
"Chiari malformation" isn't one single condition — it's a spectrum, ranging from a mild, often incidental finding to a severe structural problem present from birth. Getting the type right matters, because it shapes everything from what symptoms to expect to whether surgery is ever on the table. This guide walks through each recognized type, and pays particular attention to one category that's directly relevant to upper cervical care: acquired Chiari, where tonsillar position can change later in life, sometimes tied to the mechanics of the upper neck itself.
How Chiari Malformation Is Classified
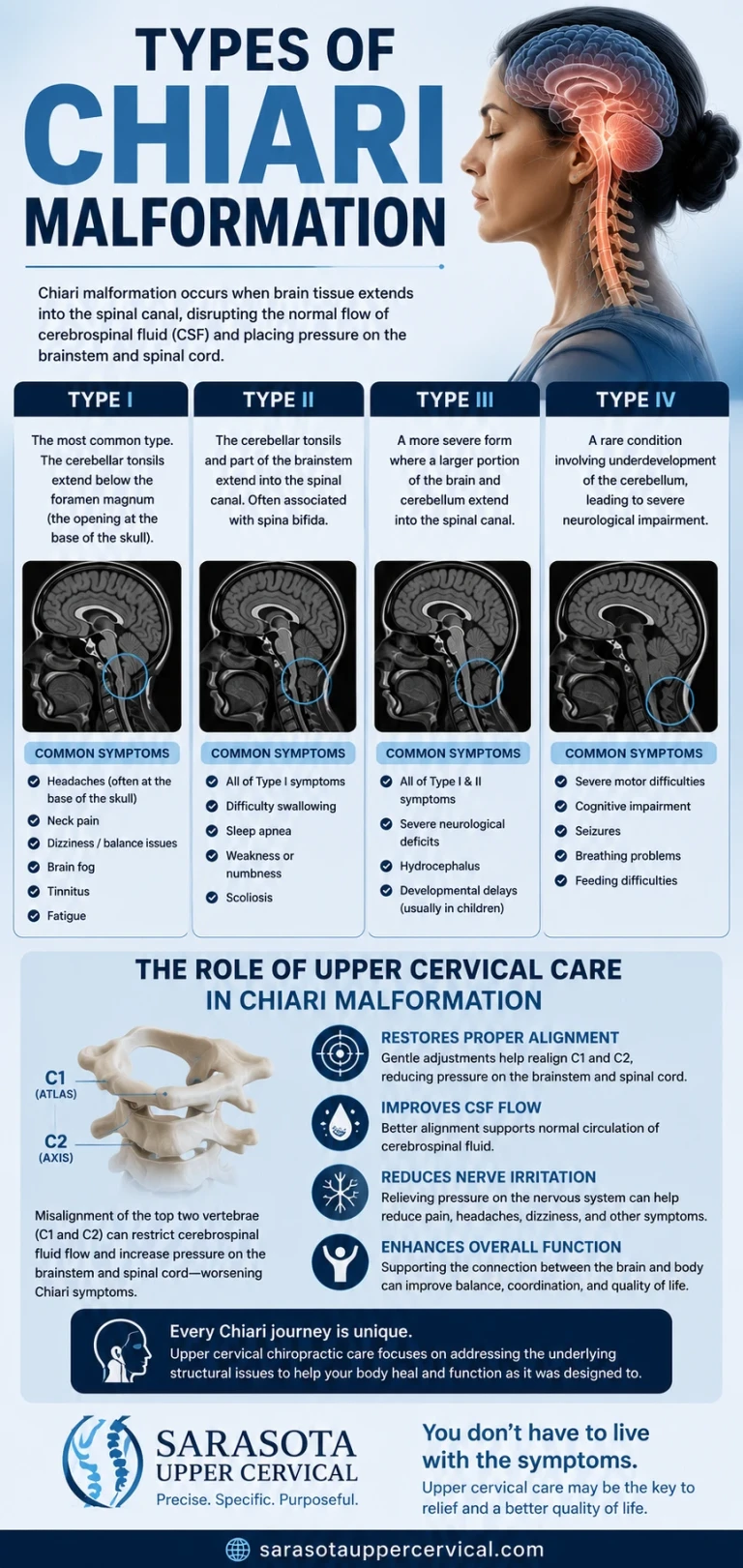
All Chiari types describe some degree of the cerebellum, brainstem, or fourth ventricle extending into or through the foramen magnum, the opening at the base of the skull where the brainstem transitions into the spinal cord. What differs between types is how much tissue is involved, how it got there, and how severe the associated findings tend to be.
Schedule Your Appointment
Schedule appointmentChiari Type 0
The mildest and least understood category. In Chiari 0, the cerebellar tonsils sit in a normal position, with little to no descent, yet a person has a syrinx (a fluid-filled cavity in the spinal cord) along with symptoms otherwise typical of Chiari. It's generally thought to reflect abnormal cerebrospinal fluid (CSF) flow dynamics at the foramen magnum without frank crowding by the tonsils themselves.
Chiari Type 1 (the most common type)
Chiari type I (CM-I) is defined by downward displacement of the cerebellar tonsils of 5 millimeters or more below the foramen magnum, measured on midsagittal MRI. Extension of 3 millimeters or less is considered a normal variant, and 3–5 millimeters is considered borderline. CM-I is frequently discovered incidentally, can remain silent for life, and when symptomatic, most often presents in later childhood through adulthood with the classic cough-triggered occipital headache, along with neck pain, dizziness, and the wider symptom list common to this condition. Syringomyelia, a fluid cavity within the spinal cord, coexists in a substantial share of CM-I cases.
Chiari Type 1.5
Considered a progression of Type 1, Chiari 1.5 involves not just the cerebellar tonsils but also a portion of the brainstem extending into the foramen magnum. Because brainstem tissue itself is involved, this type is generally associated with a somewhat more severe symptom profile than straightforward Type 1, and clinical series have found headaches and neck pain to be the most prevalent presenting complaints in this group.
Related article
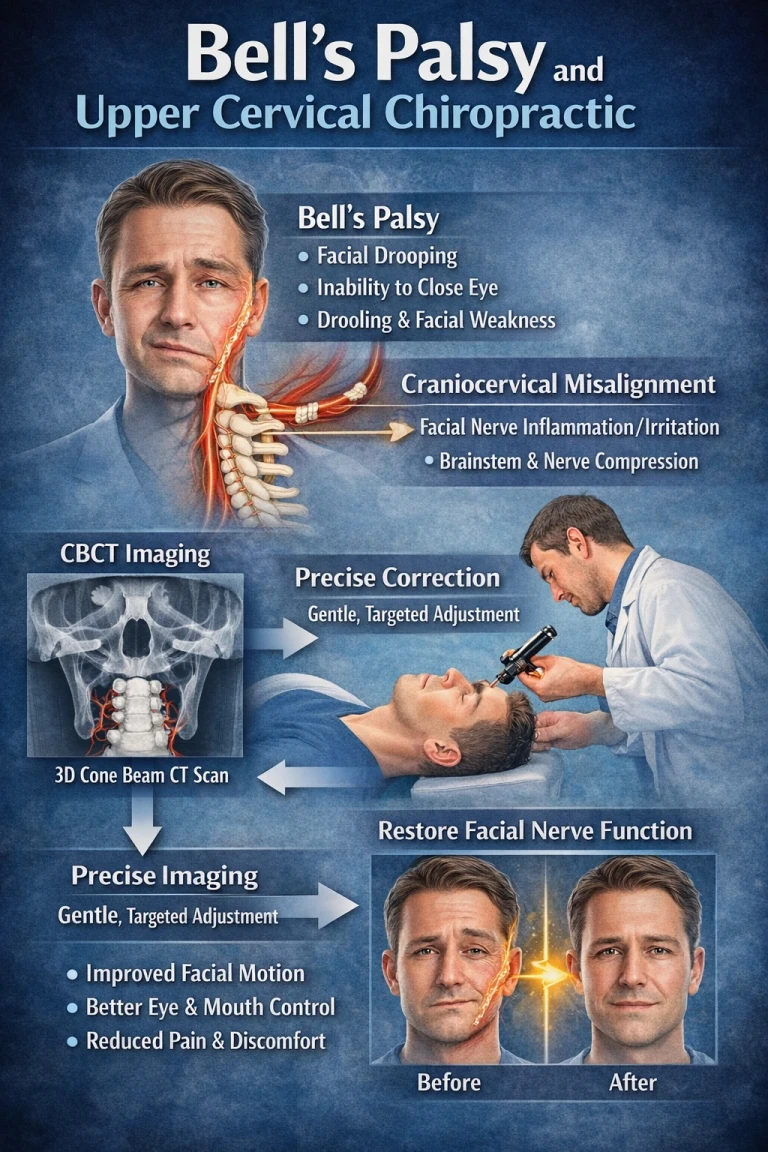
Bell’s Palsy Treatment in Sarasota & Bradenton | Upper Cervical Chiropractor Sarasota and Lakewood
Mar 18, 2026Chiari Type 2
A more severe, congenital form in which the cerebellar vermis, brainstem, and fourth ventricle (a fluid-filled cavity deep in the brain) are all displaced and compressed. Chiari 2 is almost always associated with spina bifida (specifically myelomeningocele) and is frequently accompanied by hydrocephalus, a disruption of normal CSF circulation within the brain's ventricles. This type is typically identified early, often prenatally or in infancy, given its association with spinal defects.
Chiari Types 3 and 4
Rare and severe forms. Type 3 involves herniation of posterior fossa contents into a skull or upper spinal defect (an occipital encephalocele) and carries a serious prognosis. Type 4 describes an underdeveloped or absent cerebellum and is exceedingly rare.
Acquired Chiari: The Type That Changes the Conversation
The traditional view of Chiari has always centered on a posterior fossa (the bony compartment housing the cerebellum) that's simply too small for the brain it contains from birth, pushing the tonsils downward. That model is real and well established for a large share of cases. But it is not the whole picture, and it's the piece most often left out of patient-facing explanations.
The medical literature clearly recognizes a distinct category: acquired Chiari, tonsillar descent that develops in someone who did not have it before, driven by something other than a congenitally small posterior fossa. Huang's 1994 paper formally describing acquired Chiari I was a turning point in this understanding, and documented cases since have described patients with a completely normal brain MRI at birth who later developed measurable tonsillar descent. Recognized causes include conditions that raise pressure above the tonsils and pull them downward, as well as mechanical instability or trauma at the craniocervical junction itself. One frequently cited analysis found that roughly a quarter of symptomatic patients identified trauma, most commonly whiplash from a motor vehicle accident or a direct blow to the head and neck, as the precipitating event behind their symptom onset.
This matters enormously for how the upper cervical spine fits into the picture: if tonsillar position and symptom severity can change after an injury to the neck, then the mechanical state of the upper cervical spine, specifically the atlas (C1) and axis (C2), is a legitimate variable worth evaluating, not an unrelated afterthought.
The Mechanical Models Behind Acquired and Worsening Chiari
Cord tethering and traction
One of the most well-supported mechanical theories holds that the cerebellar tonsils don't simply fall, they get pulled. Tethered cord research has found that an inelastic filum terminale anchoring the bottom of the spinal cord can place the entire neuraxis under downward tension, transmitting all the way up to the hindbrain; in selected surgical cases, releasing that tension has allowed the tonsils to rise. A separate model, from Goel and colleagues, proposes that in many adults, instability at the C1–C2 (atlantoaxial) junction is itself the primary driver, with tonsillar herniation occurring as a protective response to mechanical pinching at that junction. Whether the tension originates at the bottom of the cord or the top, the unifying idea is the same: abnormal mechanical tension on the spinal cord and its coverings can influence tonsillar position.
Cervical curve loss ("straight neck syndrome")
A healthy cervical spine holds a gentle forward curve. When that curve flattens or reverses, a pattern often called straight neck syndrome, the geometry of the spinal canal changes and effectively lengthens along its back wall, placing the spinal cord and dura under increased longitudinal tension, the same kind of tension the tethering model implicates in tonsillar position. Loss of cervical curve is one of the most common consequences of whiplash and head or neck trauma, which helps explain a coherent sequence: an injury damages the upper neck, the protective curve flattens, the cord comes under increased tension, and in a person whose tonsils already sit at a borderline position, that mechanical change may contribute to new or worsening symptoms.
The myodural bridge
The deep suboccipital muscles, chiefly the rectus capitis posterior minor, are physically connected to the dura mater via connective tissue bridges called myodural bridges, right at the level of the craniocervical junction. Whiplash-type injury transmits force through this bridge directly to the dura, and research has found that the rectus capitis posterior minor undergoes degeneration in Chiari patients specifically, with whiplash-related damage to this muscle associated with a significantly increased likelihood of Chiari-related findings. Notably, some previously asymptomatic Chiari patients became symptomatic after a whiplash-type injury with no corresponding increase in the degree of tonsillar herniation, meaning the change occurred in the soft tissue and dural tension rather than the malformation's measured size.
Proprioceptive aberrancy
The suboccipital muscles double as sensory organs, carrying an unusually high density of muscle spindles that continuously report head position to the brainstem's balance centers. Following injury, these muscles often become chronically unbalanced, tight on one side, lengthened on the other, feeding distorted, asymmetric signals into a brainstem region that, in Chiari, may already be mechanically crowded. This creates a self-reinforcing pattern: injury flattens the cervical curve and unbalances the suboccipital muscles, the unbalanced muscles feed distorted signals and altered dural tension back into an already-stressed brainstem, and the distorted signals help sustain the very posture that's keeping cord tension elevated.
How Atlas Correction Fits Into the Acquired Chiari Picture
It bears repeating clearly: upper cervical care does not treat, correct, or cure any type of Chiari malformation. It does not move the cerebellar tonsils and does not decompress the foramen magnum. What a focused upper cervical evaluation addresses is the mechanical environment surrounding the craniocervical junction, atlas and axis alignment, cervical curve, and suboccipital muscle balance, particularly relevant in cases where trauma or instability appears to have played a role in symptom onset. For appropriately evaluated patients, addressing that mechanical layer may help reduce some of the secondary irritation contributing to symptoms, working alongside, never in place of, ongoing neurological care.
Related article
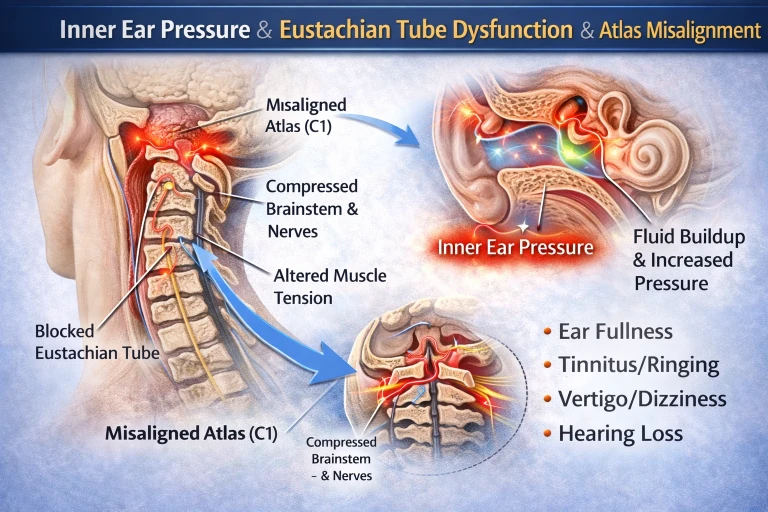
Ear Pressure Relief Sarasota | Eustachian Tube Dysfunction Lakewood Ranch
Mar 04, 2026Questions and Answers
What's the difference between Chiari Type 1 and Type 1.5?
Type 1 involves descent of the cerebellar tonsils alone below the foramen magnum. Type 1.5 involves both the tonsils and a portion of the brainstem, and is generally considered a progression of Type 1 with a somewhat more significant symptom profile.
Is acquired Chiari the same as congenital Chiari?
No. Congenital Chiari is typically attributed to a posterior fossa that is too small from birth. Acquired Chiari develops later in someone who did not previously have tonsillar descent, driven by another cause such as trauma, instability of the upper cervical spine, or changes in CSF pressure.
Can a car accident or whiplash actually cause a Chiari malformation?
Trauma is one of the most commonly cited precipitating factors for acquired or newly symptomatic Chiari, with roughly a quarter of symptomatic patients in one frequently cited analysis identifying trauma, most often whiplash, as the trigger. Research has also documented symptom onset after whiplash-type injury without any measurable increase in tonsillar herniation, suggesting soft tissue and dural tension changes rather than a newly created malformation in most such cases.
Does Chiari Type 2 relate to the upper cervical spine the same way Type 1 does?
Type 2 is a congenital condition strongly associated with spina bifida and is generally identified very early in life; the mechanical, trauma-related models discussed here are most relevant to Type 1, Type 1.5, and acquired Chiari rather than Type 2 or the rarer Types 3 and 4.
Should everyone with tonsillar descent on an MRI have upper cervical care?
Not necessarily. Many people with measurable tonsillar descent have no symptoms at all. An upper cervical evaluation is most relevant for symptomatic patients, particularly those with a history of neck trauma, instability, or a cervical curve that has flattened or reversed, and should always occur alongside, not instead of, appropriate neurological evaluation.
This article is for general educational purposes only and is not medical advice, a diagnosis, or a treatment recommendation for any individual. Chiari malformation is a structural neurological condition that must be diagnosed and managed by qualified medical professionals. Upper cervical chiropractic does not treat, correct, or cure any type of Chiari malformation and is intended only to address the biomechanics of the craniocervical junction as a complement to medical care. Upper cervical chiropractic is an area of focus within chiropractic; it is not a board-recognized specialty, and no claim of specialization is made or implied. The mechanisms and research described, including acquired Chiari, cord tethering, cervical curve loss, and the myodural bridge, represent emerging and in some cases debated areas of science, and are presented for education rather than as proof of treatment outcomes. Individual results vary, and no specific outcome is guaranteed. Always consult your physician, neurologist, or neurosurgeon regarding diagnosis and treatment of Chiari malformation or any neurological symptoms.



Leave a comment