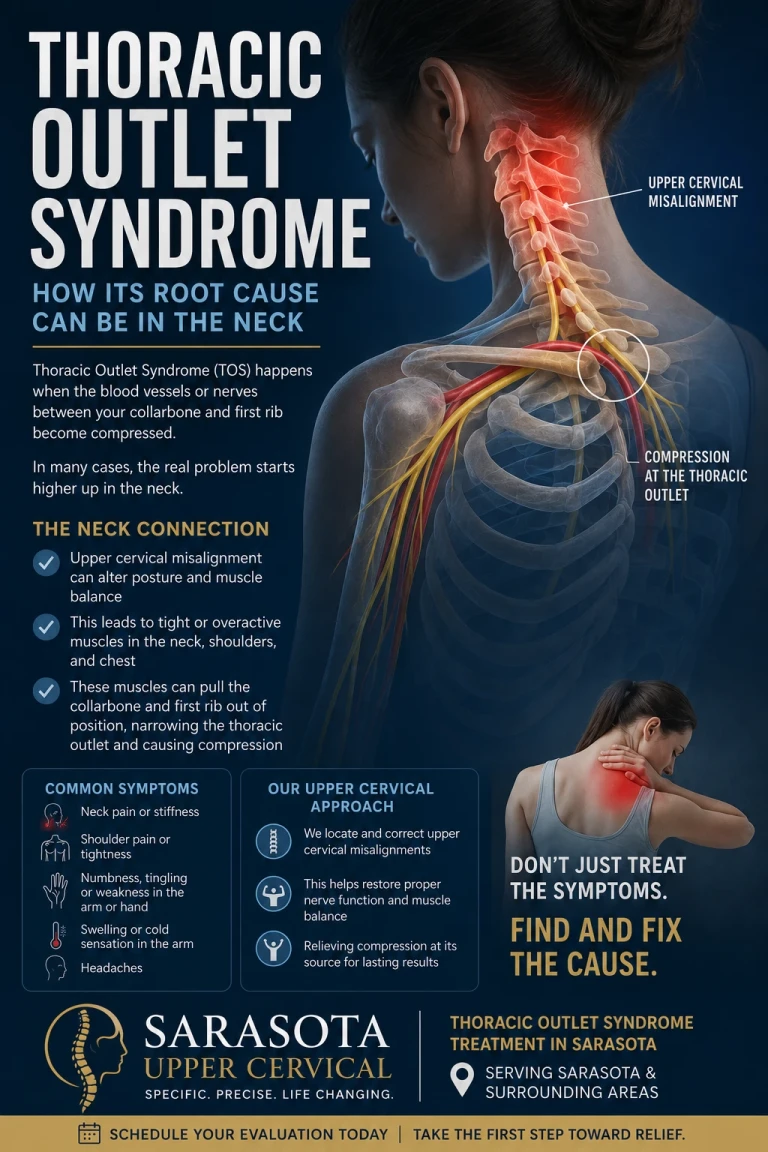
The "thoracic outlet" is the narrow corridor at the base of your neck where a bundle of nerves (the brachial plexus) and blood vessels travel from your neck and chest out toward your arm. When that corridor gets crowded, the nerves or vessels get compressed — and you feel it down the arm.
There are three types, and the proportions matter. Neurogenic TOS — compression of the brachial plexus nerves — accounts for roughly 95% of all cases, while arterial and venous (vascular) TOS make up the small remainder. This is important context: the overwhelming majority of TOS is a nerve-compression problem driven by the soft tissue and posture of the neck, not a blood-vessel emergency. Symptoms of the neurogenic form include pain, numbness, tingling, weakness, and a cold or fatigued feeling in the arm and hand, often worse with overhead activity.
The single most common site of compression is a small triangle in the neck. In neurogenic TOS, the brachial plexus is compressed between the scalene muscles of the neck and the first rib, and the condition is believed to result from traumatic or repetitive scalene muscle injury that narrows the scalene triangle. Hold onto that phrase: narrowing of the scalene triangle. Almost everything in this article comes back to what makes those scalene muscles tighten and that triangle close down.
The scalene triangle: where the neck squeezes the nerve
The brachial plexus and subclavian artery pass through the interscalene triangle, bordered by the anterior scalene muscle, the middle scalene muscle, and the upper surface of the first rib, and this triangle is the most common site for neural compression in TOS. The anterior and middle scalenes both originate from the transverse processes of the cervical vertebrae and descend to anchor on the first rib. That anatomy is the whole story in miniature: these are neck muscles, governed by neck mechanics, and the nerve threads right between them.
When the scalenes are chronically tight, hypertonic, or shortened, the triangle narrows and the nerve bundle gets pinched. When they're balanced and at a normal resting length, the corridor stays open. So the real clinical question isn't just "are the scalenes tight?" — it's "what is telling the scalenes to stay tight?" That answer leads straight up the neck.
Forward head carriage: the posture that closes the outlet
Picture the modern posture: head drifted forward over phones, keyboards, and steering wheels; shoulders rounded; chin poking ahead of the chest. This is forward head carriage, also known as military neck, and it is mechanically hostile to the thoracic outlet.
Related article

When the head moves forward of the shoulders, the deep neck muscles and the scalenes are recruited to hold the heavy head up against gravity. The scalenes shift from quiet postural stabilizers into constantly working muscles, becoming shortened and hypertonic. With forward head posture, the neck muscles stay tight and the cervical vertebrae are compressed, which can lead to impingement of the nerves both as they exit the spine and as they pass between the scalene muscles. The forward-head position also tips the first rib and collarbone into a more closed relationship, further shrinking the costoclavicular space the nerves and vessels travel through.
So forward head carriage narrows the outlet in two ways at once: it keeps the scalenes engaged and shortened (closing the scalene triangle), and it changes the bony geometry of the rib and clavicle (closing the costoclavicular space). The posture itself is a compression machine. And forward head carriage is rarely a "willpower" problem you can simply sit up straight to fix — it's usually driven by what's happening at the top of the neck.
The upper neck: master control center for postural muscle tone
Here's the part most TOS discussions miss entirely. The muscles that hold your posture — including the scalenes — don't decide their own tone in isolation. Their resting tension is set by a control system, and the headquarters of that system is the upper cervical spine.
The suboccipital muscles at the very top of the neck contain an unusually high density of muscle spindles — the sensory organs that report muscle length and movement. In fact the upper cervical spine holds one of the highest densities of proprioceptive receptors in the entire body, making it a key contributor to postural control and motor coordination. These tiny muscles aren't movers — they're sensors, constantly telling the brain where the head sits in space.
That information doesn't stay local. It drives reflexes that set muscle tone throughout the body. The cervical afferents feed three major reflex pathways — the cervico-collic reflex, the tonic neck reflex, and the cervico-ocular reflex — that translate head-and-neck position into coordinated muscle activation. The tonic neck reflex is precisely a system in which head position drives postural tone and stability in the limbs and trunk. In other words, the upper neck is wired to dictate how tight or relaxed your postural muscles are — including the scalenes that gate the thoracic outlet.
The core thesis: The scalenes that pinch your brachial plexus are downstream. The upper cervical spine is upstream. If the top of the neck is misaligned and sending faulty position signals, the reflex system can hold your scalenes and postural muscles in a chronically tightened, outlet-narrowing state — no matter how much you stretch them.
When the signal goes bad: proprioceptive mismatch and locked-in tone
Now connect injury to the control system. After a whiplash, fall, sports impact, or years of forward-head loading, the upper cervical joints can lose normal motion and position, and the suboccipital muscles settle into a chronically unbalanced state. When that happens, the high-density sensors at the top of the neck start sending distorted information.
This matters because the system is sensitive to it. Research shows that higher tone in the suboccipital muscles is significantly associated with a more forward head posture (a lower craniovertebral angle) — the faulty muscle state and the bad posture travel together. And experimental disturbance of neck proprioception measurably degrades balance and postural control, confirming that intact neck neuromuscular function is required to maintain normal standing posture. When the upper cervical signal is corrupted, the brain compensates by altering muscle tone across the postural chain — and a common compensation is to hold the head forward and keep the scalenes working overtime.
The result is a self-reinforcing loop. The upper cervical injury distorts proprioception → the reflex system raises postural muscle tone and pulls the head forward → forward head carriage keeps the scalenes shortened → the narrowed scalene triangle compresses the brachial plexus → and the resulting neck dysfunction and pain feed still more distorted signals back into the system. Stretching the scalenes or massaging the shoulder treats the bottom of the loop while the top keeps driving it. That's a major reason TOS is famously stubborn and recurrent.
The myodural bridge: a direct cable at the top of the chain
There's a specific anatomical structure that makes the upper neck's influence even more direct. The myodural bridge is a band of connective tissue physically connecting the deep suboccipital muscles — chiefly the rectus capitis posterior minor, to the dura mater, the membrane surrounding the spinal cord and brainstem. It's a literal mechanical link between the small muscles at the base of the skull and the covering of the central nervous system.
The same research notes that whiplash-type hyperflexion-extension injuries transmit traction forces through this bridge to the cervical dura, the exact mechanism behind so many post-trauma neck syndromes. For the TOS picture, the myodural bridge matters because it means tension and dysfunction at the very top of the neck are mechanically and neurologically coupled to the dura and the cord. The suboccipital region isn't just sending nerve signals that set scalene tone — through the bridge it's physically tugging on the neuromeningeal system that the entire brachial plexus is continuous with. The top of the neck and the outlet at the bottom are part of one connected mechanical system.
Double crush: two small compressions, one big problem
One more concept explains why the neck is so central. The "double crush" phenomenon describes how a nerve compressed at one point becomes more vulnerable to symptoms from a second, milder compression somewhere else along its length. The brachial plexus nerves originate at the cervical spine and then travel through the scalene triangle and outlet.
If a nerve root is already irritated where it exits an upper or mid cervical segment, and the same nerve is then mildly squeezed at the scalene triangle, the two modest compressions can sum into significant symptoms — even when neither alone would. This is why a careful evaluation looks at the whole cervical spine, not just the outlet. Major medical centers explicitly note that cervical spine disease and other nerve entrapments can mimic or coexist with TOS and must be sorted out. Addressing an upstream cervical contributor can change how much the downstream outlet compression actually bothers you.
The upper cervical approach in Sarasota, and where its limits are
Upper cervical chiropractic care focuses on the alignment and motion of the atlas (C1) and axis (C2), because that's the control point for the proprioceptive and reflex system that governs postural muscle tone. The goal isn't to force or "crack" the neck — it's to restore normal position and motion at the top of the cervical spine so the sensors there send accurate information again, allowing the reflex-driven postural tone (including scalene tone and head carriage) to normalize from the top down.
There's measurable support for the upstream effect. A randomized controlled trial found that upper cervical manipulation produced significant improvement in global postural-control measures — reducing sway velocity, surface, and path length on standing balance testing. That's direct evidence that what happens at the top of the neck changes postural control for the whole body — exactly the lever that forward head carriage and scalene tone sit on.
Why CBCT imaging matters here
Because the correction is precise, the analysis has to be precise. At Sarasota Upper Cervical we use cone beam computed tomography (CBCT) as a precision measurement tool — it shows the true three-dimensional position of the atlas and axis far more accurately than a flat 2D X-ray. A misalignment driving the postural cascade above may be only a few degrees of rotation or a small lateral shift, and the scalenes and head carriage respond to exactly that kind of subtle upper cervical positioning. CBCT lets us measure it in three dimensions and tailor the analysis to your individual anatomy, rather than guessing. (CBCT is a measurement and analysis tool, not a stand-alone diagnostic device for TOS — the diagnosis is clinical.)
The honest boundaries
Not all TOS is mechanical-postural. Some cases are driven by a cervical rib, an extra rib growing from the C7 vertebra, present in roughly 1–3% of people — or other bony anomalies that physically crowd the outlet; these often require medical or surgical management. Vascular TOS (arterial or venous compression) is a medical condition that needs prompt medical attention, especially if you have arm swelling, color changes, or coldness. And progressive muscle wasting or weakness in the hand is a red flag that warrants neurological evaluation. Upper cervical care is a complement to appropriate medical evaluation, not a replacement for it. A good upper cervical doctor will help identify whether your case has a postural-mechanical driver worth addressing — and will refer out when it doesn't.
Related article
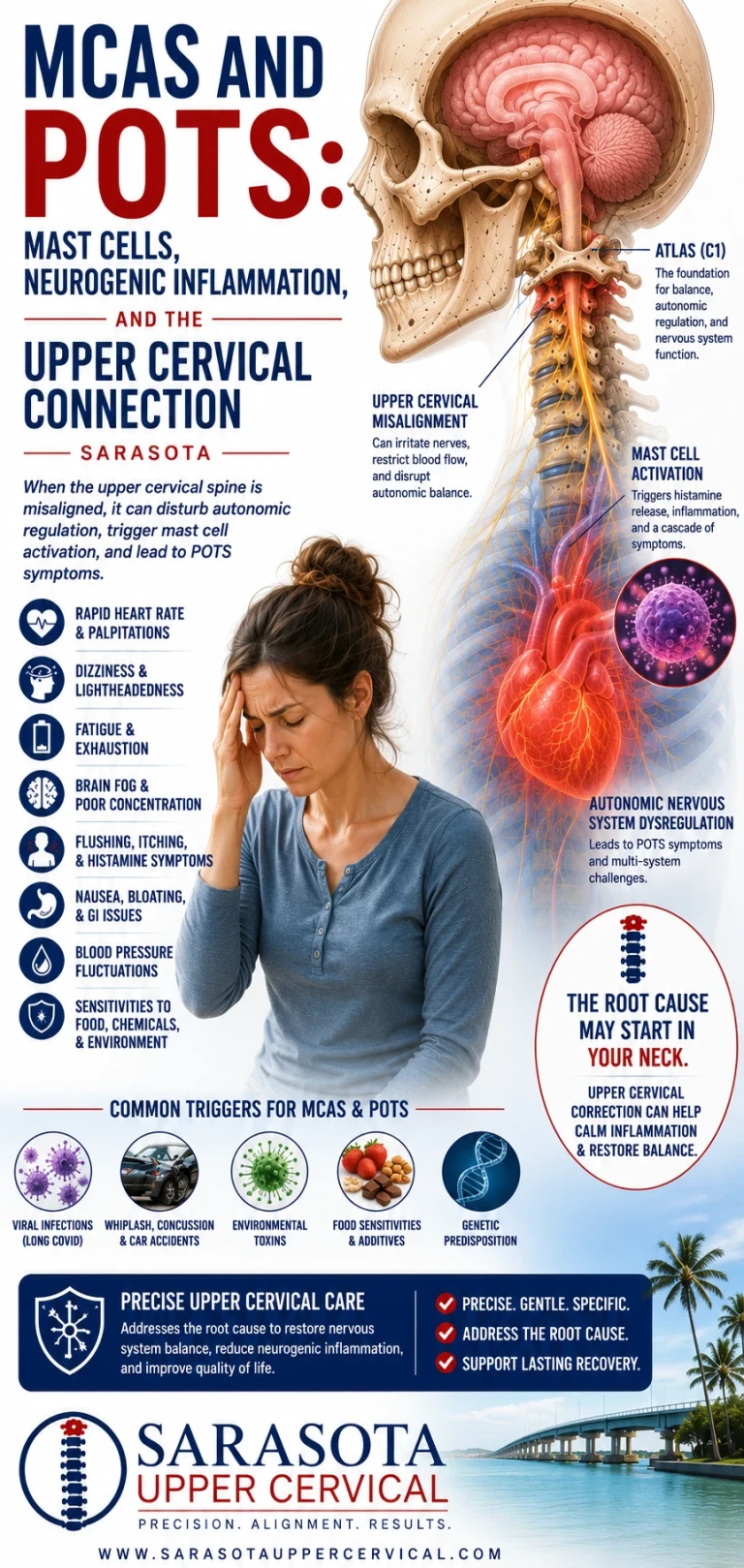
MCAS and POTS: Mast Cells, Neurogenic Inflammation, and the Upper Cervical Connection | Sarasota
Jul 28, 2026Questions and Answers
How can a problem at the top of my neck cause symptoms at the base of my neck and down my arm?
The top of the neck doesn't compress the nerve directly — it controls the muscles that do. The suboccipital region has one of the body's highest densities of position sensors, and through reflexes like the tonic neck reflex, it helps set postural muscle tone throughout the body, including the scalenes. When the upper neck sends faulty signals, the reflex system can hold your head forward and your scalenes tight, narrowing the outlet at the base of the neck where the nerve actually gets pinched.
I've been stretching my scalenes and it isn't helping. Why?
Because stretching addresses the bottom of the loop while the top keeps driving it. If the upper cervical spine is sending distorted proprioceptive input, the reflex system will keep re-tightening those scalenes no matter how often you stretch. Until the upstream signal normalizes, the muscle tone tends to return. That's a common reason TOS is so recurrent.
What's the connection between forward head posture and thoracic outlet syndrome?
Forward head carriage narrows the outlet two ways: it keeps the scalenes shortened and working to hold the heavy head up, closing the scalene triangle, and it tips the first rib and collarbone into a more closed position, shrinking the costoclavicular space. Both squeeze the nerves and vessels. And forward head posture is usually driven by upper cervical mechanics, not just habit.
What is the myodural bridge and why does it matter for TOS?
It's a connective-tissue cable linking the deep suboccipital muscles to the dura that surrounds the spinal cord. Whiplash forces transmit through it to the dura. For TOS, it means dysfunction at the very top of the neck is mechanically coupled to the neuromeningeal system the brachial plexus is continuous with — reinforcing that the top of the neck and the outlet are one connected system, not separate problems.
Do I still need to see a medical doctor?
Yes, particularly to rule out the forms that need medical care. Vascular TOS (with arm swelling, coldness, or color change), a cervical rib or other bony anomaly, and progressive hand weakness or muscle wasting all need medical or surgical evaluation. Upper cervical care addresses the postural-mechanical contributors and works alongside your medical team — it isn't a substitute for an appropriate diagnostic workup.
Why do you use CBCT instead of a regular X-ray?
CBCT shows the true 3D position of the atlas and axis, where a flat X-ray can only show two dimensions. The misalignments that drive postural tone are often a few degrees of rotation or a small shift, and seeing them accurately allows a precise, individualized analysis. We use it as a measurement and analysis tool; the TOS diagnosis itself remains clinical.
Thoracic outlet syndrome treatment in Sarasota
If you have arm numbness, tingling, or weakness that hasn't resolved, especially after a neck injury or years of desk and device posture — a focused upper cervical evaluation can help determine whether the root driver is at the top of your neck, working alongside your medical care.
Request a Consultation-941 259-1891
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Thoracic outlet syndrome has neurogenic and vascular forms; vascular TOS, cervical rib and other bony anomalies, and progressive neurological deficits require medical or surgical evaluation, and upper cervical chiropractic care is intended to address postural and mechanical contributors as a complement to appropriate medical care, not as a cure or a replacement for it. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization or superiority is made or implied. Cone beam CT is used as a precision measurement and analysis tool, not as a stand-alone diagnostic device. The mechanisms and research described are presented for education; individual results vary, and no specific outcome is guaranteed. Always consult a qualified healthcare provider regarding diagnosis and treatment of thoracic outlet syndrome or any neurological symptoms.



Leave a comment